
Abstract
GER into the nasopharynx has been implicated as an inflammatory cofactor and possible cause of OME. 9-13 GER is a common physiological occurrence in neonates and infants that decreases in frequency during the first year of life. Studies in animal models suggest that GER may be related to Eustachian tube dysfunction. 11-13 Current techniques used to detect reflux include esophageal pH and impedance probes, esophagoscopy with biopsy, chest radiography, and barium meal. However, these are not used routinely in patients with middle ear disease because they typically do not present clinical signs or symptoms of GER. 8
Because comprehensive testing for GER is not done in this population, studies addressing the relationship between GER and OME have been limited. Recently, the ability to detect gastric pepsin in middle ear fluid has led to a new direction in elucidating the role of GER in middle ear disease. Two recent studies by Tasker et al 14,15 have reported detectable pepsin in 83 to 90 percent of middle ear fluid samples using an ELISA (concentration range, 0.8 to 213 mg/ml) and 24 to 29 percent using an enzymatic method. Lieu et al 16 reported that pepsin was present in 77 percent of middle ear fluid samples in patients with OME (n = 36) using an ELISA (concentration range, 2.68 to 196 mg/ml) and in 73 percent using an enzymatic assay (concentration range, 1.33 mg/ml to 275 mg/m). The goals of this study were to confirm these findings in a larger sample size and to develop a more sensitive and specific method to detect trace amounts of pepsin in middle ear samples.
MATERIALS AND METHODS
Study Subjects
One hundred fifty-two patients scheduled for myringotomy with tube placement for otitis media were enrolled in a prospective study to evaluate the presence of pepsin in middle ear aspirates. The patients ranged in age from 6 months to 10 years (43 boys, 57 girls). Demographic and clinical data, including patient age, sex, admitting diagnosis, operative procedure, and other medical history such as gas-troesophageal reflux disease (GERD), allergy, and asthma, were collected by chart review. The study was approved by the IRB of the sponsoring institution, and informed consent and assents were obtained.
Criteria for Diagnosis of Otitis Media
Patients were scheduled for bilateral myringotomy with tubes based upon clinical history and otoscopic evaluation in a tertiary care pediatric otolaryngology clinic using standard accepted criteria of the American Academy of Family Physicians, American Academy of Otolaryngology-Head and Neck Surgery, and American Academy of Pediatrics Subcommittee on Otitis Media with Effusion. 17
Middle Ear Fluid Sampling
Myringotomy with tubes was performed using general inhalation anesthesia in the operating room. At the time of myringotomy (prior to placement of the tube), a suction cannula was placed through the myringotomy incision into the middle ear cleft. If fluid was present, this was aspirated in its entirety into a Lukens trap; then, while the cannula was maintained in the middle ear space, 1 ml of sterile saline was flushed into the external auditory canal and allowed to flow into the middle ear cleft and then aspirated with the suction cannula. This was to allow tenacious secretions to be flushed from the suction cannula into the specimen container for analysis. If no effusion was present in the middle ear space and to recover any pepsin adherent to the middle ear mucosa, the cannula was placed through the myringotomy incision and 1 ml of sterile saline was flushed into the external canal and allowed to bathe the middle ear cleft prior to aspiration. The fluid aspirated into the Lukens trap was immediately transferred to a freezer and stored at −20°C in preparation for pepsin assay. Ears were categorized by the operating surgeons at the time of surgery as being “dry” or “with effusion” based on the otomicroscopic appearance of the middle ear cleft after myringotomy and recorded in the operative note.
Pepsin Assay
The enzymatic assay initially described by Krishnan et al 18 was modified to increase the lower limit of sensitivity from 250 ng/ml to 12.5 ng/ml. The key changes included use of 0.1 mg/ml bovine serum albumin (BSA) in the reaction buffer and lowering of the pH to 2.0 in the reaction. Briefly, pepsin (porcine) standards (12.5 to 400 ng/ml) were prepared in 0.1 mg/ml BSA with saline (pH 5.5). Gastric fluids used as positive controls from two unidentified patients were diluted in the same BSA/saline solution. Samples, standards, and controls (50 ml) were mixed with 23 ml of 129 mM hydrochloric acid to adjust the pH to 2.0 and left on ice for 15 minutes to inactivate lysosomal acid hydrolase (cathepsin D) and to convert pepsinogen to active pepsin. Next, the samples were incubated with 20 ml of 0.5 percent fluorescein isothiocyanate casein (FITC-casein) as a substrate for 3 hours at 37°C. Alternatively, the reaction was carried out with various concentrations of BSA to determine the interference of protein on the assay. The enzymatic reaction was stopped by inactivation at 100°C and followed by trichloroacetic acid (TCA) precipitation and centrifugation. Supernatant (38 ml) was transferred to a microplate and mixed with 212 ml of 500 mM Tris (pH 8.5). The plate was read in a spectrofluorometer (Cytofluor Plate Reader 4000; Perseptive Biosystem, Stafford, TX) with excitation at 485 nm and emission at 530 nm. The net fluorescent unit of an assay was calculated by subtracting values from a blank in which pepsin was inactivated by incubating at 100°C for 10 minutes prior to the addition of the substrate. Duplicate reactions were performed for both blank and assay. Any experiment in the assay or blank with a deviation greater than 10 percent over the average of the duplicates was repeated. The final pepsin concentration of a sample was determined based on the net fluorescent unit of the known concentrations of the standards.
Determination of the Lower Limit Sensitivity of Pepsin Assay
Enzymatic reaction of porcine pepsin concentration at 0.0, 12.5, 25, 50, 100, 200, and 400 ng/ml was performed 10 times at conditions described above to determine the consistency and the lower limit sensitivity of the assay. The standard curve from the average value of the 10 runs had an R 2 = 0.99. Pepsin (porcine) at 12.5 ng/ml had a net fluorescent unit increase of 35.0 ± 11.0 percent (mean ± SD) over the blank, which was significantly higher than that of the negative control (0.0 ng/ml pepsin consisting only of buffer and reagents) with 8.7 ± 4.2 percent net fluorescent unit increase (P < 0.05). Pepsin at 6.25 ng/ml or less had a similar net fluorescent unit increase over the blank as the negative control (0.0 ng/ml pepsin). Therefore, the empirical pepsin level differentiating positive from negative for pepsin in a sample was set at the lower limit of the sensitivity of the assay at 12.5 ng/ml. A patient was defined as pepsin-positive if one of the ear samples had pepsin above 12.5 ng/ml. FITC-casein (type III) and porcine pepsin A were purchased from Sigma-Aldrich (St. Louis, MO).
Data Analysis
Pepsin positivity in patients or samples was expressed as percent of pepsin-positive samples over the total number of samples in a group. Pepsin concentration was expressed as mean with SD. Data were analyzed using the Student t test and the Fisher exact test to look for significant differences. P value <0.05 was considered a significant difference.
RESULTS
Description of the Study Subjects and Samples
A total of 152 patients diagnosed with otitis media and undergoing unilateral or bilateral myringotomy with tube placement were enrolled in the study from 2005 to 2006. Characteristics of the study subjects and the samples collected are summarized in Table 1. The average age of the 152 children was 2.8 ± 2.3 years, ranging from 6 months to 10 years. Clinical history of GERD, allergy, and asthma is depicted in Table 1. Only a few patients had objective confirmation in their medical record of GERD, allergy, or asthma based on pH/impedance probe testing, endoscopy with biopsy, skin testing, or pulmonary function testing (five for GERD, three for allergy, and six for asthma). A total of 225 middle ear samples (114 from dry ears and 111 from effusion ears) from the 152 patients were collected. Seventy-three patients had two samples collected, and 79 had one sample collected.
Description of the study subjects
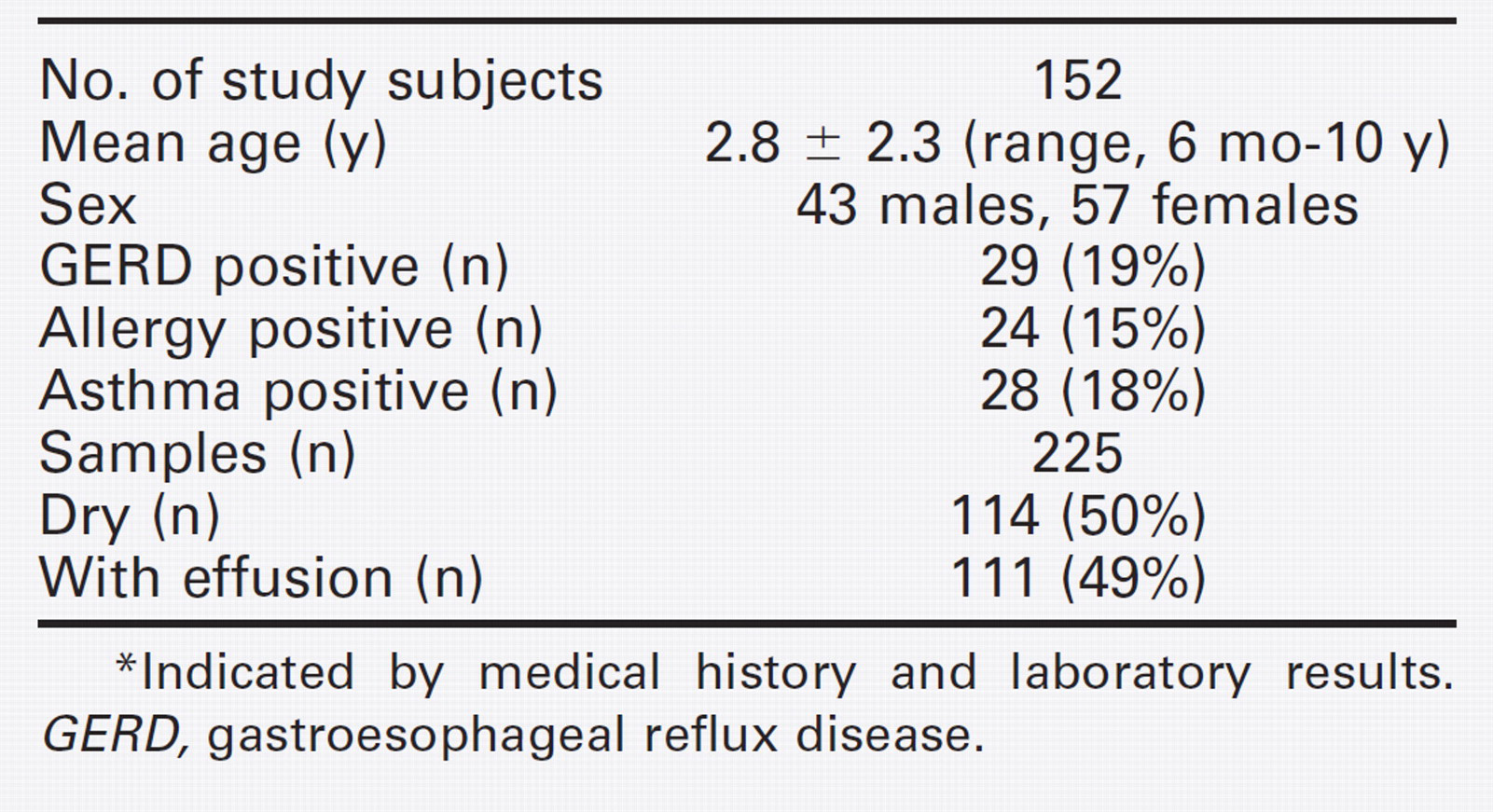
Indicated by medical history and laboratory results. GERD, gastroesophageal reflux disease.
Pepsin Positivity
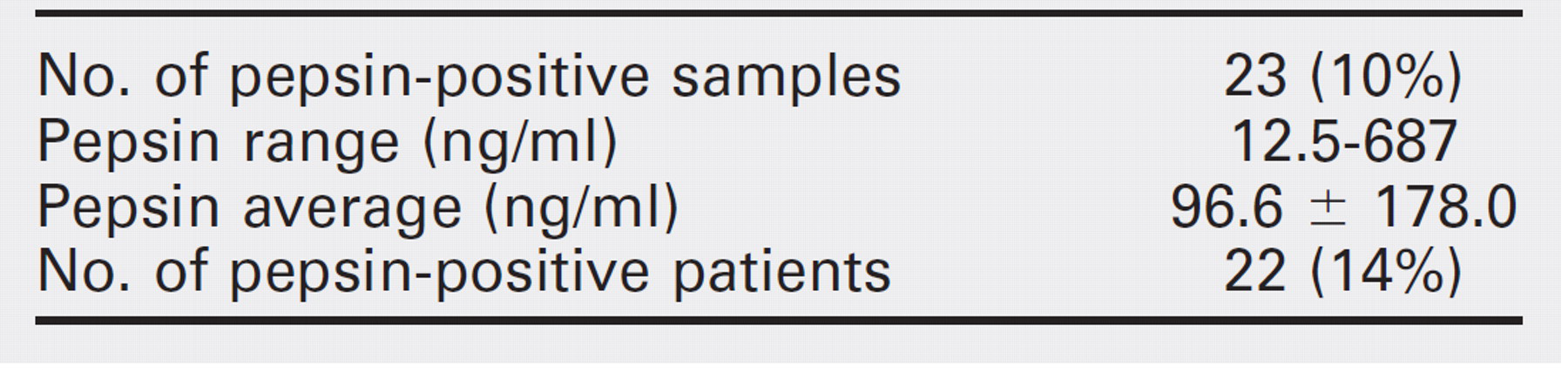
Using the modified enzymatic method, we measured pepsin activity in all 225 samples. Ten percent (23 of 225) of the samples had pepsin activity above the detectable level with an average of 96.6 ± 170.8 ng/ml, ranging from 12.5 to 687 ng/ml (Table 2). The 23 pepsin-positive samples were from 22 patients, with only one patient having both ear samples positive for pepsin. The overall incidence of pepsin detected in the middle ear fluid of this cohort was 14.4 percent (22 of 152).
Pepsin Positivity in Dry Versus Effusion Ears
Pepsin positivity was compared between samples from dry ears (n = 114) and those with effusion (n = 111). Figure 1 shows that 13.5 percent of samples with effusion had detectable pepsin activity, and 7 percent of samples from dry ears were positive. This difference did not reach statistical significance (P > 0.05). Similarly, pepsin levels were higher in samples with effusion (n = 16; 151.6 ± 180.7 ng/ml) when compared with dry ear samples (n = 7; 52.6 ± 79.8 ng/ml) but were not statistically different (P > 0.05).
Pepsin data summary
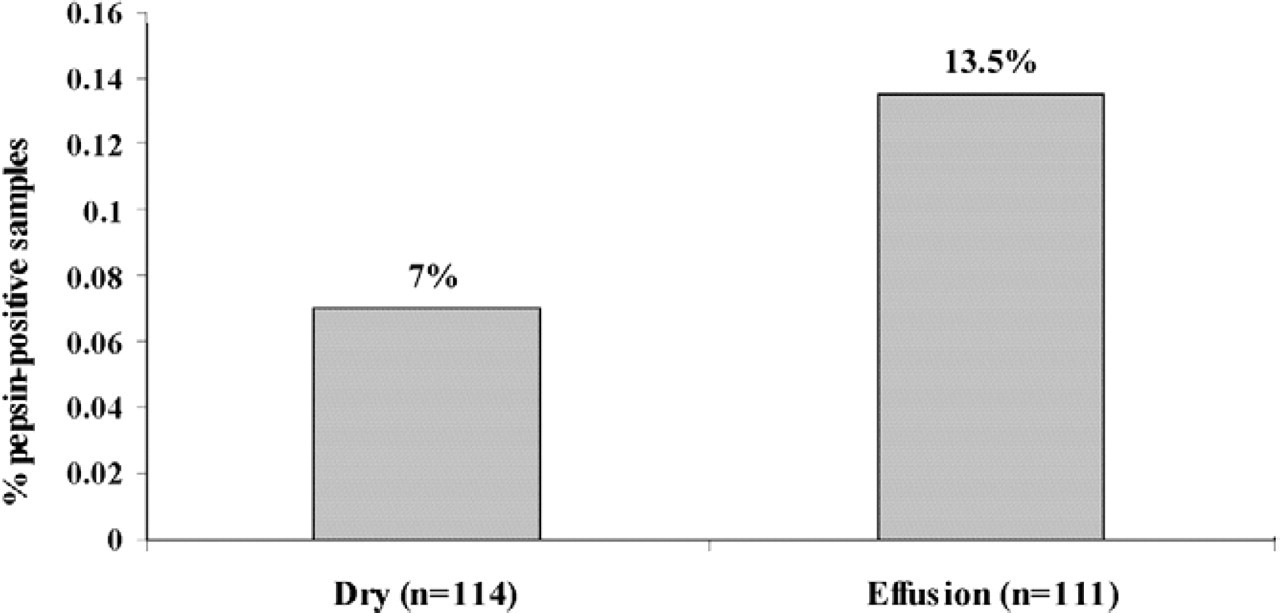
Comparison of pepsin positivity of dry and effusion ear samples. Pepsin positivity was expressed as percent of pepsin positive samples divided by the total number of samples in a group.
Analyzing Pepsin Positivity with Age and Clinical Parameters
Pepsin results were stratified and compared among four age groups (Table 3). Children younger than 1 year had a higher rate of pepsin positivity (27 percent) when compared with the other three age groups, but the difference was not statistically significant (P > 0.05). Comparison of pepsin concentration in the samples revealed the group younger than 1.0 year had significantly higher levels (P < 0.05) than two of the older age groups (2 to 4 years and >4 years) but not the group 1.0 to 2.0 years old. Even though pepsin levels were higher in the 1- to 2-years group than that in the other two older groups, the difference was not statistically significant (Table 3). We found no correlation between pepsin positivity and presence or absence of clinical history of reflux, allergy, or asthma (Table 4).
Pepsin Assay Development
To test the specificity of the assay that we developed, pepsin activity in human gastric fluid was measured as positive controls and in serum as negative controls. Gastric fluid was diluted 800-fold with saline/BSA before it was assayed. The final concentration of pepsin was 132 μg/ml and 71 μg/ml, respectively, from the two unidentified individuals. In addition, pepstatin, a pepsin inhibitor, was included in the reaction to test the specificity of the assay. Pepstatin completely inhibited pepsin activity in gastric fluid and ear samples. No pepsin activity was detected in serum, undiluted or diluted, and measured in various concentrations with saline/BSA. Protein concentration was determined in all samples with an average of 3.0 mg/ml, ranging from less than 0.1 mg/ml to 39.5 mg/ml. We noticed that the fluorescent units of the blanks were much lower in samples with high protein concentration (>10 mg/ml) when compared with samples with average protein concentration. We suspected that protein at very high concentration might interfere with the assay. To test this, we measured porcine pepsin activity (50 ng/ml) with BSA at various concentrations. Figure 1 shows that BSA at 48 mg/ml completely inhibited pepsin activity. The inhibition was still significant at BSA concentrations of 10 mg/ml, but pepsin activity was detectable, and no further inhibition was observed at BSA concentrations of 2.5 mg/ml or less (Fig. 2). Similar results were observed when the same experiment was carried out with control serum at the same concentration of BSA (data not shown). These data suggest that samples with high protein contents should be diluted to at least 10 mg/ml to detect pepsin activity. However, over dilution might also dilute pepsin levels in the sample below the detection limit. Therefore, to accurately determine the pepsin concentration of a sample with protein content greater than 2.5 mg/ml without over dilution of the pepsin, the pepsin activity of the standards was determined at a similar protein (BSA) content as the sample. Specifically, the pepsin concentration of any sample with a protein concentration greater than 2.5 mg/ml was determined using a calibrated standard curve obtained at a similar protein concentration to the sample.
Pepsin data by age groups
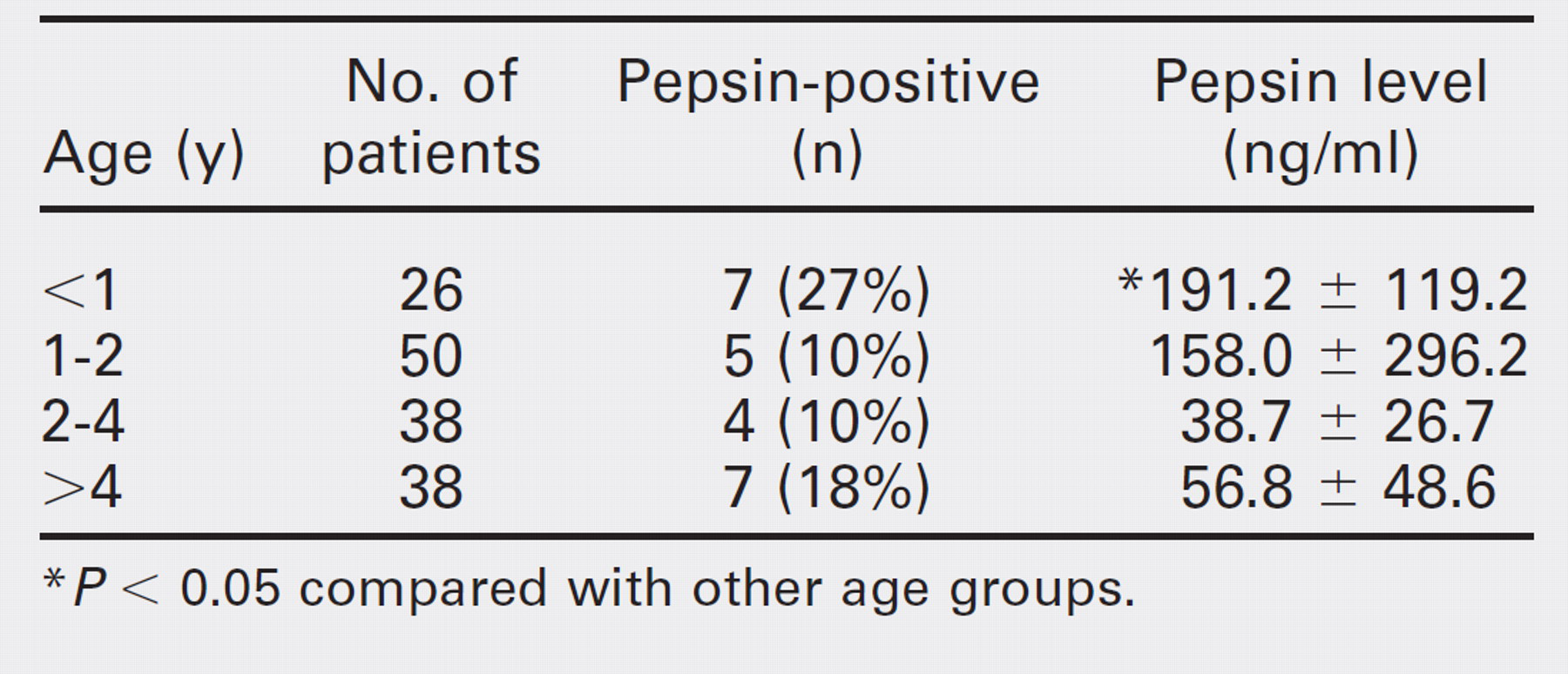
P < 0.05 compared with other age groups.
Comparison of pepsin positivity and clinical parameters
GER, gastroesophageal reflux.
DISCUSSION
In this study we report on a modification of the pepsin enzymatic method initially described by Krishnan et al 18 to improve the sensitivity from 250 ng/ml to 12.5 ng/ml. These experiments and statistical analyses establish a cutoff value to distinguish pepsin positivity from negativity in middle ear samples. Using our methods, positive controls (active pepsin in gastric fluid) showed a pepsin concentration ranging from 72 to 130 μg/ml, whereas no pepsin activity was detected in serum. Of the 225 samples from the middle ears of 152 patients undergoing myringotomy with tube for otitis media, pepsin was detected in 10 percent with 14.4 percent of patients having at least one ear sample positive. Our data demonstrate a trend toward a higher rate of pepsin recovery in ears with effusions and in children younger than 1 year, but the number of subjects was inadequate to demonstrate statistical significance.
Two studies so far have demonstrated the presence of pepsin (or pepsinogen) in middle ear effusions. Lieu et al 16 reported that 77 percent of samples had detectable pepsin with an ELISA and 73 percent of samples had detectable pepsin using an enzymatic method. We used a modified version of the enzymatic method that was initially described by Krishnan et al 18 and found only 14.4 percent patients had detectable pepsin in one or both ears in concentrations much lower than that reported by Lieu et al. 16 Our modifications could only increase the prevalence of pepsin positivity because our method showed greater sensitivity than the initial assay. The limitation of the enzymatic method is that it can only detect active pepsin or pepsinogen. Inactive pepsin is measured only by immunoassay, such as ELISA or Western blot analysis. We believe that using a cutoff of 12.5 ng/ml to call a sample positive in our method gives us a sensitivity equal to or better than that achieved with the immunoassay technique for pepsin detection.
A possible reason for the discrepancy in our results compared to prior studies could be the difference in the type of ear samples. More than half of our ear samples were collected from dry ears without effusion present compared with prior studies done only on patients with effusions. 16 It is not known if the presence of pepsin in the middle ear is related to the underlying pathophysiologic process causing the effusion and may speak to the severity of disease or to the sampling technique and the potential inability to collect an adequate sample from a dry ear. When we compared samples with and without effusion, we found that pepsin positivity and pepsin levels were higher in the samples with effusion, but the difference was not statistically significant. Therefore, it is possible that the discrepancy between our results and those of other studies was contributed in part by the difference in sample type as demonstrated in our results (Fig. 1); however, it is also possible that the improvements we made in the assay technique resulted in more accurate results.
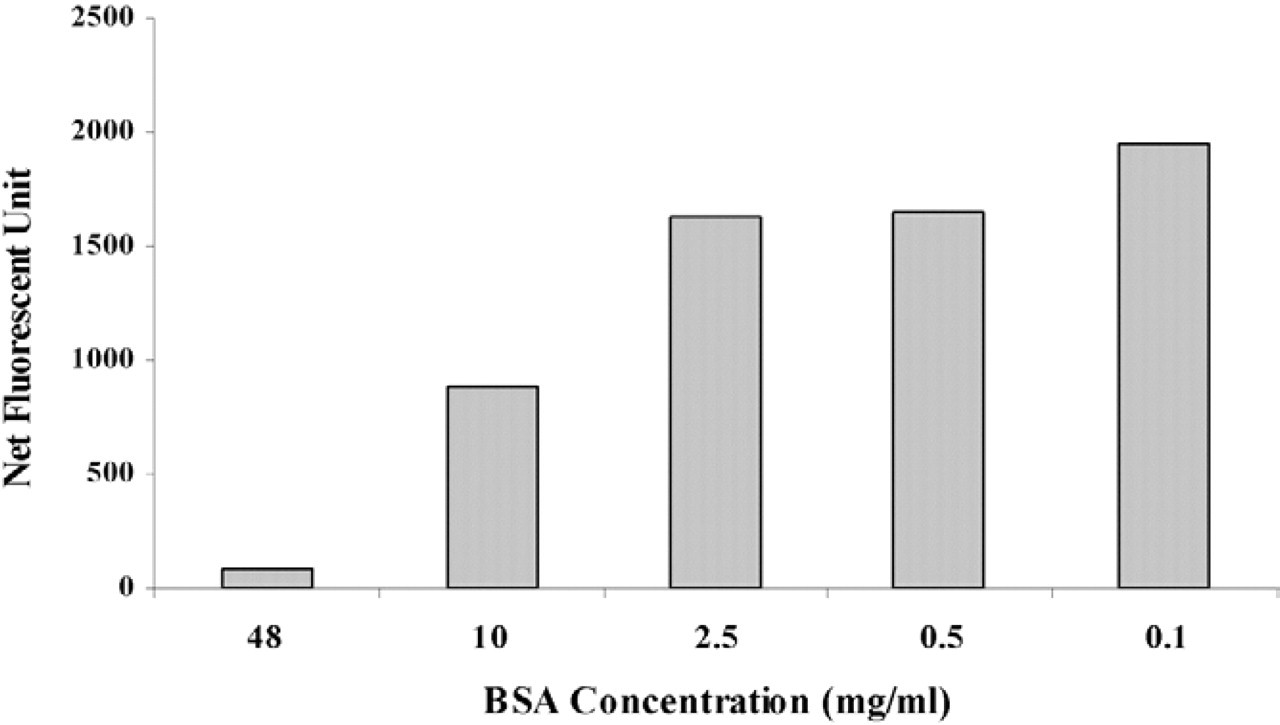
Net fluorescent unit of porcine pepsin (50 ng/ml) measured in saline containing various BSA concentrations. BSA at 0.1 mg/ml was a standard condition for samples that had a protein content of less than 0.1 mg/ml.
An earlier study by Tasker et al 14,15 revealed that 83 to 90 percent of effusion samples were pepsin positive using an ELISA and 24 to 29 percent were positive using the enzymatic method. The results from the enzymatic assay were similar to our observations. The slight variation could be due to the difference in the enzymatic methods used or the difference in effusion types as described above. The larger difference in the results using the ELISA may have been due to cross-reactivity of the antibody. In our unpublished Western blot data with the same commercially available polyclonal antibody used by Tasker et al, 15 we found that the antibody recognized a nonspecific protein in addition to pepsin at a higher molecular weight, and a protein at the same molecular weight was also observed in normal serum. This unknown protein was observed in most of the samples we tested because middle ear fluid samples often are contaminated with blood. This contamination suggests that the unidentified serum protein recognized by the poly-clonal antibody could contribute partly to the reported positive pepsin detection in some ear samples when tested by ELISA, thus resulting in falsely high rates of pepsin. Therefore, caution is necessary when using Elisa. If an antibody has a strong nonspecific interaction with other proteins in the samples, it will exhibit a high false-positive rate. Currently, no pepsin antibody has been tested enough to ensure high sensitivity and specificity.
The concentration of pepsin in prior studies was measured in micrograms, 14-16 whereas our pepsin level was measured in nanograms, which represents a significant difference. It is difficult to compare the level of pepsin in the different studies because different methods of sampling and pepsin assay were used. The only meaningful analysis is to compare with a positive control, such as gastric fluid, and a negative control, such as serum. Between the expected physiological clearing of small amounts of gastric fluid from the middle ear and dilution by saline lavage during sampling, it is expected that the range of pepsin concentration in the middle ear would be significantly lower than that in gastric fluid but higher than that in serum. Our results confirmed this expectation in that there was only a trace amount of pepsin in the middle ear fluid when compared with gastric fluid.
GER is frequently encountered in infancy with or without the typical symptoms of GERD. 19-22 Symptomatic GER only occurs after prolonged exposure to gastric contents and can lead to GERD with clinical complications. 23 In our study population, less than 20 percent of patients had clinical evidence of GERD, with only six patients having documented evidence of GERD on pH-probe. However, in this subgroup, there was no statistical association with detection of pepsin in the middle ear (Table 4). It has been postulated that the exposure of gastric contents to extraesophageal organs such as the airway may not always lead to typical symptoms of GERD in infants. 24 Even in our patients younger than 1 year who had a trend toward a higher rate of pepsin positivity and pepsin concentration when compared with other age groups (Table 3), detection of pepsin was not associated with signs or symptoms of GERD (data not shown). Our results suggest that the detection of pepsin in the middle ear of these children might not be always related with classic GERD symptoms.
Accumulated evidence has established that GERD is likely to induce or exacerbate asthma. 25 In our study, only 15 percent (24 of 152) of patients had clinical or objective evidence of allergy and 18 percent (28 of 152) had clinical or objective evidence of asthma. Presence of pepsin in the middle ear was not correlated with either allergy or asthma (Table 4). However, a larger sample size may be required to reveal the association.
The frequency of pepsin recovery from the middle ear of patients diagnosed with otitis media undergoing myringotomy with tube placement requires further investigation. In prior studies, the sample sizes were small: 36, 54, and 65 ears, respectively. 14-16 We had a larger sample size (n = 225), however, the number of pepsin-positive samples was still relatively small (n = 23) and likely impacted our ability to correlate our findings with clinical symptoms. The pathophysiological role of gastric reflux in otitis media requires further investigation in a larger sample size. This will require the verification of absence of pepsin in ears of a control population without otitis media to further support the role of gastric reflux in otitis media. We are currently evaluating this in a larger study in our institution.
In conclusion, we report a 14.4 percent prevalence of pepsin in the middle ear of patients with otitis media, suggesting that gastric reflux might be a factor in middle ear disease. Further study with a larger sample size and a negative control group without otitis media is needed to confirm these results. Our results also demonstrate that this assay has the potential to become a reliable, sensitive, and simple way to detect pepsin in middle ear fluid and in samples from other sources for research or clinical testing.
FINANCIAL DISCLOSURE
None.