
Abstract
OBJECTIVE: We sought to review the presentation, evaluation, and treatment of branchial anomalies in the pediatric population and to relate these findings to recurrences and complications.
STUDY DESIGN AND SETTING: We conducted a retrospective study at a tertiary care pediatric hospital.
PATIENTS: Ninety-seven pediatric patients who were treated for branchial anomalies over a 10-year period were reviewed. Patients were studied if they underwent surgical treatment for the branchial anomaly and had 1 year of postoperative follow-up; 67 children met criteria, and 74 anomalies were studied. RESULTS: Patients with cysts presented at a later age than did those with branchial anomaly fistulas or sinus branchial anomalies. 32% of branchial anomalies were previously infected. Of these, 71% had more than one preoperative infection. 18% of the BA were first arch derivatives, 69% were second arch derivatives and 7% were third arch derivatives. There were 22 branchial cysts, 31 branchial sinusies and 16 branchial fistulas. The preoperative and postoperative diagnoses differed in 17 cases. None of the excised specimens that contained a cystic lining recurred; all five recurrences had multiple preoperative infections.
CONCLUSIONS: Recurrence rates are increased when there are multiple preoperative infections and when there is no epithelial lining identified in the specimen.
STUDY DESIGN
A retrospective study was designed to review all the patients treated for a BA by the senior author (J.M.) at the Children's Memorial Hospital in Chicago during the 10-year period from January 1996 through June 2005. Study patients had care supervised by the senior author, had a preoperative diagnosis of a BA, were under 18 years of age at the time of diagnosis, and had received surgical treatment for the con-dition. The purpose of this study is to define the relationship of presentation, work-up, and treatment of BAs in the pe-diatric population to recurrences and complications.
MATERIALS AND METHODS
Approval from the institutional review board at Children's Memorial Hospital was obtained before beginning this study. Basic demographic information for each patient was recorded, including gender, age at presentation, and age at surgery. The means by which the patient came to the attention of the senior author was noted. The presenting history and physical examination, clinic notes, and radiological reports were reviewed. The preoperative diagnosis was based on history, clinical examination, and radiology reports. The diagnosis was categorized based on the suspected arch of origin and then further subdivided into cyst, sinus, or fistula. The postoperative diagnosis was determined by intraoperative findings and histologic pathology. The histological data were recorded and compared with the diagnosis. Complications were determined to be minor and major, with minor complications not requiring surgical intervention; these included hematoma or seroma formation, wound infection, and temporary nerve injury. Major complications were defined as those requiring surgical intervention and/or causing a permanent morbidity; these included recurrence, hypertrophic scar formation, and permanent nerve injury.
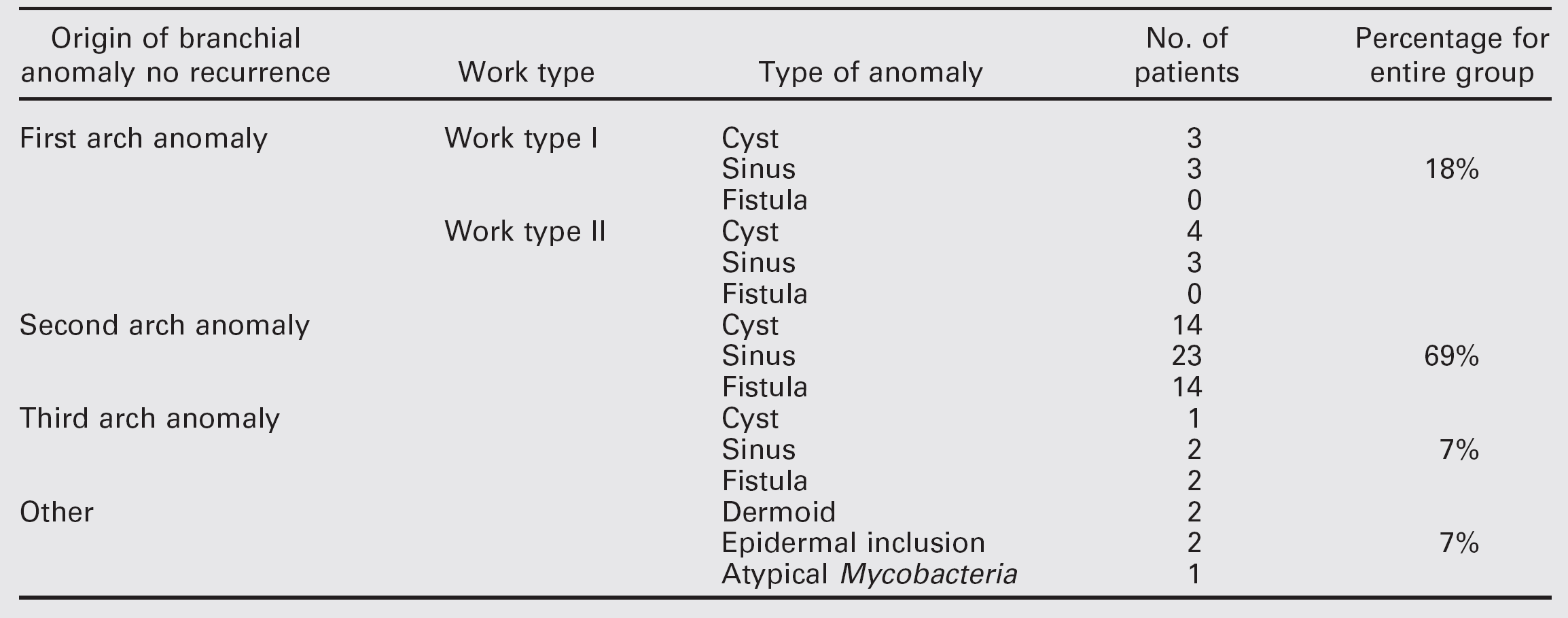
Summary of branchial anomalies based on post-operative diagnosis
RESULTS
Sixty-seven children met the criteria for inclusion. There were 32 females and 35 males. Bilateral BAs were seen in seven children, two males and five females, resulting in a total of 74 BAs. The anomalies were divided evenly between the right (37) and the left (36) sides.
Presentation
Eighty-eight percent of patients came to the attention of the senior surgeon as a referral by a primary care physician for evaluation of a suspected BA. Only 8% of the children were evaluated in the emergency department for a neck mass, and 4% of the children initially presented for another, unrelated complaint. The average age of presentation for a cyst was 4.1 years, 3.6 years for a sinus, and 2.6 years for a fistula. Forty-five percent of anomalies studied presented with a lateral neck mass. Only five presented with an abscess, of whom 80% had a history of multiple infections. Of the BAs, 32% had a history of previous infections; 71% had more than one. A total of 46 anomalies presented with a skin opening located close to the anterior border of the sternocleidomastoid muscle. Twenty-eight were ultimately diagnosed as sinuses and 16 as fistulas. Of the anomalies with a skin opening, 85% presented with drainage and 35% presented with a history of infection. For those with both a lateral neck skin opening and drainage, 59% were ultimately diagnosed as a sinus and 37% as a fistula. Significant past medical history included four children born premature, one had hydrocephalous, one had fetal alcohol syndrome, and one diagnosed with branchio-oto-renal syndrome.
Imaging
Preoperative radiographic images were obtained on 63 BAs. Computed tomography (CT) scanning with contrast was performed on 90% of the patients, while 2% had an ultrasound; 6% underwent both. One anomaly was investigated using a CT scan without contrast. In no patient was barium esophagraphy or magnetic resonance imaging performed. Eleven had no preoperative imaging study. Based on the imaging, the preoperative diagnosis of a BA was correct in 93% of the cases. Diagnosis of the type of anomaly within each arch, however, was accurate in only 75% of the cases. More specifically, using CT scanning, cysts were accurately diagnosed in 95% of cases, sinuses were diagnosed correctly in 81% of the cases, and fistulas were diagnosed correctly in 50% of cases.
Diagnosis
The preoperative diagnosis was based on the patient's history, physical examination, and radiographic studies. The postoperative diagnosis was based on the intraoperative findings and postoperative histopathology. The presence and location of a skin opening, the course of a fistula tract in relation to surrounding neurovascular structures, and the presence and location of a mucosal opening all helped define the diagnosis. Eighteen percent of the BAs were first arch derivatives, 69% were of second arch origin, and the remaining 7% were third arch anomalies. There were no fourth BAs identified in this series. The preoperative and postoperative diagnoses differed in 17 patients. First BAs were correctly diagnosed in 92% of cases. Second and third BAs were correctly diagnosed preoperatively in 76% and 60% of cases, respectively. Five patients with lesions initially diagnosed as BAs were given a different diagnosis postoperatively based on histopathologic findings. One patient was diagnosed with atypical mycobacterial adenitis, two were discovered to have a dermoid cyst, and two were diagnosed with an epidermal inclusion cyst. In summary, there were 22 (30%) branchial cleft cysts, 31 (42%) sinuses, and 16 (22%) fistulas. The results are outlined in Table 1.
Histology
All of the Work type I first BAs were composed of a cyst lined by keratinizing squamous epithelium. Five of the six Work type II first BAs contained a cyst lined by keratinizing squamous epithelium along with cartilage. The sixth one contained only keratinizing squamous epithelium. Of the second and third BAs that contained an epithelial lining, 19 consisted of nonkeratinizing squamous epithelium, while 19 other lesions had pseudostratified columnar respiratory epithelium. No cystic lining was seen in 28% of the second and third arch specimens. Seven had a combination of both. One of the third branchial cleft sinus specimens contained thymic tissue. None of the excised specimens that contained a cystic lining on histopathologic review were associated with a recurrence. All five recurrences had no epithelial lining identified at the time of the original excision. How-ever, adnexal tissue and lymphoid tissue were seen in these cases.
Complications
There were eight minor complications that did not require surgical intervention. Wound infections developed following the initial surgical resection in five cases, two in one patient who had bilateral BA. These were treated with antibiotics and resolved. There was one seroma that became infected but resolved without surgical intervention. No patient developed a hematoma. One patient had a temporary twelfth nerve paresis that resolved after 3 months. One patient had a stitch extrusion that did not become infected and required no treatment.
There were nine major complications that required surgical intervention and/or resulted in permanent morbidity; these included three hypertrophic scars, one keloid, and five recurrences. Of the five recurrences, all had multiple pre-operative infections and four had a skin opening at the time of presentation. Three were on the left, and two were on the right. The initial surgical specimens from the anomalies that recurred lacked a cystic lining and contained no identifiable squamous or respiratory epithelium. All recurrences were treated with re-excision. The histopathology of the re-excised specimens was reviewed. Of these, three contained a cystic tract lined by squamous epithelium, one contained a suture granuloma, and one was diagnosed as an epidermal inclusion cyst. Based on histology and intraoperative findings, the re-excised anomalies were ultimately diagnosed as a Work type I first arch sinus, a Work type II first arch sinus, and two second arch sinuses. One was diagnosed as an epidermal inclusion cyst and not as a BA.
DISCUSSION
BAs can present as a cyst, sinus, or fistula and result from developmental abnormalities of the branchial apparatus during the embryologic period. It is a misnomer to use only the word “cleft” when describing these congenital malformations, as this implies that there is no contribution from the branchial arch or pouch. The branchial apparatus consists of grooves (ectoderm), arches (mesoderm), and pouches (endoderm). 2 A sinus forms when a groove or pouch fails to obliterate and subsequently communicates with either the skin or the mucosa, respectively, of the upper airway. A fistula results when both a groove and a pouch fail to obliterate, causing a continuous communication between the mucosa and the skin. A cyst is created when a branchial groove remnant forms an epidermis-lined space without a communication to the skin or mucosa. Branchial complexes 2, 3, and 4 fuse into one structure referred to as the sinus of His. This is formed by the overlapping second arch's ventral pole, which becomes the platysma muscle. It is generally accepted that most BAs are derived from remnants of this sinus. 3 It is important that the surgeon treating these anomalies have a comprehensive understanding of their origin. The embryology of BAs is well described in the literature and will not be presented here.
BAs typically present in infancy and childhood but can be diagnosed for the first time at any age. A sinus or fistula tends to be diagnosed earlier than a cyst due to the obvious skin opening and associated drainage and infection. 4 In this study, the average age of diagnosis of a fistula and sinus was 2.6 years and 3.6 years, respectively. The average age of diagnosis for a cyst was 4.1 years. Furthermore, sinuses and fistulas were more likely to have presented with infection (67%) compared with the cysts (21%). A majority of the fistulas and sinuses were diagnosed by primary care providers and referred to the senior surgeon (J.M.) for definitive management after a period of watchful waiting. The average age at surgery was 2.8 years for a fistula, 4.5 years for a sinus, and 4.9 years for a cyst.
Males and females were equally affected by BAs in this study. The lesions reviewed here were also equally distributed between the right and left sides of the neck. However, it has been reported that third and fourth BAs have a strong predominance for the left side due to the asymmetry of the transformation of the fourth branchial arch to form the aorta and the innominate arteries. 5 In this study, there was no fourth BA, and of the five third arch BAs, three were on the left side of the neck while two were on the right.
First arch BAs are rare. Typically, only 1-8% of all BAs are derived from the first arch. 6 We present a higher rate of 18%. However, previous studies have reported rates as high as 25%. 7 Second arch BAs are the most common of all BAs. We report 69% of our population as having BAs derived from the second arch.
Clinical examination alone is only 50-60% accurate when used to make the diagnosis of a second BA. 8,9 The presence of a skin opening is a common clinical finding. In our study, 62% of the BAs presented with a lateral neck skin opening in which 84% had at least one episode of drainage. Forty-five percent of our patients presented with a lateral neck mass. The differential diagnosis as determined by the location of the lesion should include tuberculosis adenitis, lymphadenitis, abscess, lipoma, cystic hygroma, hemangioma, lymphoma, ectopic thyroid and thyroglossal duct cysts, cervical thymic cyst, and parotid neoplasm. Ectodermal malignant neoplasms are uncommon in the pediatric population but should be considered in the work-up of a cystic neck mass in the adult population.
(
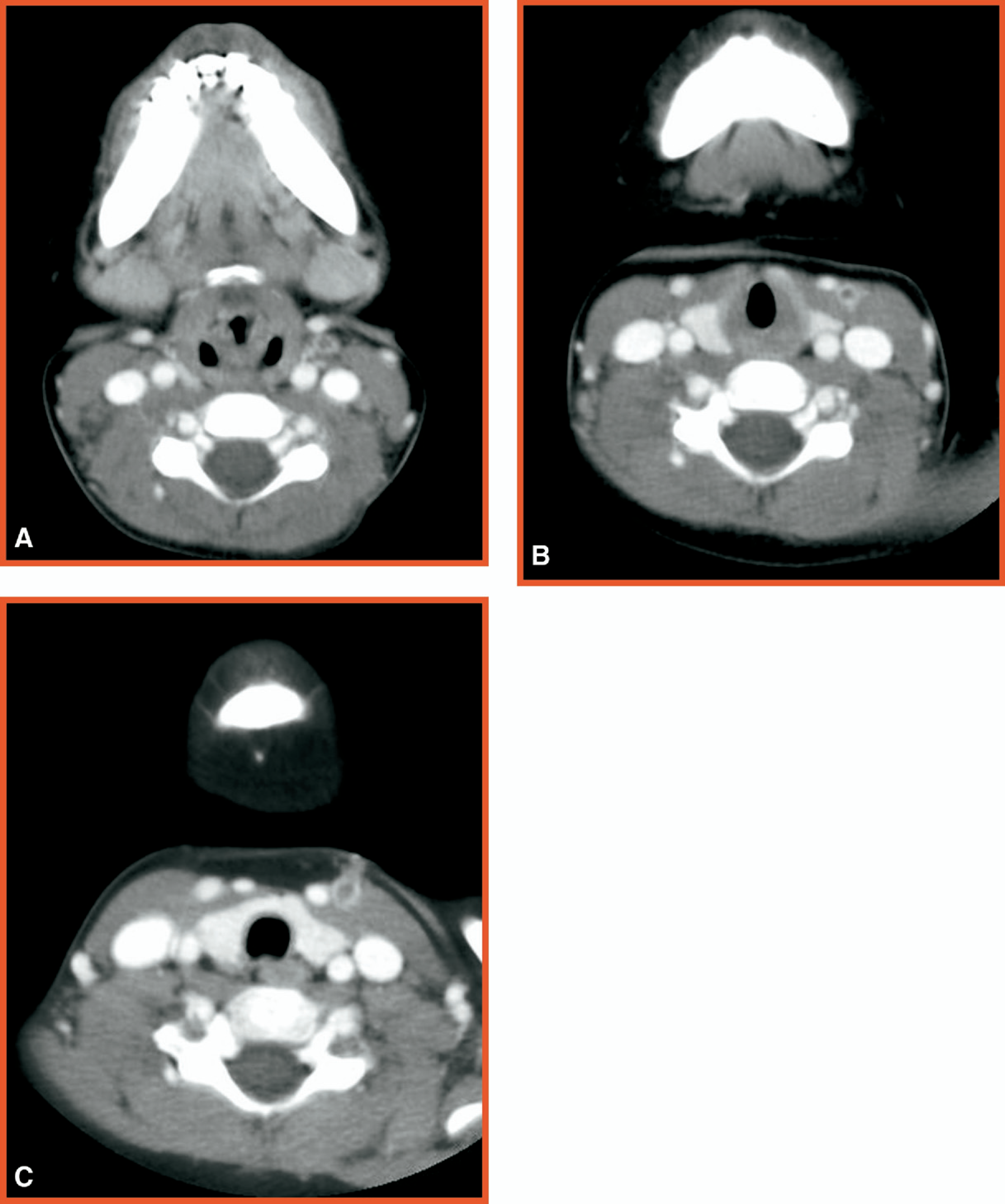
The use of radiographic imaging to assist with the diagnosis of BA has been well documented. 10 A CT scan with contrast can define the anatomy of a fistula or cyst along with the surrounding structures, thereby aiding in the complete surgical excision of the lesion. 11 This is demonstrated in Figure 1, where the outline of a left sided second arch fistula can clearly be followed from the skin to carotid bifurcation. However, the sensitivity of the CT scan to differentiate a fistula or sinus from an isolated cyst or remnant has not been determined. In this study, the accuracy of a CT in diagnosing a sinus and fistula was 81% and 50%, respectively. Furthermore, infants and children often require sedation or even general anesthesia when undergoing this procedure. Ultrasonography, on the other hand, can also be used to aid with preoperative diagnosis. BAs appear as well-defined, smoothly outlined, and uniformly anechoic lesions with posterior enhancement. 12 Yet BAs often have variable sonographic appearances, which may lead to confusion. 13 Cysts can be distinguished from lymphadenopathy with the use of color flow Doppler. 12 Preoperative fistulography using thin barium has also proved helpful in defining the anatomy of a fistula or sinus. 14 However, inflammation, scarring, and recent infections can lead to false-negative results. Performing a direct laryngoscopy in conjunction with a thin barium swallow can increase the rate of preoperative piriform sinus fistula identification to nearly 100%. 15 However, it is not clear that these procedures will reduce the recurrence rate. We report 16 fistulas, and none of the patients underwent barium swallow or direct laryngoscopy. All had complete surgical excision by dissecting the fistula up to its entrance into the pharynx, and there were no recurrences. These patients had at least a 2-year follow-up. Our study found the imaging modality had no relationship to complication or recurrence rate. Although imaging is often necessary to differentiate a BA from other lesions, we found no single radiographic technique that was helpful in determining the type of BA present in each case. CT scanning alone was accurate in diagnosing the type of BA in 75% of the time. Rather than use multiple imaging modalities for each patient, it is the practice of the senior author (J.M.) to use CT scanning or ultrasonography to confirm the diagnosis of BA when it is in doubt.
The sinus tracts of BAs are typically lined by stratified squamous epithelia, which may be replaced in some areas with respiratory epithelium. 16 Additionally, considerable quantities of subepithelial lymphoid tissue in a follicular pattern are often seen. We reviewed 13 first BAs that were evenly distributed between Work type I and type II. All of the type I anomalies were composed of squamous epithelium, consistent with their ectodermal origin as a duplication of the membranous external auditory canal. 17 All except one of the type II anomalies were composed of squamous epithelium and cartilage, which is also consistent with their combined ectodermal and mesodermal origin as a duplication of membranous and cartilaginous external auditory canal. Second and third arch anomalies were composed of respiratory or squamous epithelium in equal quantities. Thirty percent of these lesions were composed of both types. The presence of thymic tissue (third arch) or thyroid tissue (into which fourth arch derivatives incorporate) in the tract can also help determine the BA of origin. 18 One third branchial sinus specimen contained thymic tissue. The thymus and inferior parathyroid glands are derivatives of the third branchial arch; therefore, their association with these anomalies is often seen. 19 There were no recurrences among the patients in which excised specimens contained a cystic lining; all five that did recur had no epithelial lining seen on final histopathology. Three of the re-excised specimens contained a cystic tract lined by squamous epithelium. There were five lesions that were misdiagnosed as BAs preoperatively. Two lesions were ultimately diagnosed as dermoid cysts and two other lesions were diagnosed as epidermal inclusion cysts. One lesion proved to be an atypical mycobacterial infection. After re-excision, no further surgery was needed in all recurrent cases.
Definitive treatment for branchial cysts, sinuses, and fistulas is complete surgical excision. If not removed, these lesions do not spontaneously regress and can have recurrent infections. The timing of surgery is dependent on the age of the patient and the presence of infection. Ideally, surgery is performed before infections occur and distort the surgical planes of dissection and hinder the complete excision. We determined that sinuses and fistulas are more likely to become infected preoperatively than cysts (67% vs 21%, respectively). This may influence the timing of surgical excision. Early excision may obviate the need for a drainage procedure and multiple courses of antibiotics. Of the 17 anomalies reviewed that were infected preoperatively, only 2 occurred before 1 year of age. In all five of the recurrences reviewed, there was a history of multiple infections. As a result, the senior author prefers to schedule elective surgical excision at 1 year of age or after the acute infection has resolved. Infections were aggressively treated with intravenous antibiotics, reserving incision and drainage procedures for recalcitrant cases.
The surgical technique for complete excision of these lesions has been standardized by the senior author. For first BAs, intraoperative facial nerve monitoring is performed in conjunction with a standard parotidectomy incision and facial nerve dissection. The dissection rarely extends 1-2 cm past the division of the facial nerve. Occasionally, the incision needs to be extended into the neck. If the tract leads into the cartilaginous portion of the external auditory canal, a small portion of cartilage is resected and the canal is packed for several weeks. We found no cases of postoperative external auditory canal stenosis. Patients with suspected second, third, or fourth BAs undergo a lateral neck exploration, including exploration of the carotid sheath up to the lateral pharyngeal wall (Fig 2A). Even if no fistula is identified on preoperative radiography, one is still looked for during surgical dissection (Fig 2B). We found no in-creased recurrence rate of dissected branchial fistulas when preoperative laryngoscopy or barium swallow studies were not used. The fistulous tract is followed into its pharyngeal opening and suture ligated. Third branchial remnants require dissection in the tracheoesophageal groove and occasionally necessitate resection of a small portion of the lateral thyroid cartilage. Patients with direct thyroid involvement, a thyroid mass, or thyroiditis require a hemithyroidectomy. Transoral obliteration of a pyriform sinus opening is rarely necessary and has not been used by the senior author. High suture ligation of the tract at its end point in the neck is sufficient. By using these techniques, no permanent nerve injury or other morbidity associated with dissection has occurred.

(
CONCLUSIONS
Branchial complex anomalies are a common cause of pediatric neck masses. The diagnosis is primarily based on history and physical examination findings. Sinuses and fistulas are more likely to become infected before excision than are cysts. Radiographs, particularly CT scans with contrast and ultrasonography, should be used to differentiate BAs from other neck lesions. Extensive work-up to determine the exact type of BA preoperatively may have no effect on recurrence rate. All 16 fistulas presented were excised without the use of a preoperative laryngoscopy or thin barium swallow, and there were no recurrences. Barium swallow studies should be reserved for recurrent cases. Surgical excision is the definitive treatment and is ideally performed after the patient reaches 1 year of age or before repeated infections occur. Aggressive medical management of infections is used, reserving incision and drainage procedures for recalcitrant cases. Lack of identification of an epithelium-lined tract on the postoperative specimen is the most sensitive predictor for recurrence.
FINANCIAL DISCLOSURE
None.