
Abstract

DISCUSSION
Bifurcations and even trifurcations of the facial nerve have been previously reported. They may involve all or any portion of the nerve from the intracanalicular segment to the mastoid segment, and are most common in the tympanic segment. The previous report 1 of mesodermal tissue attached to the vertical facial nerve described 5 cases of mesodermal masses pedunculated off the vertical facial nerve. In our specimen, a pseudobranching occurs in the mastoid segment, with the posteromedial branch being confirmed as fibrous tissue on pathological examination. The ossicles, semicircular canals, cochlea, and internal auditory canal were all dissected and visualized, and found to have normal anatomy. In our specimen each of the vertical “nerves” had sufficient bulk to be mistaken for the entire nerve. Facial nerve stimulation might have been of assistance in a living patient.
This temporal bone specimen clearly displays the appearance of a vertical segment pseudobifurcation and demonstrates that the surgeon can never afford to be complacent in visually identifying the vertical nerve. The mastoid surgeon should retain this mental image for future work along the vertical segment of the facial nerve (Figure 1).
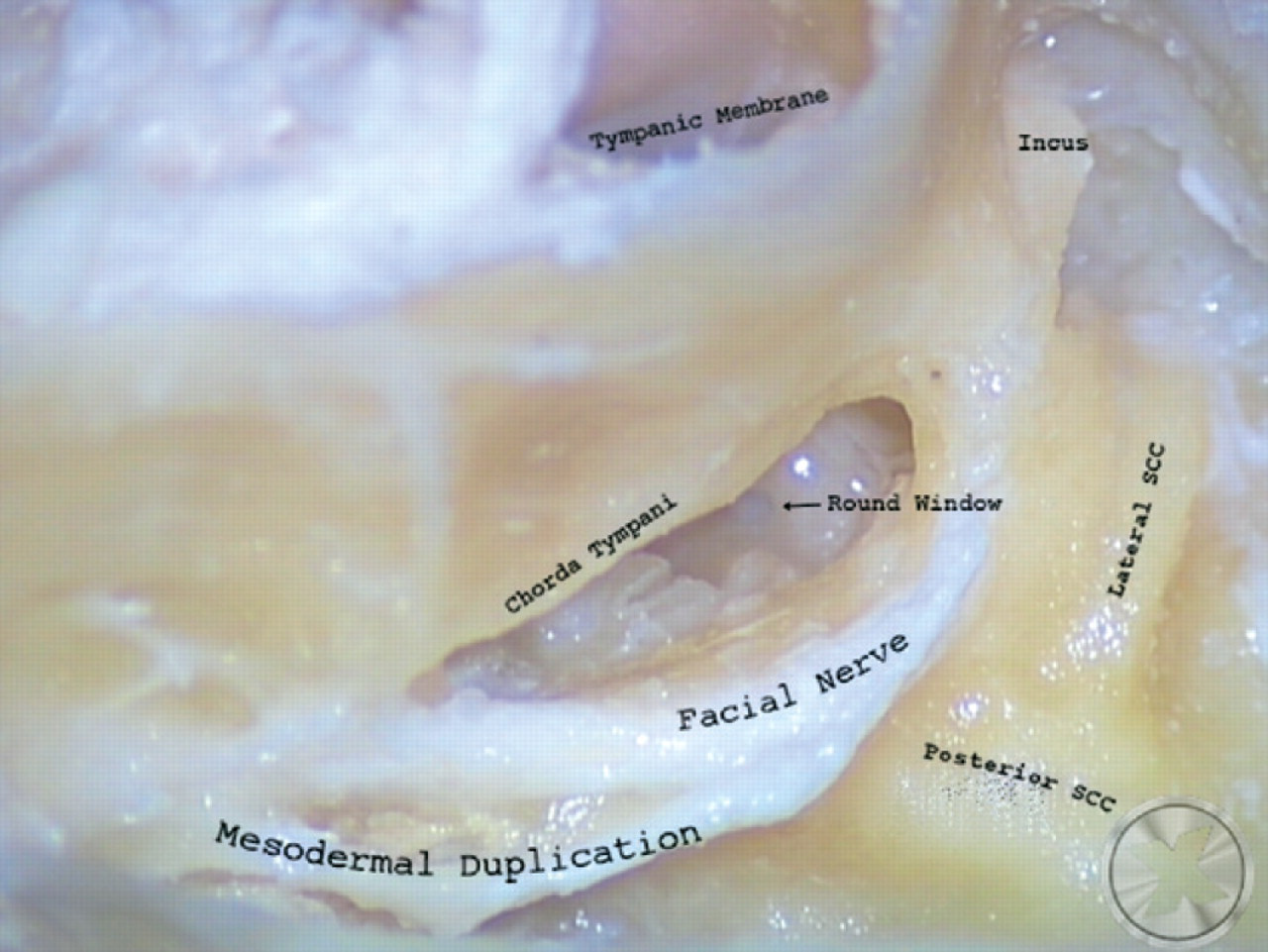
Temporal bone laboratory specimen: right ear. Visible are the lateral and posterior semicircular canals, facial recess, round window, chorda tympani, and tympanic membrane. The facial nerve appears to bifurcate directly after the second genu and to reunite near the take off of the chorda tympani. In fact, this posteromedial limb of tissue is fibrous tissue only and contains no neuronal elements.
AUTHOR INFORMATION
From the Section of Otolaryngology–Head and Neck Surgery (Drs Sigari, Mhoon, and Redleaf) and the Department of Pathology (Dr Montag), University of Chicago Medical Center.
Corresponding author: Farhad Sigari, MD, Aurora Medical Center, Suite 215, Kenosha, WI 53142.
E-mail address:
FINANCIAL DISCLOSURE
None.