
Abstract
Objective
Stroke is the third leading cause of death in the United States, behind heart disease and cancer. It affects as many as 5% of the population over 65 years old, and this number is growing annually due to the aging population. A significant portion of stroke patients that initially survive are faced with the risk of aspiration, as well as quality-of-life issues relating to impaired communication. The goal of this paper is to define the scope of practice in otolaryngology for these patients, and to review pertinent background literature.
Study Design
Consensus report and retrospective literature review.
Results
Otolaryngology involvement in these patients is critical to their rehabilitation, which often requires an interdisciplinary team of specialists. This committee presentation explores epidemiological data regarding the impact of stroke and its complications on hospitalizations. A pertinent review of neuroanatomy as it relates to laryngeal function is also discussed. State-of-the-art diagnostic and therapeutic procedures are presented.
Conclusion
There is a well-defined set of diagnostic and therapeutic options for laryngeal dysfunction in the stroke patient.
Significance
Otolaryngologists play a critical role in the interdisciplinary rehabilitation team.
© 2007 American Academy of Otolaryngology-Head and Neck Surgery Foundation. All rights reserved.
The session is divided into six sections: 1) epidemiology of stroke, 2) neuroanatomy, 3) voice production, 4) differentiation with other voice disorders, 5) common themes in the stroke population, 6) state-of-the-art diagnostic evaluation, and 7) interdisciplinary management with special attention to swallowing and airway protection.
The role of the otolaryngologist in managing these patients is emphasized, along with practice-oriented tips. Interventions for airway and swallowing safety, management of the dysfunctional upper esophageal sphincter, surgical management of glottic insufficiency, and strategies for secretion management are discussed. Discussion reinforces that early multi-specialty involvement and good communication are integral to the care of these complex patients.
Epidemiology of Stroke
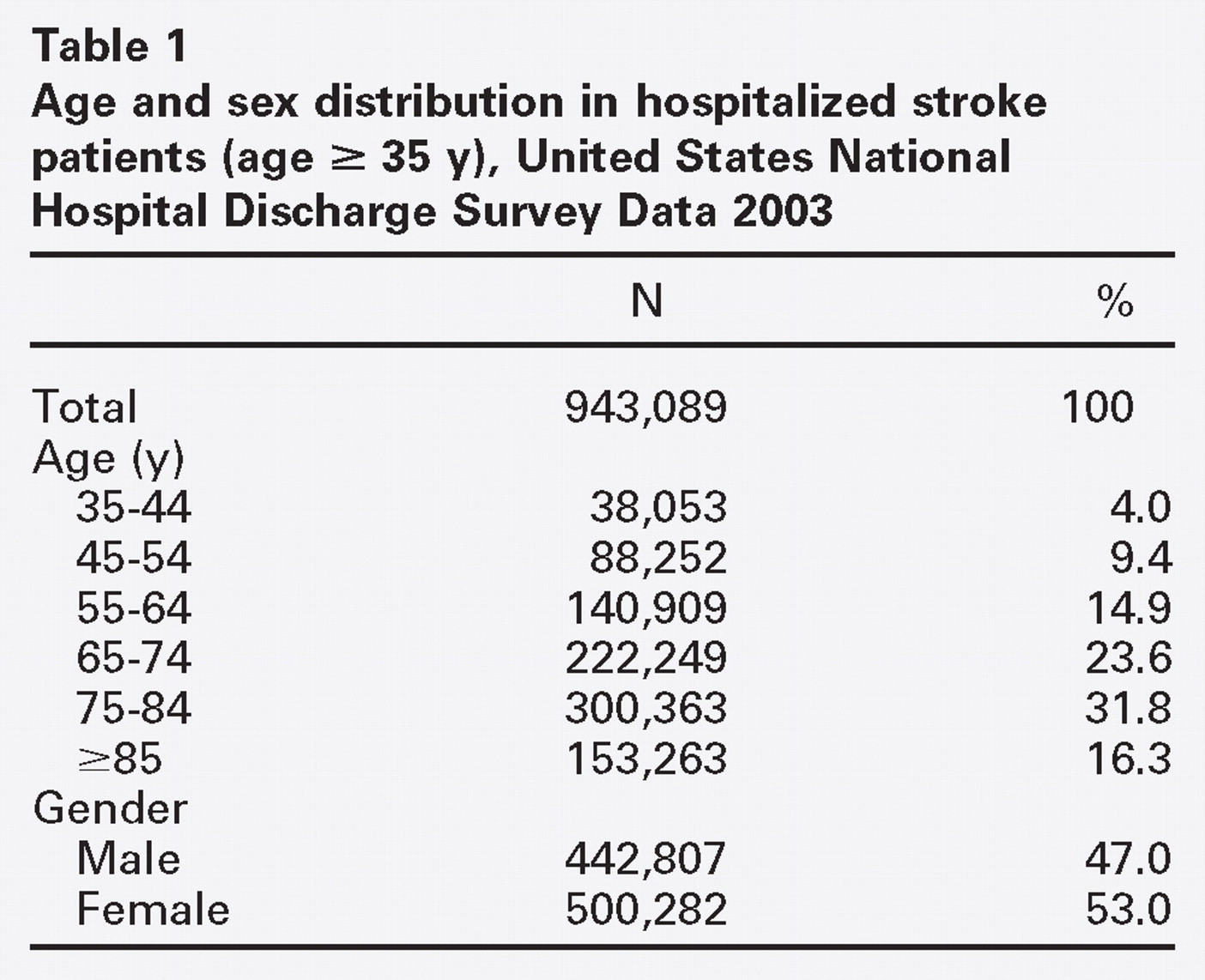
Stroke is the third leading cause of death in developing countries, behind heart disease and cancer. The median age is about 70 years in men and 75 years in women. A number of studies recognize the high prevalence of 5 to 7/1000, with greater than 5% of the population over 65 years old affected. The morbidity and mortality of cerebrovascular accidents is also significant, with a one-month fatality rate of about 23%. 1 Ischemic strokes account for 75%, while intracerebral hemorrhage accounts for 15% and subarachnoid hemorrhage 5% of all strokes. 1
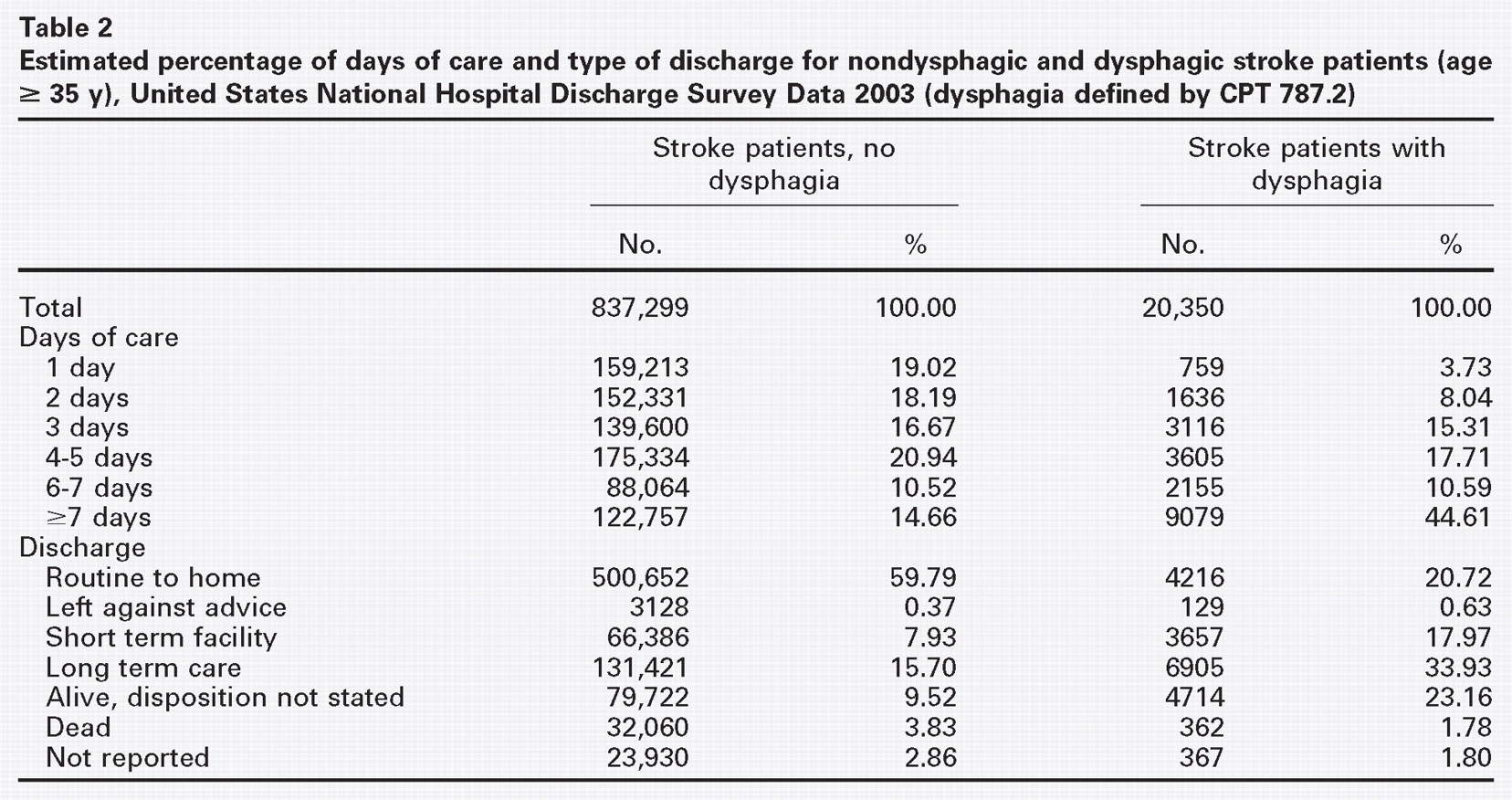
Stroke is also a major cause of serious, long-term disability among adults; the projected cost of stroke during 2003 is $51 billion, including $12 billion in nursing home costs. During 1988-1997, the rate of hospital admission for stroke increased 18.6%, from approximately 560 per 100,000 population in 1988 to 664 in 1997. 2 , 3 Dysphagia is a common and important complication after acute stroke. The reported rates ranged from 27% to 50% of patients, 4 – 8 depending on the timing of the assessment, the diagnostic methods used, and the case mix. About half of dysphagic patients either die or recover spontaneously within the first 14 days of stroke onset, leaving half with swallowing deficits that can significantly impair function, recovery, and quality of life.
Neuroanatomy
Phonation, speech, and language are interrelated tasks that require respectively higher orders of brain function. Phonation is defined as the production of sounds (phonemes). Speech requires the pronunciation of words from a collection of sounds. Language involves meaningful groupings of words into phrases to communicate ideas. While the neuroanatomy of basic phonation principally involves brain stem functions, 11 , 12 language requires control by the cortex. Production of language involves sensory input from auditory and visual cues, and then input from memory of sounds, spelling, and knowledge prior to generating motor output.
The nineteenth-century neurological model of language was based on the gross anatomy of cortex areas that were damaged by tumors or stroke. Broca in 1861 performed a postmortem examination on a patient with an articulation disorder, and found the defect to be in the left third frontal convolution (“expressive aphasia”). Wernicke in 1874 recognized a patient with impaired comprehension to have a lesion in the left posterior superior temporal cortex (“receptive aphasia”). Further anatomic study defined the arcuate fasciculus as a major conduction pathway between these two areas. 13 The twentieth-century model of language recognizes the complexity of linguistic functions analogous to parallel distributed processing of highly interactive parts (“connectionist”). Functional MRI has further advanced the understanding and relationships between phonation, speech, and language. 13
The production of speech relies on the left-sided dominance of the cortex. However, it has been recently recognized that the right side of the cortex plays important roles in prosody of speech (inflection, intonation, and timing), and creative thought. 14 Corticobulbar tracts are responsible for communication from the cortex to the brain stem. The cerebellum has also been implicated as having a modulatory role in the motor control needed to produce speech. 15 The basal ganglia regulates motor control from these inputs as a higher level of control over the Xth cranial nerve nuclei in the medulla.
Voice Production and Stroke
Components of voice production and their roles
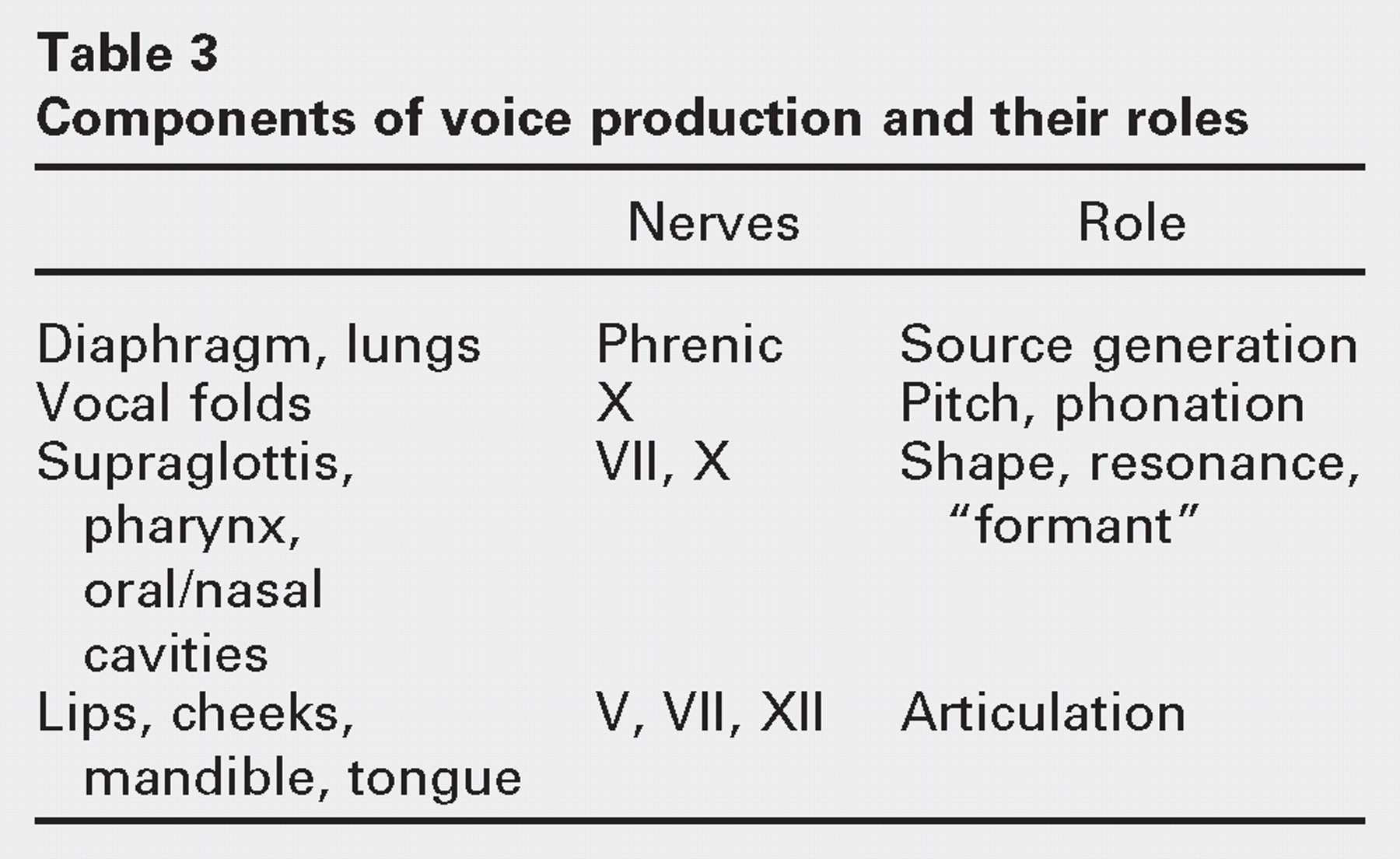
Voice and connected speech changes in CVA are complex and highly dependent on the location of the cerebral event. Vocal fold immobility or paresis is a relatively uncommon finding compared to dysarthria, which is present in 8% to 30%. 16 Spastic voice changes are common with upper motor neuron lesion, as seen in bilateral CVAs. Speech is characterized by slowed articulation, strained voiced quality, and hypernasality. In contrast, flaccid voice changes result from a lower motor neuron lesion in the brain stem, principally from loss of muscle tone and reflexes. In this case, speech quality would be characterized by a breathy voice quality with diminished loudness and air wastage. 17
Vocal fold paralysis as a direct result of stroke is rare, and is most commonly associated with brain stem stroke, lateral medullary syndrome, Wallenberg syndrome, and Claude Bernard Horner syndrome. 18 Motor recovery of the paralysis from these etiologies is likely comparable to motor recovery in general in stroke patients, such that earlier recovery portends a better prognosis. 19 Acoustic voice measures may also reveal high jitter in these patients. 20
Voice Problems Indicative of Underlying Neurologic Disease
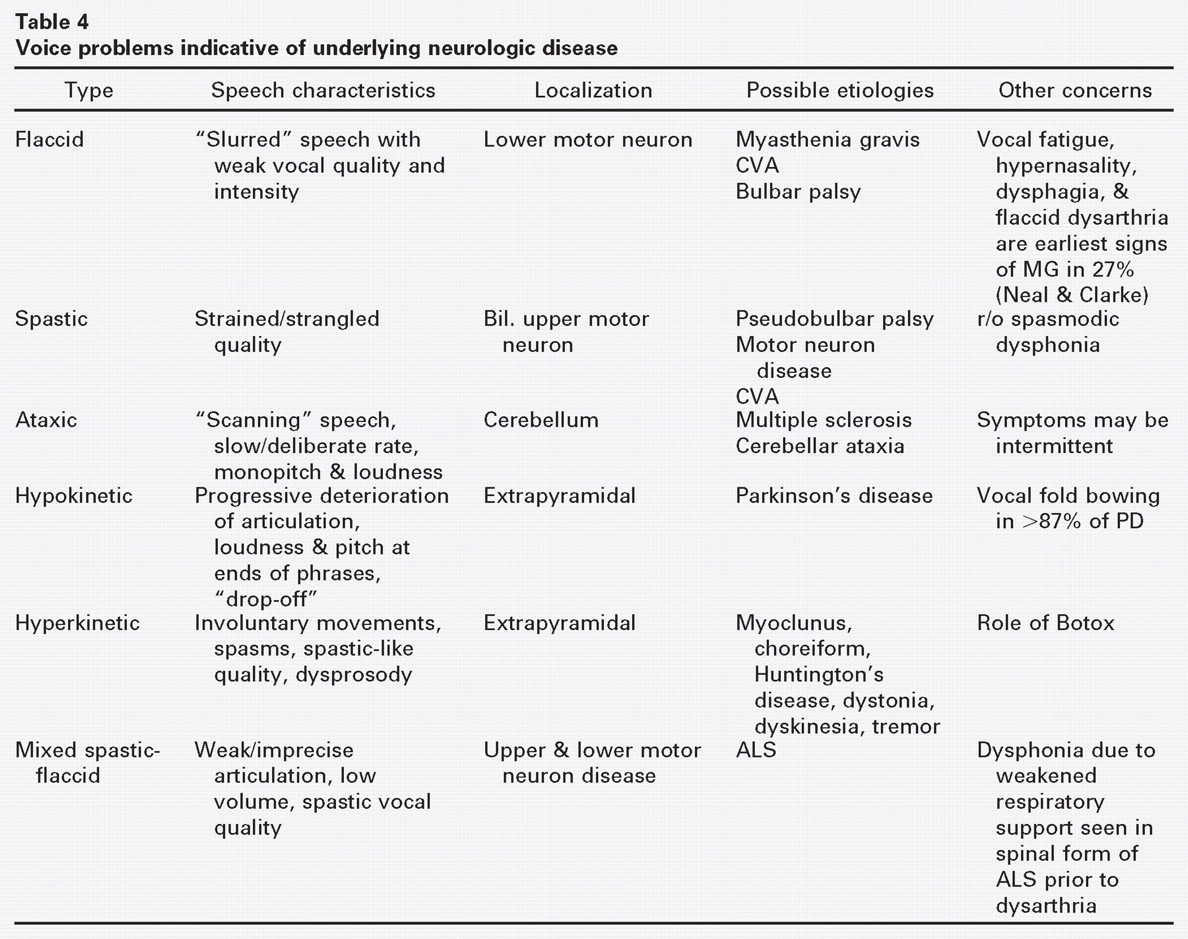
While the voice, speech, and swallowing are often affected in stroke, it is important to recognize the spectrum of other neurologic diseases that may affect these functions. Vocal symptoms of fatigue, hypophonia, unsteady tone, tremor, and hypernasality may signal the development of an underlying neurologic disorder. 21 Abnormal laryngeal and nasopharyngeal findings, including vocal fold bowing, abnormal movement patterns, and acquired velopharyngeal incompetence, may also herald the onset of a neurologic disease. Thus, it is important to recognize, identify, and differentiate between those vocal symptoms that are peripheral versus those that are more likely to indicate a central neurologic disorder to determine the most appropriate management.
Voice problems indicative of underlying neurologic disease
Common Themes in The Stroke Population
The typical stroke patient is elderly with multiple co-morbidities (Table 5). There are specific psychoneurologic morbidities commonly associated with stroke, namely dementia (alteration of cognition or intelligence), depression (alteration of mood), and aphasia (alteration of language). 28 , 29 Depression affects up to 40% of patients in the first two months after stroke, 30 which can interfere with rehabilitation and has been associated with higher mortality rates. The voice of a depressed patient is weak, with poor effort and endurance, made worse by dulled affect and a monotone quality.
Common themes in stroke patients
Indirect effects on the voice in stroke patients
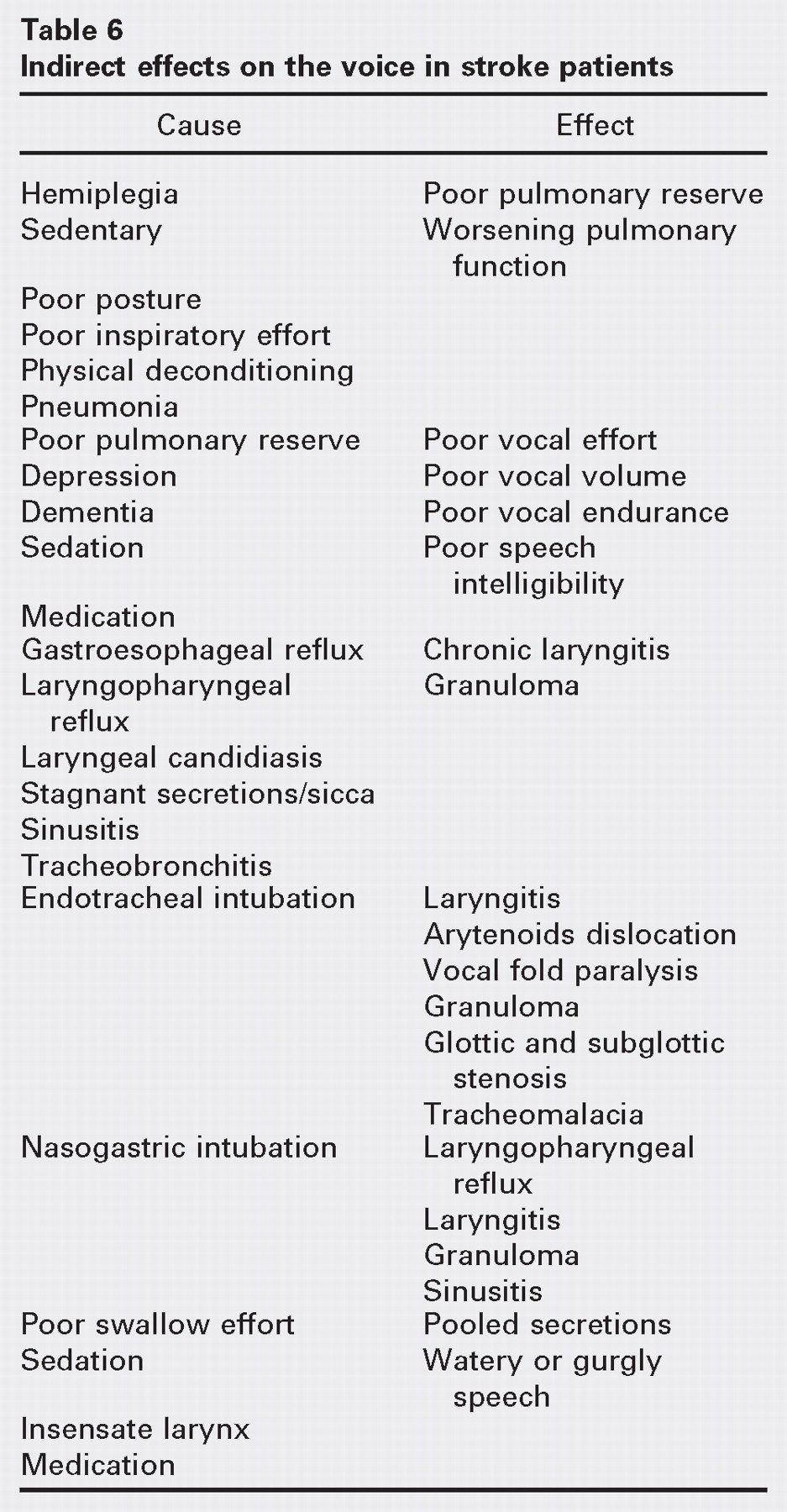
Table 6 summarizes causes and effects that stroke patients may have that contribute to voice problems. Prolonged hospitalization and rehabilitation is common. 31 Of note to the otolaryngologist, sleep-disordered breathing, primarily in the form of obstructive sleep apnea, can affect about 50% of patients following stroke. 32
Patients have both established neural pathways and neuroplasticity as mechanisms to recover from stroke, 33 so assessment and timing of intervention may vary over their clinical course. Attempts have been made to develop integrated care pathways, but outcome studies show no significant difference between patients who have been involved in these pathways as compared to controls. 34 It is important to recognize that each individual has a different disability and therefore different therapeutic goals. 35
Diagnostic Evaluation
The otolaryngologic management of the stroke patient should also attend to the roles of the larynx as prioritized by evolution: 1) protection, 2) respiration, and 3) phonation. Since secretion management is supremely important in protecting from aspiration, noting pooled secretions or gross aspiration on a larynx exam should raise the appropriate level of concern. While swallowing and dysphagia are not the primary focus of this paper, aspiration assessment is critically important in the evaluation of post-stroke laryngeal dysfunction as a whole.
Laryngeal Endoscopy
Laryngeal endoscopy, or preferably stroboscopy, is a key procedure in the diagnosis of vocal change in CVA. An initial perceptual evaluation yields information on the coordination of connected speech, articulation, and voice quality but cannot definitely diagnose the status of vocal fold function. Stroboscopy provides an assessment of mucosal wave details, which is the only way to identify subtle paresis or atrophy of the vocal fold. Sensation can also be tested by touching the endoscope tip to the arytenoids bilaterally, where a strong vocal fold closure should be elicited. Pooling of secretions in the hypopharynx suggests impairment of sensation or secretion management.
Laryngeal Electromyography
Laryngeal electromyography (LEMG) is helpful in the assessment of immobility of one or both vocal folds. Recent studies suggest utility in LEMG 6 weeks to 3 months following injury. 36 , 37 If there is evidence of early motor unit recovery, then a temporary procedure should be performed to assist with vocal rehabilitation. EMG is also useful to delineate swallowing problems at the level of the laryngeal sphincter and the cricopharyngeal sphincter and for supra-glottic/glottic sensation. 38 Additional testing of the cricothyroid (CT) muscle yields information about intact motor and sensory pathways to the supraglottis. The cricopharyngeal sphincter can be assessed, noting a normal innervation pattern that is active at rest, with a 400- to 600-msec relaxation period initiated by a swallow to allow for passage of the bolus followed by a second burst of activity. 39 A relaxation period less than 300 msec or evidence of EMG bursts suggests a diagnosis of CP spasm. 39
Dysphagia Examination
As discussed, dysphagia in CVA occurs in 22% to 65% of patients and can persist for many months, often resulting in a poor prognosis. 40 Not only the location but also the size of the stroke lesion predicts poorer outcome. 41 Dysphagia can result from weak or poorly coordinated pharyngeal muscular activity or from a lack of sensory detection necessary for safe bolus transfer. This can result in either frank aspiration or silent aspiration.
Swallowing impairments related to strokes may occur at multiple levels including: initiation of swallow, delay in oral bolus transfer, lack of pharyngeal muscular strength and coordination to propulse the bolus forward, lack of epiglottic tilt and incomplete laryngeal excursion in protecting the glottis, reduced tongue base movement, and cricopharyngeal dysfunction with incomplete relaxation. 42 Weakness of the velum and gag should alert the physician to the possibility of nasopharyngeal regurgitation. Spastic responses at this level are typically seen with bilateral upper motor neuron deficits. 43 Primitive reflexes such as rooting of the lips with gentle stroking of the cheek and blinking with glabellar tapping can also be elicited in settings of bilateral upper motor neuron lesions.
Bedside Swallow Evaluation is often the first step of a swallow evaluation and is typically performed by a speech language pathologist shortly after the CVA. The examination focuses on the ability of the individual to adequately protect the airway with a variety of substances with a focus on the coordination of respiration, speech, and swallow with varying food substances and bolus sizes. Features most suggestive of aspiration risk include a weak voluntary cough, wet phonation, cough with swallowing, absent gag response, or a prolonged swallow. 40 In many cases, the examination is not specific and underestimates the degree of dysphagia. 41 The reliability of bedside evaluation in this population is inconsistent, however. 40 , 44 – 46
Modified Barium Swallow (MBS) is the work horse for routine swallow assessment. MBS is performed by a radiologist, radiology technician, and speech and language pathologist with the patient in an upright position in the radiology suite. Evaluation includes bolus transfer from the oral cavity to the upper esophagus using barium in a variety of textures and portion sizes. Anterior-posterior and lateral projections yield a three-dimensional perspective and assist in pinpointing sites of dysfunction, as well as evaluating the efficacy of compensatory techniques in altering swallow dysfunction. 47
Studies suggest that even with better delineating of the site of swallow difficulty, that MBS may still miss 20% of patients with clinical aspiration. 48
Surgical and Treatment Options
Early supportive involvement from the interdisciplinary team is supremely important. The four major subdivisions in the treatment algorithm of laryngeal dysfunction in stroke are tracheotomy/airway management, dysphonia, dysphagia/aspiration, and secretion management.
Tracheotomy
Early tracheotomy in patients with anticipated prolonged ventilation provides an opportunity for early ventilator wean (due to decreased resistance respiring through a tracheotomy compared to endotracheal tube), quicker patient mobilization off the ventilator circuit, improved secretion management and pulmonary toilet, and decreased laryngeal complications of prolonged ventilation. Although the presence of the tracheotomy may have some minor effect on swallowing function, it is also an avenue to assess early swallowing ability and aspiration risk, since evidence of dyed food suctioned from the tracheotomy tube is an indication of aspiration when swallowing.
The ultimate goal is to downsize the tracheotomy tube, establish a safe upper airway while performing capping trials, and decannulate when aspiration and suctioning are no longer issues. One role of capping that has not been emphasized in the literature is the incompetence of the cough when a tracheotomy tube is not capped. A competent cough is designed to increase intrathoracic pressure while the glottis is closed, in order to produce an expulsive force during the glottal release. 11 When a tracheotomy tube is not capped, there is insufficient pressure to force out pulmonary secretions in an expulsive fashion. Therefore, tracheotomy patients often have a sense of pooled, stagnant, or “increased” secretions that seem to require more frequent suctioning.
Dysphonia
In the case of vocal fold paresis and/or paralysis, there is ineffective glottic closure with phonation. The options available for vocal fold medialization in this case include injection laryngoplasty, placement of a thyroplasty implant, nerve-muscle pedicle flap, arytenoid adduction, and arytenopexy. 52 – 55 If return of function is possible, then a shortterm alternative, such as injection medialization with dermal collagen, fat, or methylcellulose suspension is a consideration. 52 If return of function is unlikely, then a more permanent procedure such as thyroplasty, nerve-muscle pedicle flap, and/or arytenoidopexy should be considered. 53 – 56
Palatal myoclonus often results in ineffective and inconsistent velopharyngeal closure during speech, which can introduce a hypernasal quality to the voice. Laryngeal myoclonus can result in periodic bursts of vocal fold muscle activity, which can cause intermittent bursts of breathiness and breaks in the voice. Intelligibility of speech becomes difficult as a result of these myoclonic spasms. Both forms of myoclonus can be treated with the injection of Botulinum toxin type A into the affected muscles. In the palate, 7.5 to 10 mouse units on each side appears to be an effective dose for controlling these clonic bursts. In the larynx, 2.5 to 5 mouse units into each vocalis muscle appears to help control myoclonic activity. Dysarthria results from paresis or ineffective mobility of the tongue musculature. Speech therapy aimed at improving tongue coordination and mobility is the treatment of choice for dysarthria.
Dysphagia
Two emerging treatment modalities that have shown some promise in dysphagia rehabilitation include thermal-tactile stimulation and electrical stimulation. 57 – 59 While the fundamental approach of swallowing therapy is championed by the speech and language pathologist (SLP), the otolaryngologist may play a critical role in addressing incomplete relaxation of the cricopharyngeus. Treatment options include Shaker exercises, 60 injection of Botulinum toxin type A into the cricopharyngeus, cricopharyngeal myotomy, and cricopharyngeal dilatation. In patients with central nervous system insults and aspiration as a result of increased tonicity of the cricopharyngeal muscle, these options may improve swallowing, decrease pooling, and decrease the risk for penetration and aspiration. 61 , 62
Secretion Management
The inability to handle secretions can manifest as aspiration and/or drooling and can be caused by poor oro-motor control, vocal fold paresis/paralysis, and/or poor oropharyngolaryngeal coordination of swallowing. This may be treated by resection of the submandibular gland, ligation of Stensen's ducts, and tympanic neurectomy. However, less-morbid techniques include Botulinum toxin type A injections at doses of 50 to 65 mouse units into each parotid and submandibular gland, which have been shown to result in significant control of hypersalivation. 63
Management of secretion aspiration may be aided by vocal fold medialization (injection or thyroplasty), arytenoid adduction, and cricopharyngeal myotomy when indicated. 64 , 65 In patients where paralysis of the pharyngeal muscles contribute to the pooling of secretions in the piriform sinuses, removal of redundant hypopharyngeal tissue may decrease such pooling and improve pharyngeal transit time. 66
Placement of a feeding tube, maintaining nothing by mouth status, and aggressive pulmonary toilet may be indicated in cases refractory to treatment. It must be noted that secretions and thin liquids will still bypass the cuff in the tracheotomy tube, making aggressive pulmonary toilet an important aspect of this treatment plan. 67 Tracheoesophageal diversion and laryngotracheal separation are more radical options when complications of aspiration persist in these patients. 68
Conclusion
This paper presents the scope of practice and otolaryngologists' role in the care of the stroke patient, particularly with regard to the voice and laryngeal dysfunction. Many aspects of this paper are also applicable to the rehabilitation patient, including those with head injuries, spinal cord injuries, and other protracted hospitalizations. While the diagnostic, management, and therapeutic regimens discussed are clearly important for patient rehabilitation, there is a paucity of outcome studies. These would be difficult to perform in a controlled fashion because of the many variables in the co-morbid patient population and high risk of subsequent stroke and mortality, as well as ethical issues regarding withholding the likely beneficial effects of therapy. Ultimately, clinical pathways for this population are expected to improve standardization of care and cost-effective treatment.