
Abstract

Fibrin sealant (FS) has been successfully employed as a fixation method in skin transplantation, 4 and in the management of perianal fistula. 5 This study represents the first series of patients treated with FS for mucocutaneous fistulas after head and neck cancer surgery.
METHODS
We reviewed charts of 10 consecutive patients who developed mucocutaneous fistulas following surgical excision of head and neck tumors in our institution from May 2005 to May 2006 and were treated by using FS. The study was approved by the Johns Hopkins Medical Institutions Institutional Review Board.
Fibrin Sealant Application
For patients with fistulas managed during outpatient visits, the FS (Tisseel VH, two-component, vapor-heated fibrin sealant kit; Baxter Healthcare Corp, Westlake Village, CA) was applied in an examination room from two to six times separated by 1- to 3-week intervals. For inpatients, the FS was applied one to two times every 4 to 5 days at the bedside; then additional applications were continued at outpatient visits after discharge as necessary. The number and frequency of FS applications for each patient were tailored by the treating physician through evaluation of the closure rate of the fistula at each visit.
The fistulous track was suctioned with a flexible 21-gauge suction catheter; and one to two units of FS were prepared for injection. Either a blunt application with the needle supplied in the kit was used, or a flexible 21-gauge angiocatheter was connected to the double-syringe system. The tip was placed into the fistulous track until the apex of the fistula was reached, and FS was injected into the track while simultaneously with drawing the catheter until the glue was seen at the mucocutaneous junction. The flexible catheter was then removed, and the fibrin plug gelled instantaneously. The dose of FS injected was adjusted to fill the entire fistula track. For the patient with an orocutaneous fistula, a small amount of FS was injected intraorally at the floor of the mouth as well. No gauze packing was placed in conjunction with the FS plug, and any cover gauze dressing was separated by gel foam or ointment to avoid disruption of the FS-tissue adhesion. Outpatients were instructed to resume packing of the fistulas if salivary discharge recurred between treatments.
RESULTS
Patients included nine males and one female. Ages ranged from 51 to 81 years. Other clinical details are shown in Table 1.
Nine of the 10 fistulas demonstrated successful closure without further intervention during FS use, whereas 1 fistula persisted without substantial improvement despite several applications of FS. This patient had undergone preoperative radiotherapy, and his fistula was large (> 4 cm in diameter). After 4 weekly applications of FS, he underwent surgery (pectoralis major myocutaneous flap) for fistula closure. A small fistula persisted, after which he again received FS; this fistula healed within 35 days (case 10, Table 2). All patients tolerated FS application well: There was no bleeding, allergy, or other complications from its use.
In two cases (subjects 5 and 6, Table 2), the FS was used from the beginning of fistula management, whereas it was used after failure of other measures in most instances. Initial fistula management for eight patients included maintaining nothing-by-mouth status, as well as packing with frequent dressing changes and antibiotics applied for a range of 25 to 90 days (median 59 days). Surgery to repair the fistula was attempted prior to beginning FS in one patient, and three patients were sent for at least 20 hyperbaric oxygen dives. All patients were provided high-protein diet regimens via gastric tube. Also, all patients had serum proteins ranging between below normal to lower limit of normal, and were given high-protein diets. Five patients had hemoglobin levels of 7.5 to 9.5 gm/dL and received vitamins and iron supplementation; two patients had history of diabetes. The time until complete fistula healing after first FS use in the nine successfully treated patients ranged from 16 to 93 days (median 35 days). In two cases (1 and 4), all leakage of saliva stopped after the first FS application, and within 3 days the tract had substantially closed, admitting only a Calgi swab and requiring only one to two additional applications.
DISCUSSION
There was no clear correlation between risk profile and the effectiveness of FS. In addition, our limited experience does not provide any convincing evidence of synergism between FS and other adjuvant measures for fistula healing. We believe this issue warrants further investigation.
Patient characteristics
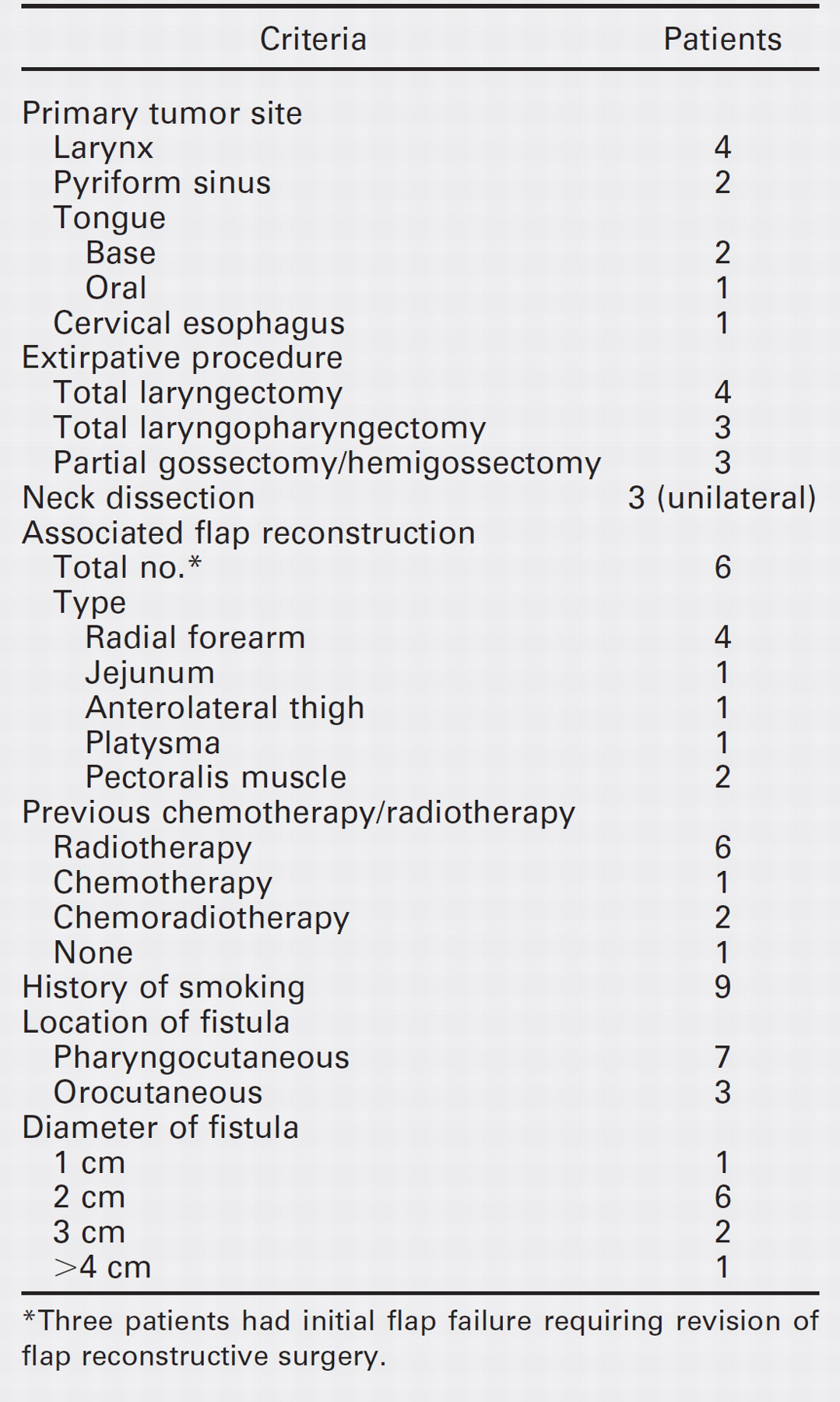
Three patients had initial flap failure requiring revision of flap reconstructive surgery.
Details of FS application
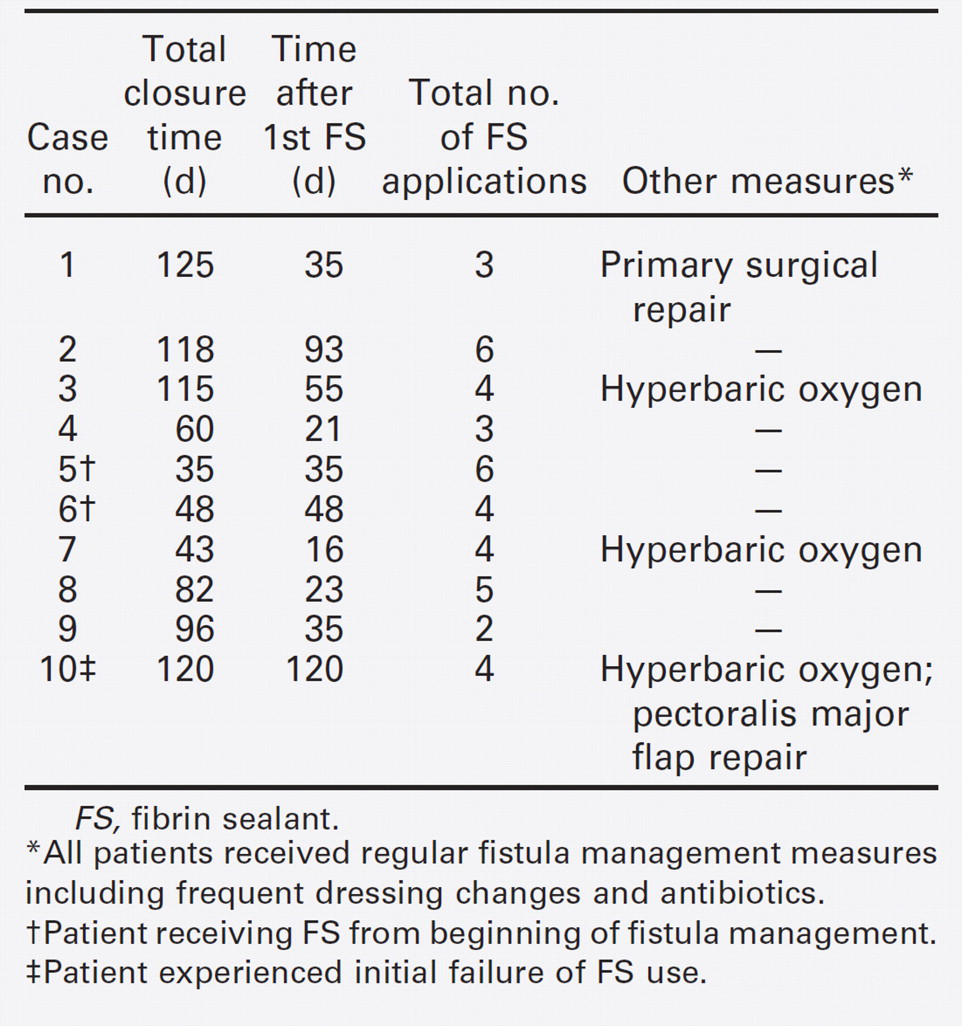
FS, fibrin sealant.
All patients received regular fistula management measures including frequent dressing changes and antibiotics.
Patient receiving FS from beginning of fistula management.
Patient experienced initial failure of FS use.
Our single failed attempt to manage a fistula with FS is instructive. This patient had had a previous total laryngectomy after failed primary radiation therapy. He developed a tongue base second primary 10 years later and underwent composite resection with pectoralis flap reconstruction. The flap failed and a wide fistula (4 cm) appeared with little thickness of surrounding soft tissue. We attempted FS application once a clean granulating wound bed was present. However, the FS plug had to be wide and thin (using up to four units) and was exposed to pooled saliva on one side and air on the other. After four applications there was no measurable reduction in fistula diameter, and a second pectoralis flap was placed. This flap was largely viable and when a smaller residual fistula appeared, it was readily sealed with FS. We believe that the use of FS in the absence of wound granulation and a tract of greater length than width is futile.
We believe that the use of FS in our study may decrease the need for dressing changes and home care nursing visits, and appeared to decrease total time needed for fistula healing.
CONCLUSION
FS may be useful as a conservative measure to enhance the healing of mucocutaneous fistulas following head and neck surgery. Further studies are recommended.
FINANCIAL DISCLOSURE
None.