
Abstract

A superficial parotidectomy with resection of the overlying skin was performed. At the time of surgery, the tumor appeared encapsulated at the level of the facial nerve (Fig 2). The frozen section was reported as benign. The facial nerve was preserved. The wound was closed with a large bilobed flap. The diagnosis on permanent section was acinic cell carcinoma of the parotid with clear margins of resection and without vascular or peri-neural invasion. The wound healed primarily. The patient refused further surgery and radiation therapy. She has since rejoined society.

Acinic cell carcinoma of parotid.
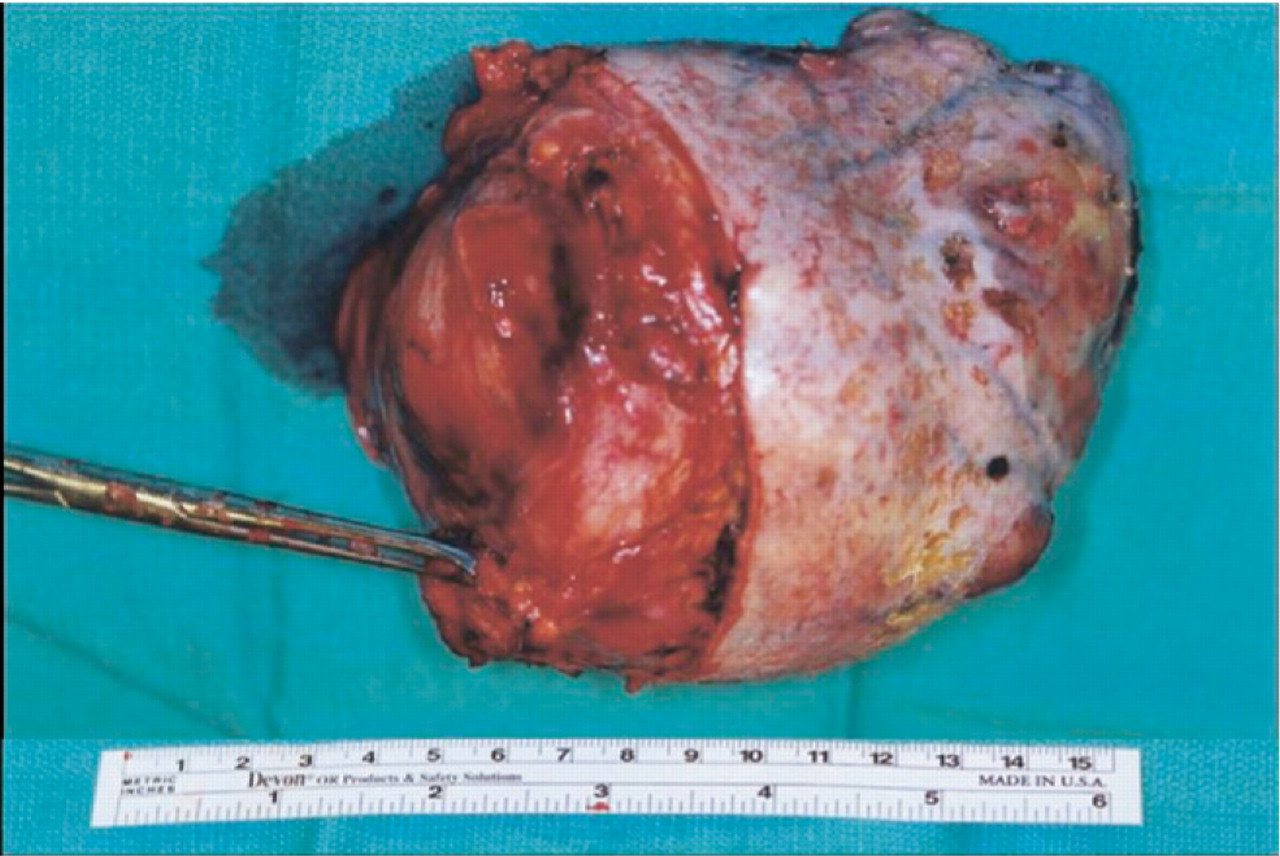
Surgical specimen encapsulated at deep margins of resection.
Discussion
Acinic cell carcinomas of the parotid gland are slow-growing malignancies. They are more common in women and are most frequent in the fifth and sixth decades of life. 1 They may occur in children and also may occur bilaterally. They comprise approximately 10% to 18% of malignant tumors and 2% to 4% of neoplasms of the parotid gland. As in the presented case, they may be present for years before treatment. After treatment, patients must be followed for years because the survival rate declines with increasing time. Enroth et al 2 in their series reported that the cure rate decreased from 89% at 5 years to 56% at 20 years. Spiro et al 3 in their series reported the survival rate to be 76% at 5 years, 63% at 10 years, and 55% at 15 years.
Grossly the tumor may have a capsule separating it from the facial nerve. It may be a multinodular mass with areas of cystic degeneration and hemorrhage or a mass with the same color and consistency as the normal gland. The microscopic appearance of the gland may vary greatly with the cells in a variety of architectural pat-terns. 4 The cells may be solid, papillary cystic, and follicular. Periodic acid–Schiff staining is usually positive.
The degree of differentiation is of no value in predicting the biological behavior of the tumor.
The treatment for acinic cell carcinoma is complete surgical removal by either superficial parotidectomy with facial nerve preservation or total parotidectomy if the nerve is involved. Because the tumor may metastasize to the cervical nodes, neck dissection is indicated for proven or suspected metastases. Distant metastases may occur with or without recurrent tumor in the parotid area or cervical node disease years after initial surgery. Adjunctive postoperative radiation therapy may also be used for clinically aggressive disease.
Author Contributions
Financial Disclosure
None.