
Abstract
The lateral pharyngoplasty, first described by Cahali, 1 was aimed at addressing the lateral pharyngeal wall collapse in patients with OSA. The procedure showed promising results; however, many patients had dysphagia postoperatively.
The ideal procedure would involve one that is easy to perform, has low morbidity and minimal complications, and does not require any special equipment.
Orticochea 6 was first to describe the construction of a dynamic muscle sphincter, by isolating the palatopharyngeus muscle, and apposing them bilaterally superiorly in the midline, for the treatment of velopharyngeal incompetence in patients with cleft palates. The modified Orticochea procedure was described by Christel et al 7 ; the procedure differed by isolating the palatopharyngeus muscle bilaterally, apposing them more superiorly and closing the lateral pharyngeal defects with Z-plasty sutures. Using these procedures, the authors present an innovative technique in creating this tension in the lateral pharyngeal walls, preventing its collapse and reducing the number of apneic episodes. The expansion sphincter pharyngoplasty basically consists of a tonsillectomy, expansion pharyngoplasty, rotation of the palatopharyngeus muscle, a partial uvulectomy, and closure of the anterior and posterior tonsillar pillars. Our hypothesis was that the expansion sphincter pharyngoplasty technique is superior to the traditional uvulopalatopharyngoplasty (UPPP) in patients with small tonsils and significant lateral pharyngeal wall collapse.
MATERIALS AND METHODS
A prospective randomized clinical trial was conducted in 45 consecutive patients. All patient were adults (older than 18 years) who have type I Fujita (retropalatal obstruction) and lateral pharyngeal wall collapse noted on flexible nasoendoscopy. The inclusion criteria included patients with small tonsils (tonsil size 1 and 2), body mass index (BMI) less than 30 kg/m 2 , and Friedman clinical stage II and III who cannot tolerate nasal continuous positive airway pressure (CPAP) therapy or for whom CPAP therapy failed. All patients underwent a thorough clinical examination that included height and weight measurements, neck circumference, BMI, and assessment of the nasal cavity, posterior nasal space, oropharyngeal area, soft palatal redundancy, uvula size and thickness, tonsillar size, and Friedman tongue position. Flexible nasoendoscopy was performed for all patients, and collapse during a Mueller's maneuver was graded for the soft palate, lateral pharyngeal walls, and base of tongue on a 5-point scale. 3 Patients with small tonsils, Friedman clinical stage II or III, type I Fujita, and lateral pharyngeal wall collapse seen on endoscopy were randomized into either the traditional UPPP procedure or the expansion sphincter pharyngoplasty (ESP). All patients had only palatal surgery with no hypopharyngeal surgery. Patients with large tonsils were excluded because we know, from Friedman's clinical staging of OSA, that patients with large tonsils have a 80% success rate with traditional UPPP; hence, use of this new technique (ESP) on patients with large tonsils will not justify good results if they are obtained. The mean follow-up was 6.5 months. All patients had a postoperative polysomnogram at 6 months. The study was approved by the institutional review board, ethics committee in the institution.
Surgical Technique
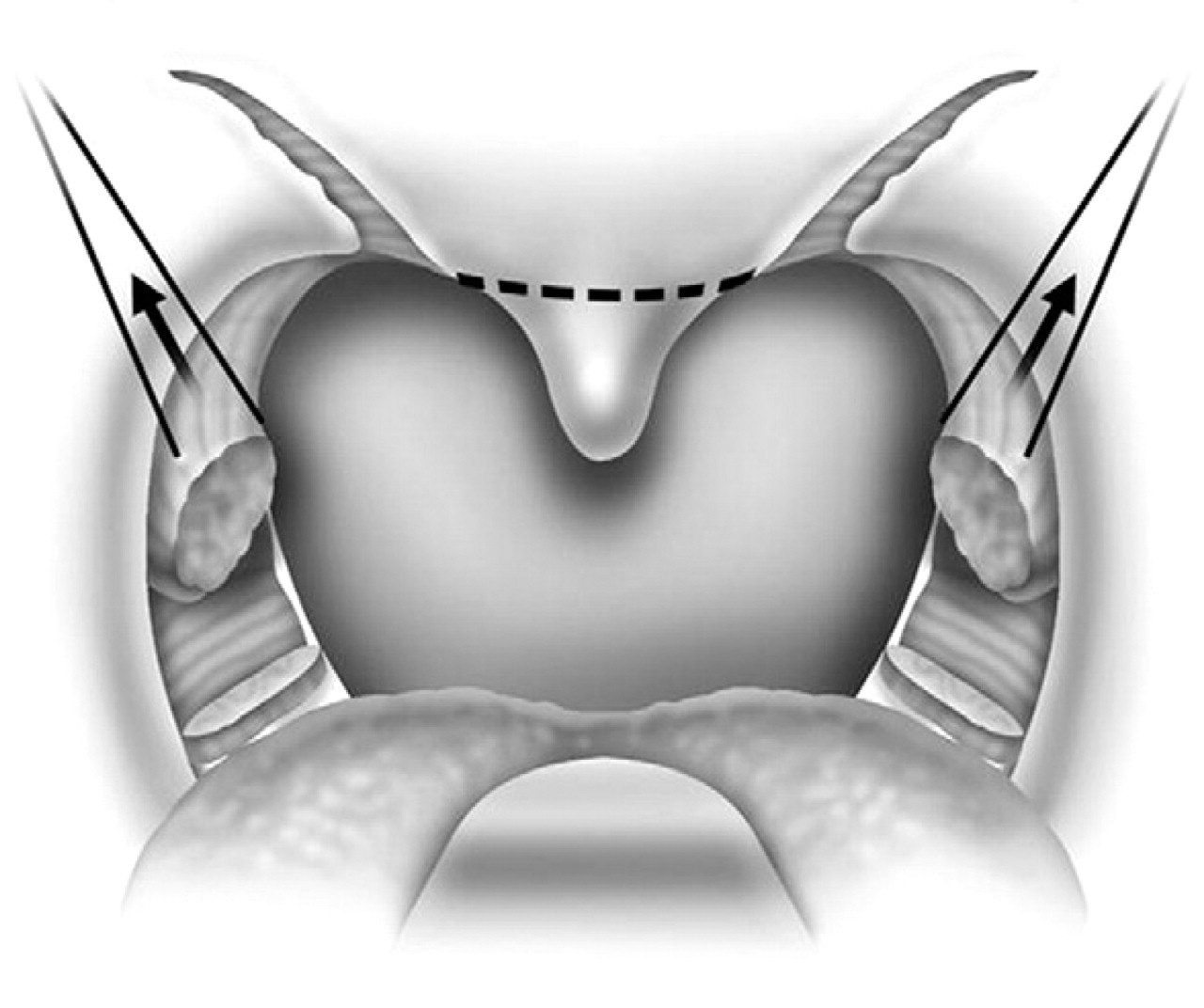
The procedure is performed under general anesthesia, with the patient in the supine position. The authors perform the procedure with orotracheal intubation, with a Boyle-Davis mouth gag within the oral cavity to keep the mouth open, and with isolation of the endotracheal tube forward. A bilateral tonsillectomy is performed (Fig. 1). The palatopharyngeus muscle is identified; its inferior end is transected horizontally (Fig. 2) and rotated superolaterally with a figure 8 suture, through the muscle bulk itself, with a Vicryl 3-0 round body needle. The muscle is isolated and left with its posterior surface partially attached to the posterior horizontal superior pharyngeal constrictor muscles (Fig. 3). Sufficient muscle has to be isolated to mobilize the muscle and to allow suturing of the muscle with the Vicryl suture. A superolateral incision is made on the anterior pillar arch bilaterally, identifying the arching fibers of the palato-glossus muscles (Fig. 4). The palatopharyngeus muscle is then attached to the arching fibers of the soft palate anteriorly with a figure 8 suture, through the muscle bulk itself, with a Vicryl 3-0 round body needle (Fig. 5). A partial uvulectomy is then performed. The anterior and posterior tonsillar pillars are then apposed with Vicryl sutures. The same steps are repeated on the opposite side (Fig. 6).
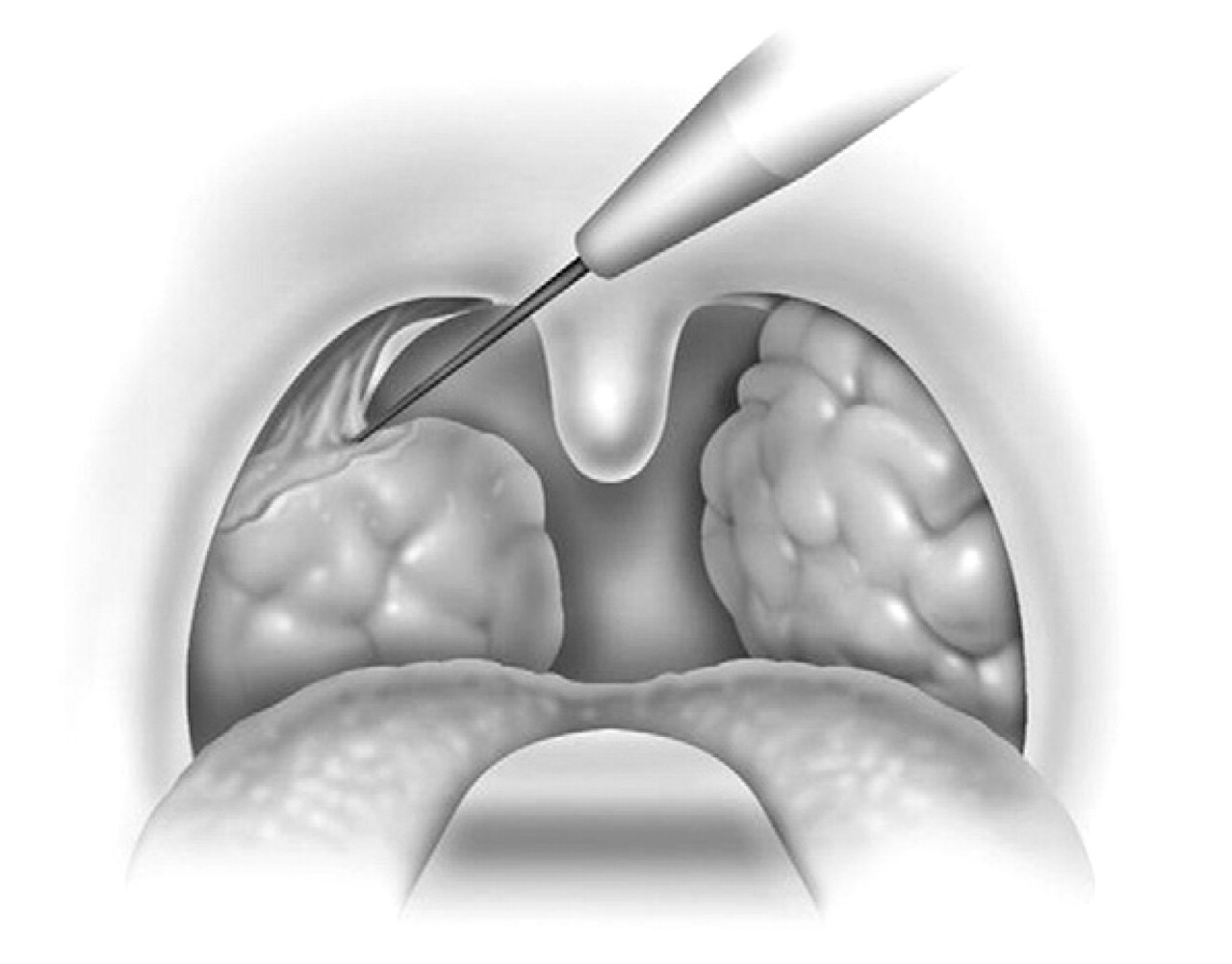
Tonsillectomy is performed.
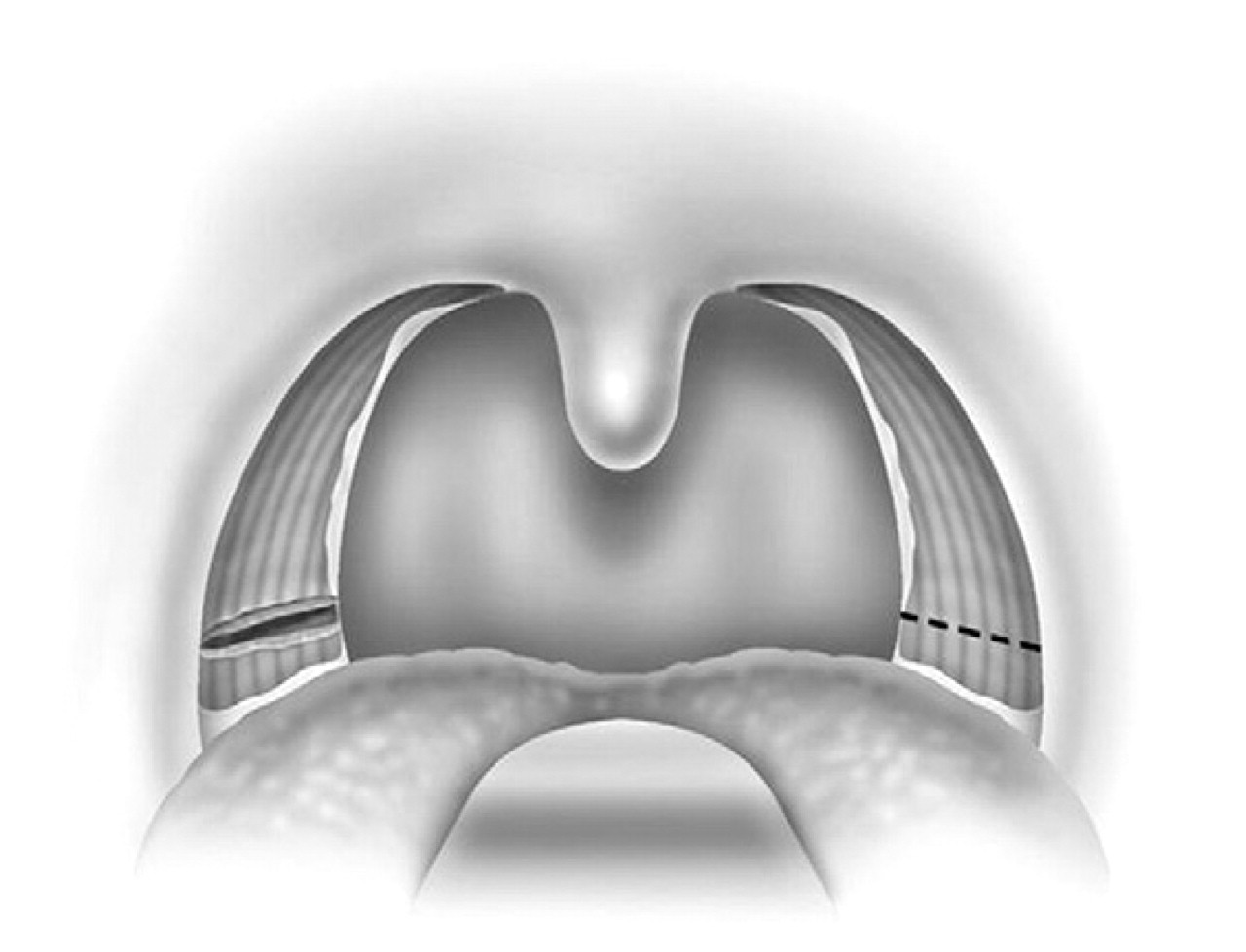
Horizontal incision made to divide the inferior end of the palatopharyngeus muscle.
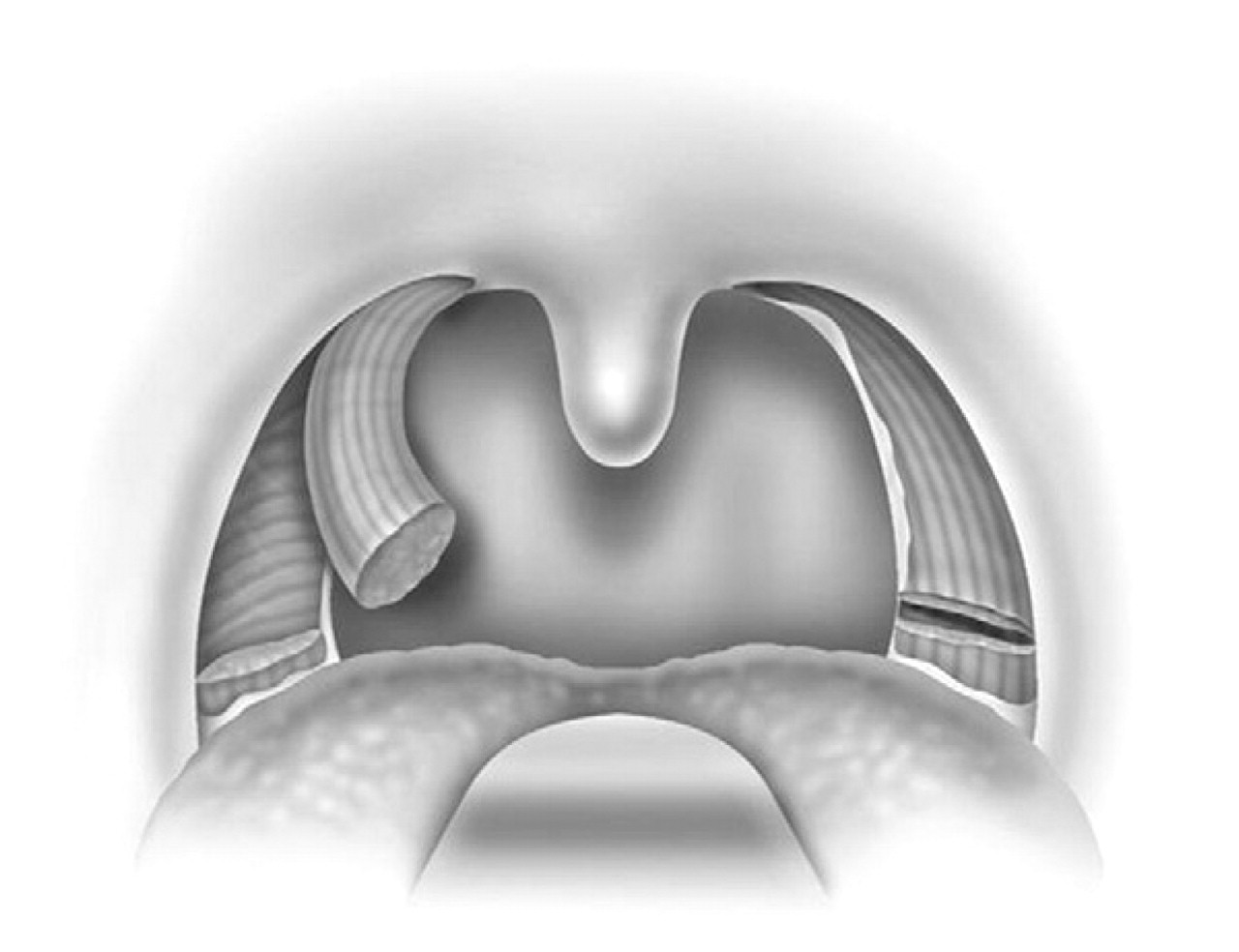
The palatopharyngeus muscle is mobilized, although not completely, with care taken to leave its fascia attachments to the deeper horizontal constrictor muscles.
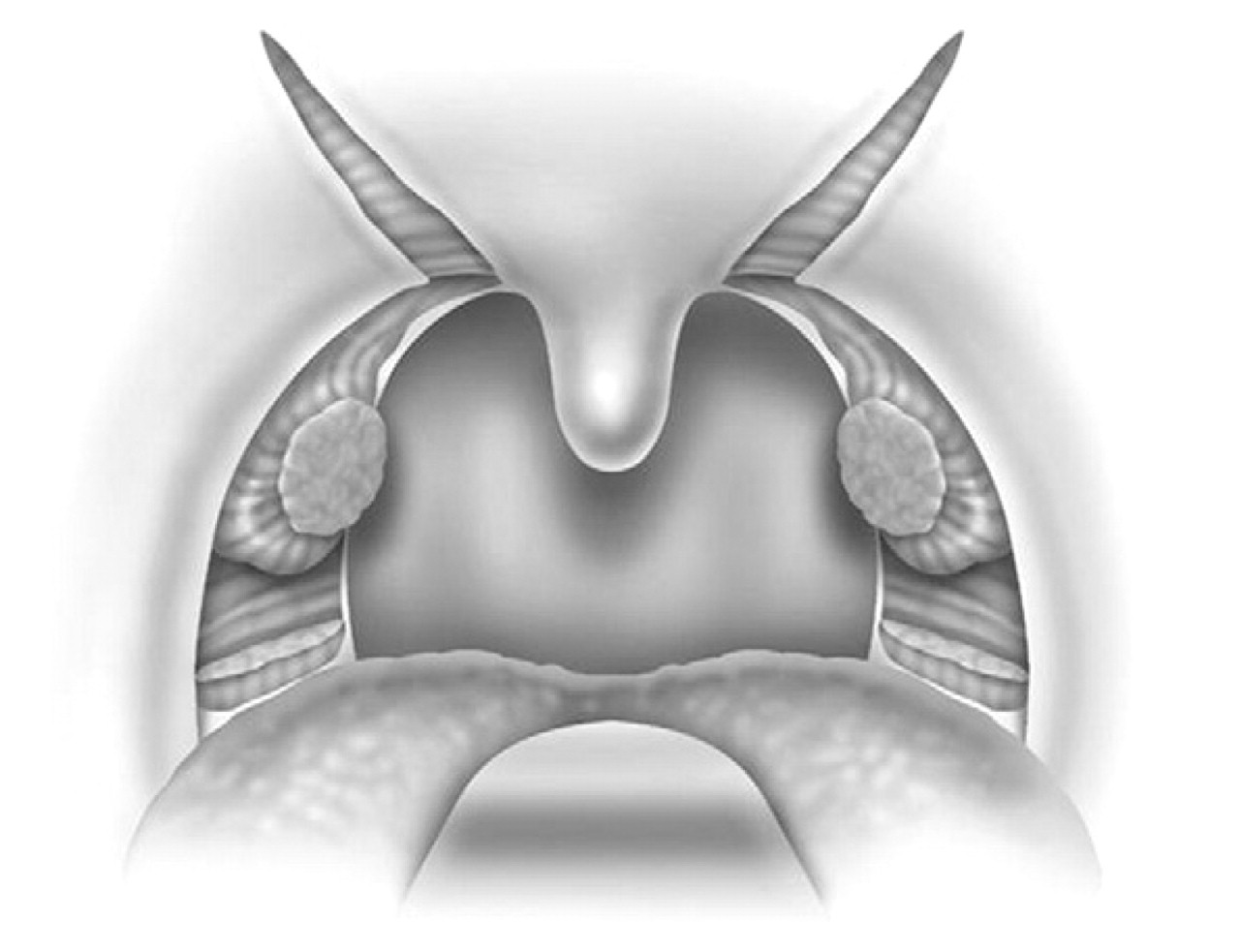
Superolateral incision made on the soft palate, revealing the arching fibers of the palatini muscles.
All patients were monitored in the postanesthesia care unit for 4 hours before being transferred to the high dependency ward for overnight monitoring. Monitoring included continuous pulse oximetry, blood pressure, and pulse rate. They were given adequate analgesia, in the form of anesthetic gargles (Difflam) and lozenges (Difflam), nonsteroidal anti-inflammatory agents (naproxen sodium), and cyclo-oxygenase 2 inhibitors. Most patients were discharged on the first postoperative day. All patients were encouraged to consume adequate oral fluid hydration and a soft blended diet in the first postoperative week. There were no complications from this procedure; there were no primary or secondary hemorrhages, and there were no fistulas of the soft palate or oral infections.
RESULTS
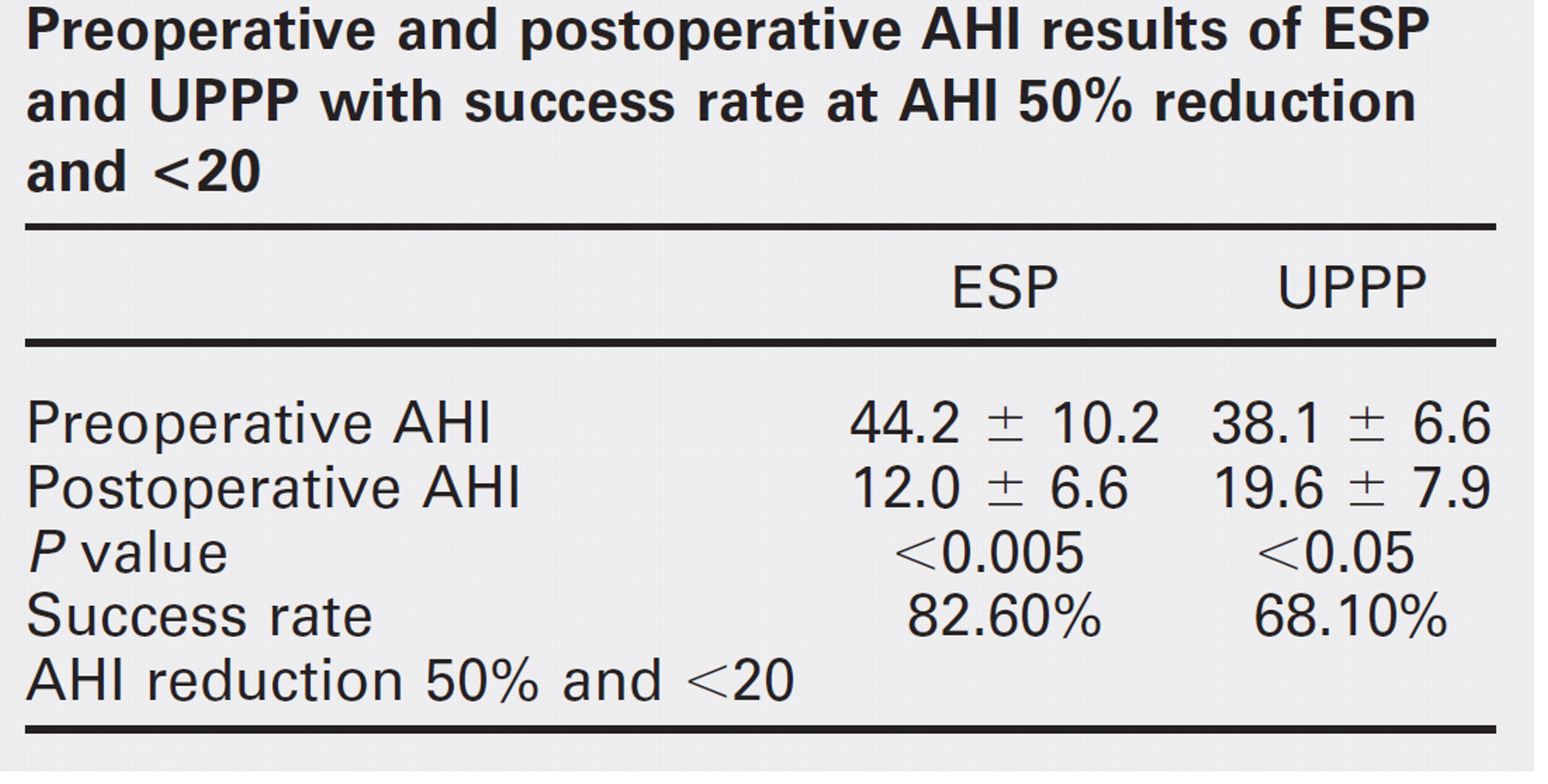
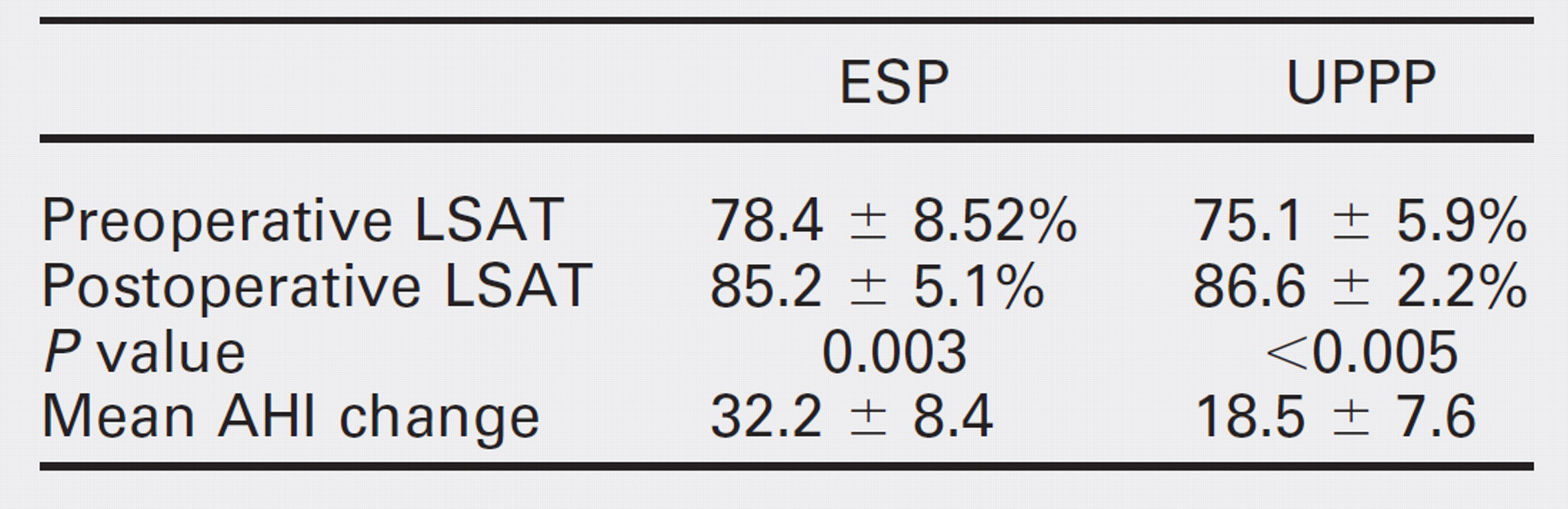
Forty-five patients were enrolled (22 UPPP, 23 ESP). Fortyone patients were men and four were women. The mean age was 42.1 years (range, 24-47 years), and the mean BMI was 28.7 kg/m 2 (range, 21.7-29.8 kg/m 2 ). The mean preoperative apnea-hypopnea index (AHI) for the entire group improved from 42.3 ± 17.1 to 19.2 ± 12.0, postoperatively with a mean follow-up of 6.5 months. The AHI improved from 44.2 ± 10.2 to 12.0 ± 6.6 (P < 0.005) (see Fig 1) following ESP and from 38.1 ± 6.46 to 19.6 ± 7.9 in the UPPP group (P < 0.005) (see Fig 2). Mean change was 32.2 ± 8.4 in the ESP group and 18.5 ± 7.6 in the UPPP group. Lowest oxygen saturation improved similarly from 78.4 ± 8.52% to 85.2 ± 5.1% in the ESP group (P = 0.003) and from 75.1 ± 5.9% to 86.6 ± 2.2% in the UPPP group (P < 0.005) (Table 1 and Table 2). Selecting an arbitrary threshold of a 50% reduction in AHI and AHI less than 20, success was 82.6% in ESP compared with 68.1% in UPPP (P < 0.05). Of great interest, when selecting an arbitrary threshold of a 50% reduction in AHI and AHI less than 15, the ESP success rate was 78.2%, compared with that of the UPPP group at only 45.5% (P < 0.005) (Table 3). Postoperative endoscopic findings also demonstrated significant reduction of lateral pharyngeal wall collapse in the ESP group, with most patients having only minimal lateral wall movements on Muller's maneuver, postoperatively. All patients in the ESP group had minimal lateral pharyngeal wall collapse noted on Muller's maneuver, with an average collapse grade of 1.4, not exceeding 50% collapse. This was not the case in the UPPP group, with some patients still having significant lateral pharyngeal wall collapse noted on Muller's maneuver, postoperatively.
Vicryl sutures used to hitch up the palatopharyngeus muscle to the soft palate muscles superolaterally.
There were no significant complications in either group. All patients started soft diet consumption on the first postoperative day. There was no significant difference in the use of narcotics or pain relief postoperatively in the two groups, and there was no long-term dysphagia or voice change.
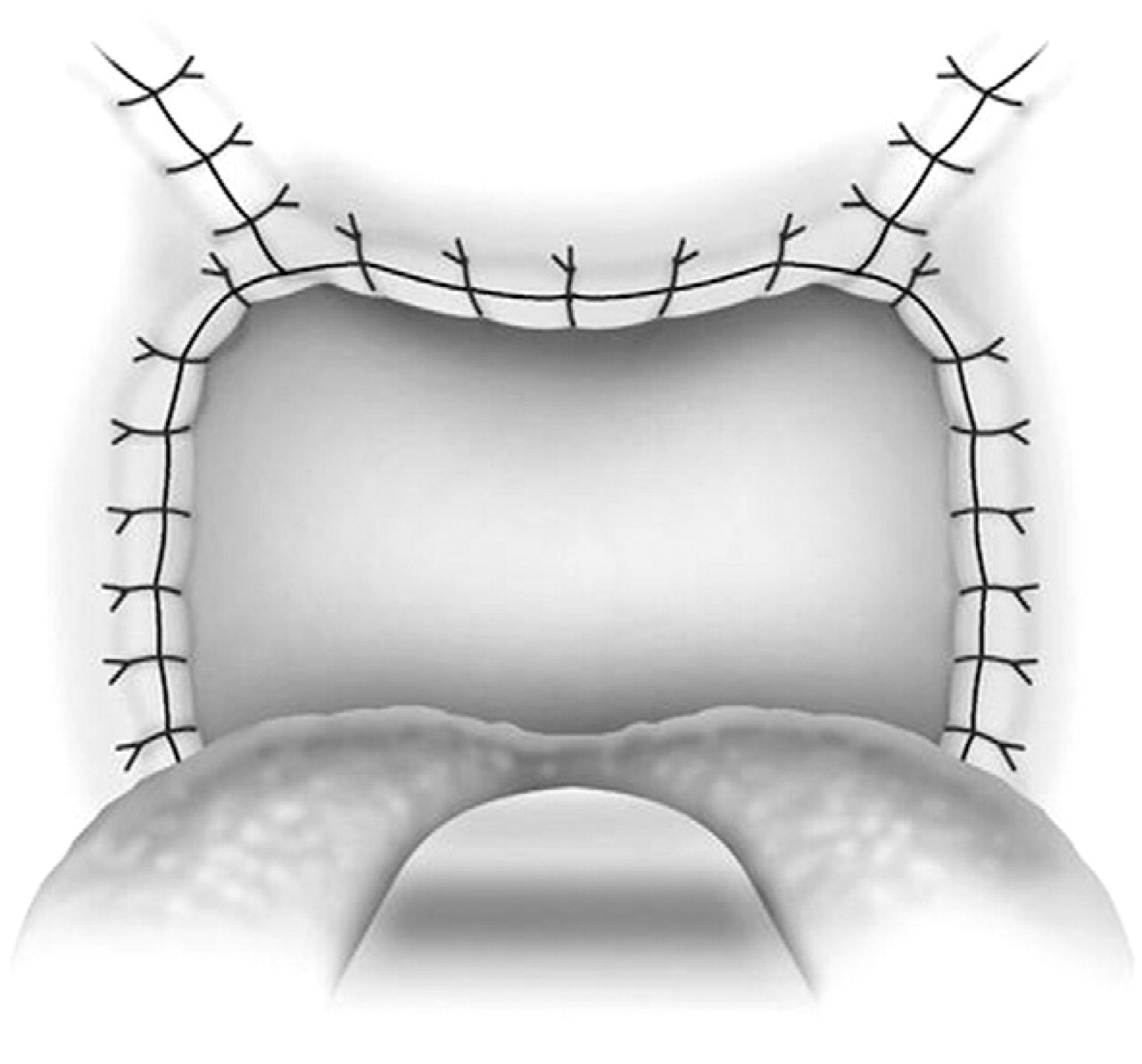
Closure of the palatal incisions.
Preoperative and postoperative AHI results of ESP and UPPP with success rate at AHI 50% reduction and <20
DISCUSSION
Cahali 1 described the lateral pharyngoplasty technique in 10 patients with moderate to severe OSA, who had mainly lateral pharyngeal wall collapse noted on clinical endoscopic examination. He showed very promising results in these 10 patients. 1 All 10 patients had improvements in their AHI, with a mean of 45.8, reducing to 15.2 (P = 0.009), postoperatively, with a mean follow-up of 8 months. Apnea index also improved with a reduction from a mean of 22.4 to 4.8 (P = 0.005). There were, however, significant swallowing problems in all 10 patients who underwent this procedure. All patients had dysphagia; this ranged from 8 days to 70 days, postoperatively (mean, 20.4 days). One patient had persistent velopharyngeal insufficiency for up to 6 weeks. Another patient had a permanent lost of taste to chocolate for 6 months. Cahali et al 9 compared this lateral pharyngoplasty technique with the traditional UPPP in 27 patients with OSA. All 15 patients who underwent the lateral pharyngoplasty achieved significant reduction in excessive daytime sleepiness, AHI, and AI. There were also improvements in the rapid eye movement sleep percentage and morning headaches in patients who had the lateral pharyngoplasty, compared with those who underwent the traditional UPPP. They concluded that patients who underwent the lateral pharyngoplasty technique had better clinical and polysomnographic results.
This new technique of ESP was conceived and modified from the Orticochea procedure and the lateral pharyngoplasty. The principle of this technique is to isolate the palatopharyngeus muscle (the main part of the lateral pharyngeal wall bulk) and rotate this muscle superoanterolaterally, to create the lateral wall tension and remove the bulk of the lateral pharyngeal walls. The key is to not completely isolate the muscle into a tube and rotate it; instead, part of its fibrous attachment to the superior pharyngeal constrictor muscle is maintained, so as to create the necessary tension and pull superoanterolaterally. A complete or partial uvulectomy is performed together with this procedure.
Preoperative and postoperative AHI results of ESP and UPPP with success rate at AHI 50% reduction and <15
AHI reduction 50% and <15
Preoperative and postoperative LSAT results of ESP and UPPP with mean change of AHI of each procedure
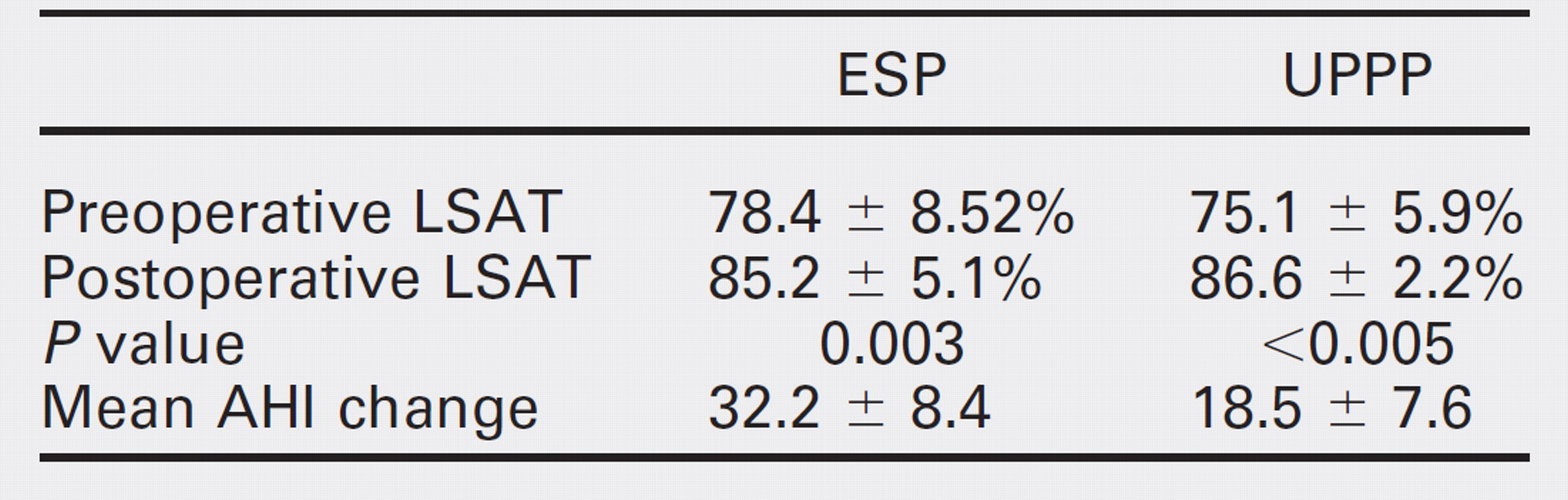
The AHI improved from 44.2 ± 10.2 to 12.0 ± 6.6 (P < 0.005) following ESP and from 38.1 ± 6.46 to 19.6 ± 7.9 in the UPPP group (P < 0.005). The data showed that the patients in the ESP group had more severe OSA compared to the UPPP group. Despite this difference, the mean change was 32.2 ± 8.4 in the ESP group and 18.5 ± 7.6 in the UPPP group. There were also similar impressive results in the lowest oxygen saturation, postoperatively.
The data from this small prospective randomized series of 45 patients suggest that the ESP may offer benefits over traditional methods of UPPP in a selected group of OSA patients with small tonsils, Friedman stage II or III, and lateral pharyngeal wall collapse noted on endoscopic examination. Patient selection is an important key to success for most surgical procedures, including this procedure.
CONCLUSION
The ESP is useful and effective in patients with small tonsils, Friedman stage II or III, and lateral pharyngeal wall collapse noted on endoscopic examination. This procedure is simple to perform, has promising results, is anatomically sound, and has minimal complications. 8
FINANCIAL DISCLOSURE
None.