
Abstract
Intra-oral ligation of the ducts from both the parotid and submandibular glands is commonly offered to patients with severe sialorrhea, often when medical therapy fails to achieve adequate salivary control. The submandibular glands function to provide approximately 70% of the resting salivary output. 1 The parotid glands function in a demand-response fashion when stimulated by a variety of sensory information. 1 Four-duct ligation is a frequently performed procedure with an intra-oral approach that requires minimal operative time. 2,3 When this procedure fails to provide adequate control of salivary flow, other surgical procedures and medical therapies are considered.
Duct-ligation procedures have not been well examined in terms of their long-term efficacy. Two recent studies reported follow-up of 13 and 14 months respectively, 2,3 and found decreases in salivary flow and aspiration pneumonia with no occurrences of xerostomia and no postoperative complications. What the studies lacked was long-term follow-up of this persistent disease process.
The aim of this review is to critically evaluate our experience with intra-oral duct ligation procedures to determine whether severe drooling, quantified and evaluated preoperatively, is improved in measurable ways. We also sought to characterize patient and caregiver satisfaction with duct ligation, to detect patient morbidity, and to further therapy required for control of drooling.
METHODS
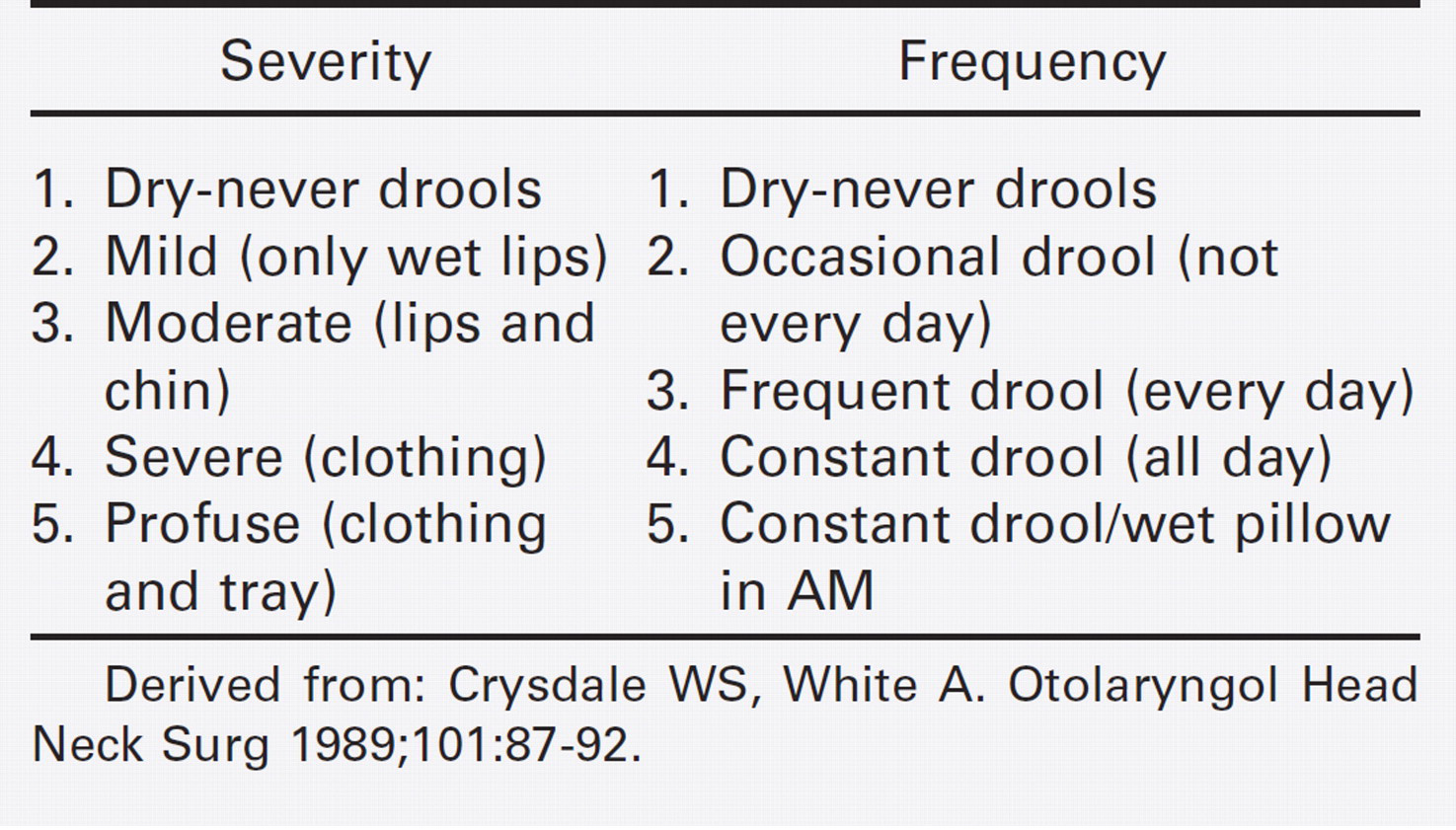
After IRB approval was received, a retrospective chart review was performed of all children who had undergone salivary duct ligation procedures as described by Klem and Mair 3 between 1999 and 2003 to assess the postoperative control of sialorrhea. Surgical therapy in our population included 4-duct ligation (submandibular and parotid), submandibular duct ligation alone, and 3-duct ligation (bilateral submandibular and unilateral parotid duct). The surgery of choice was based solely on caregiver preference. The time course of improvement, return of drooling, and additional treatments required were assessed by both chart review and patient/caregiver telephone interview. Drooling score was assigned based on the standard scale seen in Table 1. This drooling score was introduced by Crysdale and White 4 in 1989 and was modified for use in our multidisciplinary Drooling Management Clinic beginning in 1990 and applied on all patients at each visit. The patient's preoperative drooling score was compared with the patient's immediate postoperative drooling score and all subsequent score changes over time rated at each postoperative visit. All patients in this study had their drooling score compiled by the senior author (SFC) in the course of obtaining patient histories and clinical follow-up. Each child seen within the setting of the multidisciplinary Drooling Management Clinic is tracked with a standardized form to maintain consistency between all specialties.
Standardized scoring system used to assess drooling severity and frequency; score is derived by adding the severity score to the frequency score for a total out of 10
When treatment failure occurred, the timing and source of failure were noted. All patients with recurrence of drooling were referred for technetium 99 salivary flow scanning. 5 The anticipated result to delineate surgical success is a lack of washout of radionucleotides. Thus, a washout of the radionucleotides in nuclear scan implied recanalization of the previously ligated salivary duct and a surgical failure. The findings of available technetium 99 scans were recorded. Further therapies used for each patient within the study were recorded.
A postoperative telephone survey, created for use with this analysis and not separately validated, was also used to provide late follow-up of patient outcomes. Patient caregivers were asked the battery of questions listed below.
How does your child's drooling impact his/her life currently?
Would you say your child never drools, drools occasionally, drools frequently, drools constantly, or drools constantly with a wet pillow?
Would you say your child is dry or never drools now or that his/her lips are wet, chin is wet, clothing is wet, or that the drooling soils materials beyond the child's clothing?
Did your child experience any problems during the procedure?
Did your child experience any problems after the procedure?
How long after the procedure did these problems occur?
If your child's drooling was improved by the procedure, how long did this improvement last?
What additional therapies has you child undergone to control his/her drooling?
Do you feel this procedure was beneficial for your child? Rated on a scale of 1 to 5, 1 = no benefit at all, 5 = complete resolution.
The results of the data gathered by chart review and phone conversation were then evaluated.
RESULTS
Total Surgical Population
Thirty-one patients were treated with intra-oral surgery for the management of sialorrhea between December 1999 and February 2003. Each child within this review had a neurologic condition as the root cause of oropharyngeal dysfunction; 90% (n = 28) in this study had cerebral palsy. The three patients in this study without cerebral palsy had separate individual diagnoses: Down syndrome, schizencephaly, and Sanfilippo's syndrome. All patients were cared for by consistent caregivers, in most cases, a biologic or adoptive parent, but occasionally, the patient received care from a foster parent. No patients were institutionalized.
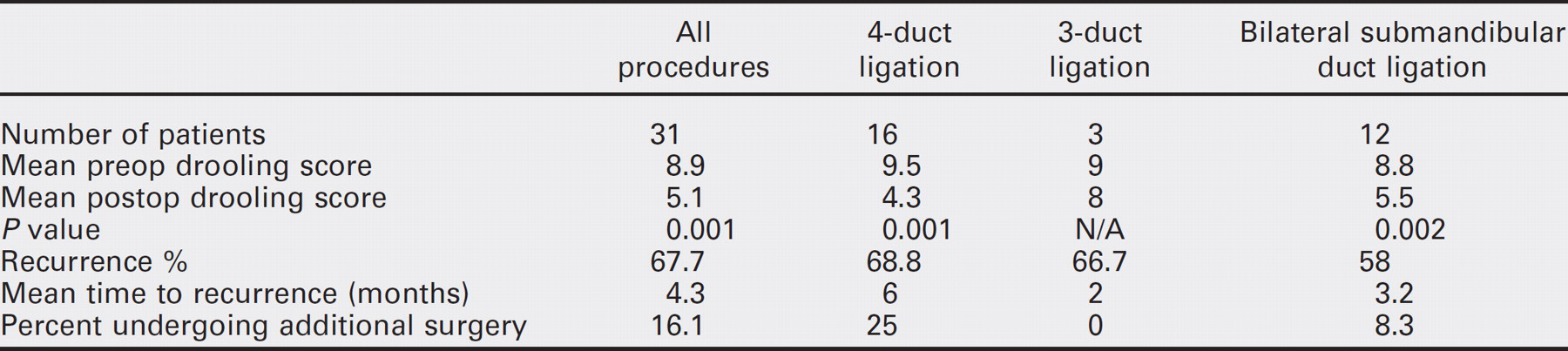
The results are summarized in Table 2. The mean presurgical drooling score was 8.9 (range, 7 to 10) and the mean postoperative score was 5.1 (range, 0 to 10), which represents a change from severe constant drooling to mild to moderate and occasional drooling. This change was evaluated with the Wilcoxon signed rank test and found to be significant to a P value less than 0.001. Recurrence of drooling occurred in 21 (67.7%) patients. The mean time to recurrence was 4.3 months, with a range of two weeks to 19 months. The mean follow-up period was 16 months with a range of two weeks to 60 months. Postoperative and postrecurrence technetium 99 salivary flow studies were recommended in all 21 patients and were undertaken in six patients, each demonstrated uptake and washout in more than one gland.
Painful swelling of the treated glands was the next most common complication, seen in four (12.9%) patients. Additional surgery was required in five patients. Four patients underwent submandibular gland excision (SGE), and one underwent laryngotracheal separation. Two patients received bilateral submandibular gland botulinum toxin therapy.
Phone survey was attempted for 27 patients with four patients not contacted as a result of patient death or inability to locate. All deaths were unrelated to the surgical procedure. A total of 10 patient caregivers consented to phone contact; the remainder did not respond to two inquiries. Two of 10 caregivers reported sustained improvement of sialorrhea at two and three years respectively; both patients had undergone 4-duct ligation (FDL). Eight of 10 patient care-givers would not have undergone the procedure given the result, thus rating the benefit for the patient at a mean score of 2.1 of 5. Each of these caregivers stated that the patient under his or her care had experienced improvement of sialorrhea on medical therapy or additional surgical therapy.
Four-duct Ligation (FDL) Patients
Sixteen of 31 patients underwent FDL. The mean presurgical drooling score was 9.5 and the mean postoperative score was 4.3. This change was evaluated with the Wilcoxon signed rank test and found to be significant to a P value less than 0.001. Recurrence of drooling occurred in 11 (68.8%) patients. The mean time to recurrence was six months, with a range of one month to 24 months. The mean follow-up period was 16 months with a range of two weeks to 48 months. Postoperative and postrecurrence technetium 99 salivary flow studies were recommended in 11 patients and undertaken in two patients; both studies demonstrated uptake and washout in more than one gland. Three patients with recurrence of drooling underwent SGE, and one patient required laryngotracheal separation.
Summary of results for all patients and for each of the surgical procedures
Submandibular Gland Duct Ligation (SDL) Patients
Twelve patients underwent SDL. The mean presurgical drooling score was 8.8 and the mean postoperative score was 5.5. This change was evaluated with the Wilcoxon signed rank test and found to be significant to a P value less than 0.002. Recurrence of drooling occurred in seven (58%) patients. The mean time to recurrence was 3.2 months, with a range of two weeks to seven months. The mean follow-up period was 16 months with a range of two weeks to 60 months. Postoperative and postrecurrence technetium 99 salivary flow studies were recommended in all five patients and undertaken in three patients; all demonstrated uptake and washout in more than one gland. One patient with recurrence of drooling underwent SGE, and one patient underwent bilateral submandibular gland botulinum toxin injection.
Three-duct ligation procedure (TDL) Patients
Three patients underwent TDL due to parental choice. The mean presurgical drooling score was 9 and the mean postoperative score was 8; two of the patients had drooling scores that remained unchanged after the procedure. The third patient showed a change from a drooling score of 10 to 7. This patient was never documented to have a recurrence and follow-up was limited to three weeks. No statistical analysis was done on these patients because of the small sample size and minimal change. Recurrence of drooling occurred in two patients. The time to recurrence was within the first two months for both patients. The mean follow-up period was 16 months with a range of two weeks to 60 months. Postoperative and postrecurrence technetium 99 salivary flow studies were recommended in both patients with recurrence of sialorrhea. One patient underwent the test that found uptake and washout in all glands. One patient with recurrence of drooling underwent bilateral submandibular gland botulinum toxin injection that provided a decrease in drooling score from 9 to 4. This effect persisted until the patient's death from progression of underlying illness.
DISCUSSION
Sialorrhea in the pediatric population is common and normal in infants up to 15 to 18 months. Disordered saliva management is seen past four years of age and is frequent with neurologic disability found in 10% of children with cerebral palsy. 1 Additional causative factors include nasal obstruction, malocclusion, poor gag reflex, disordered head posture, impaired peri-oral sensation, and lack of concentration. 6,7 The effects of sialorrhea include cheilitis, dehydration, social and psychological isolation, decreased self-confidence, and aspiration pneumonia. 6
Surgical therapy for sialorrhea is most commonly performed in the setting of profuse constant drooling (9 or 10 of 10), when patients or caregivers are unable to comply with other therapy, or with a lack of improvement with therapy or other oral training. 8 Crysdale et al 8 estimated 59% of neurologically impaired patients require surgery.
Surgical therapy for sialorrhea has been performed in a variety of ways with widely varying degrees of success. Submandibular gland excision (SGE) has been widely studied and is purported to eliminate resting salivary flow. 9 Many surgeons consider the risk of complications too great for widespread use. Complications for bilateral SGE include wound infection, xerostomia, lingual and hypoglossal nerve injury, facial paresis (36%), or paralysis (7%). 10 An additional consideration with bilateral SGE is the external incision. To avoid the external incision, Miloro 11 reported intraoral excision. To further improve the results of SGE, parotid duct relocation to the tonsillar fossae in combination with SGE was first reported by Wilkie in 1977 with a success rate of 86%. 12
In 2001, Crysdale et al 8 reported extensive experience with submandibular duct relocation alone and in combination with sublingual gland excision. This article highlighted similar outcomes with and without sublingual gland excision but fewer complications including pseudocyst formation and need for additional surgery. The extended follow-up of this study highlighted the long-term efficacy of these procedures. Relocation procedures have been questioned with respect to several factors including whether the relocation actually created a stenosis equivalent to ligation. 5
Given the variability in the reported success of rerouting procedures and the improved success rates when multiple glands are addressed, less invasive procedures have been investigated. Klem and Mair 3 reported outcomes of bilateral parotid and submandibular duct ligation in 1999 with a success rate of 80% over the 13 months of follow-up. Shirley et al 2 reported similar success rates over a similar follow-up time frame with the use of the ligation technique described by Klem and Mair. 3 Both reports were retrospective in nature and paralleled our analysis.
Our results diverge from these two series with a success rate of 31%; relatively poor results across a population of patients and caregivers seeking long-term control of sialorrhea. Analysis of only those patients who undergo ligation of all four ducts (FDL) yields strikingly divergent results than those seen in both series mentioned previously. The failure rates seem logical in the patients in which less than four salivary ducts were ligated. However, each of these patients cannot be viewed out of the context of his or her overall medical condition and caregiver choices. Follow-up with technetium 99 scanning provides a clue as to why the failures occurred. The possibility of faulty surgeon technique, namely too tight a ligature, needs to be considered. It should be noted that when the failures began to accrue, the surgical technique was modified to include a distal 4-0 suture combined with proximal 3-0 suture to avoid the possibility that the duct wall tissues were simply cut through resulting in failed ligation and recanalization. This modification resulted in no appreciable change in outcome.
The failure of FDL to provide long-term control of sialorrhea and the return of salivary flow seen on technetium 99 scanning suggests a point for further research. We believe that failure of ligation in our population is a result of recanalization of the ligated ducts. Later cases in this series used double ligation of the salivary ducts with continued frequent recurrence of sialorrhea. Although intra-oral procedures avoid the morbidity of external surgery, ligation of the gland in the setting of continue salivary flow places the ligation zone at risk for fistulization. The ligation of the salivary gland duct theoretically provides negative feedback to the gland with anticipated resultant reduction in saliva flow and eventual gland shutdown. This was not our experience on numerous occasions. We question whether long-term reduction or complete inhibition of salivary production from each of the glands before ligation might assist in healing of the ligation area and inhibition of future salivary production. This topic could be assessed by medical therapies already available, including botulinum toxin. If undertaken, it is important to use the medical therapy for an extended course as one of our patients who had a painful salivary gland swelling after duct ligation had his medical therapy discontinued by his parent on the first postoperative day.
There are several limitations inherent in this study population. The use of three different procedures makes analysis of each technique necessary to make conclusions. Failure to achieve maximal salivary flow control is inherent in surgical procedures that do not address all four major salivary glands. The chronic health condition associated with this patient population necessitates frequent outpatient and inpatient care. We believe this factor contributes to the higher level of patients who returned sporadically. This makes conclusions about length of follow-up somewhat complex. An additional confounding factor was the concurrent anticholinergic medication use seen in this population. Many patients resumed use of these medications or opted for continued use after failure to gain adequate control through the intra-oral surgery.
Several sources of bias are also evident in this review. The retrospective nature alone introduces issues related to data collection. Although every effort was made to maintain consistency in recording drooling score, the rating is based on both physical examination and caregiver assessment. We had a high level of caregiver consistency and the senior author provided all scoring based upon caregiver answers, which fortunately minimizes same-patient variability. However, the wide range of follow-up lengths makes consistent time-point evaluation a significant challenge. Given the medical challenges the patients' underlying conditions place on caregivers, standardized follow-up time-points would be an unacceptable burden, especially considering the high frequency of health-related visits, both planned and unplanned. Although this makes analysis more complicated, it is a factor that all multidisciplinary teams consistently face.
CONCLUSION
Intra-oral surgical management for sialorrhea provides minimal long-term control of sialorrhea. Additional medical and surgical therapy including anticholinergic medication, botulin toxin injection, and excision of bilateral submandib-ular glands was needed in a significant portion of patients with sialorrhea in this long-term review.
FINANCIAL DISCLOSURE