
Abstract

Surgical resection has been the standard therapy for lymphatic malformations. Because of the infiltrative nature of these lesions and involvement of important anatomic structures, total extirpation is usually not possible. Additional treatment options have been investigated, with percutaneous sclerotherapy gaining favor. Several reports have shown promising results using the sclerosant OK-432 for macrocystic lymphatic malformations, with relatively few side effects.1–3 However, this agent has yet to gain Food and Drug Administration approval and is available in a research capacity only.
Doxycycline has been shown to be effective for benign lymphoepithelial cysts of the parotid gland,4 and Molitch et al5 showed improvement in five patients with lymphatic malformations in varying areas of the body. In the present article, we report our experience using doxycycline percutaneous sclerotherapy as the primary modality of treatment for pediatric head and neck macrocystic lymphatic malformations.
Materials and Methods
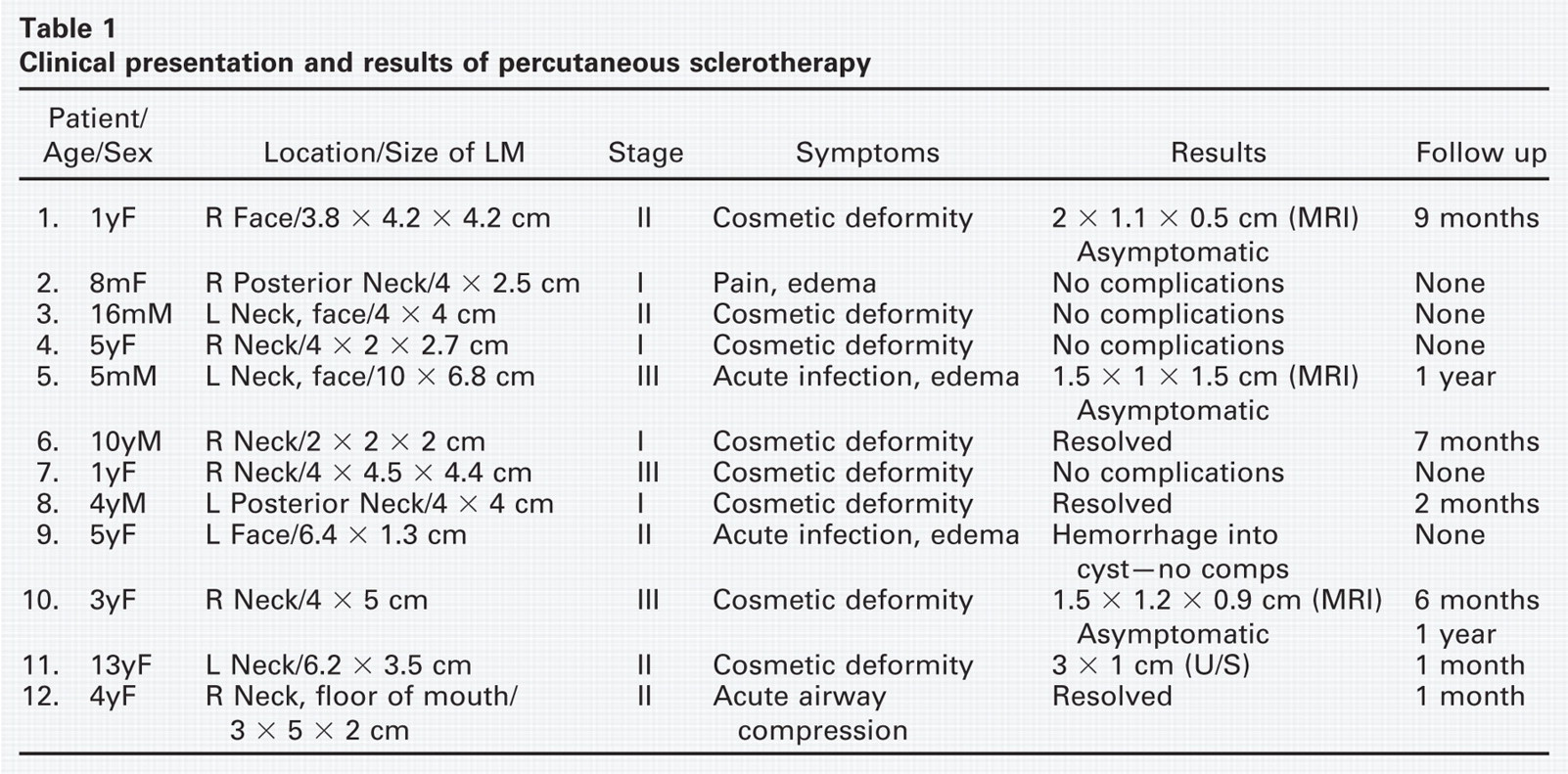
Twelve pediatric patients underwent ultrasound-guided percutaneous sclerotherapy of macrocystic head and/or neck lymphatic malformations with doxycycline as the sclero-sant. Internal review board approval was obtained for this retrospective chart review. Patient symptoms included asymptomatic neck swelling, pain, acute infection, and two instances of airway compromise. Patient presentations are summarized in Table 1. Workup of the patients included a comprehensive laboratory assessment, complete history and physical examination, and adequate imaging to appropriately delineate the lesion as a lymphatic malformation.
Clinical presentation and results of percutaneous sclerotherapy
Eight procedures were performed under intravenous sedation. Four procedures were performed under general anesthesia for the following reasons: one in conjunction with an adenoidectomy, two patients who had been previously intubated for airway stabilization, and the other for precaution in whom the lymphatic malformation was abutting the trachea. Patients were either discharged home the day of the procedure or kept for 23-hour observation.
The protocol for the procedures included a comprehensive discussion with the patient and/or family regarding the risks and benefits of the procedure as well as alternative treatments, and informed consent was obtained. All outpatient sclerotherapy procedures were performed in the interventional radiology suite. Intravenous sedation was induced with titrated doses of midazolam (0.1-0.3 mg/kg), fentanyl (1-3 μg/kg), and Nembutal (Ovation Pharmaceuticals, Deerfield, IL) (1-3 mg/kg). A scout ultrasound was performed to verify the exact location of the cavity. Patients were prepped and draped in standard surgical fashion. One percent lidocaine local anesthesia was infiltrated subcutaneously, and a 20-gauge Jelco (Medex, Ltd, Ros-sendale, UK) intravenous catheter was introduced into the cystic cavity under direct ultrasound guidance. Fluid was then aspirated from the cavity until drainage was complete. If multiple cysts were found on preoperative imaging, then a water-soluble contrast (Omniray 240; Mallinckrodt Inc., Hazlewood, MO) was injected and subsequently aspirated under ultrasound to further delineate connections among the cystic cavities and the adequacy of the drainage (Fig 1).
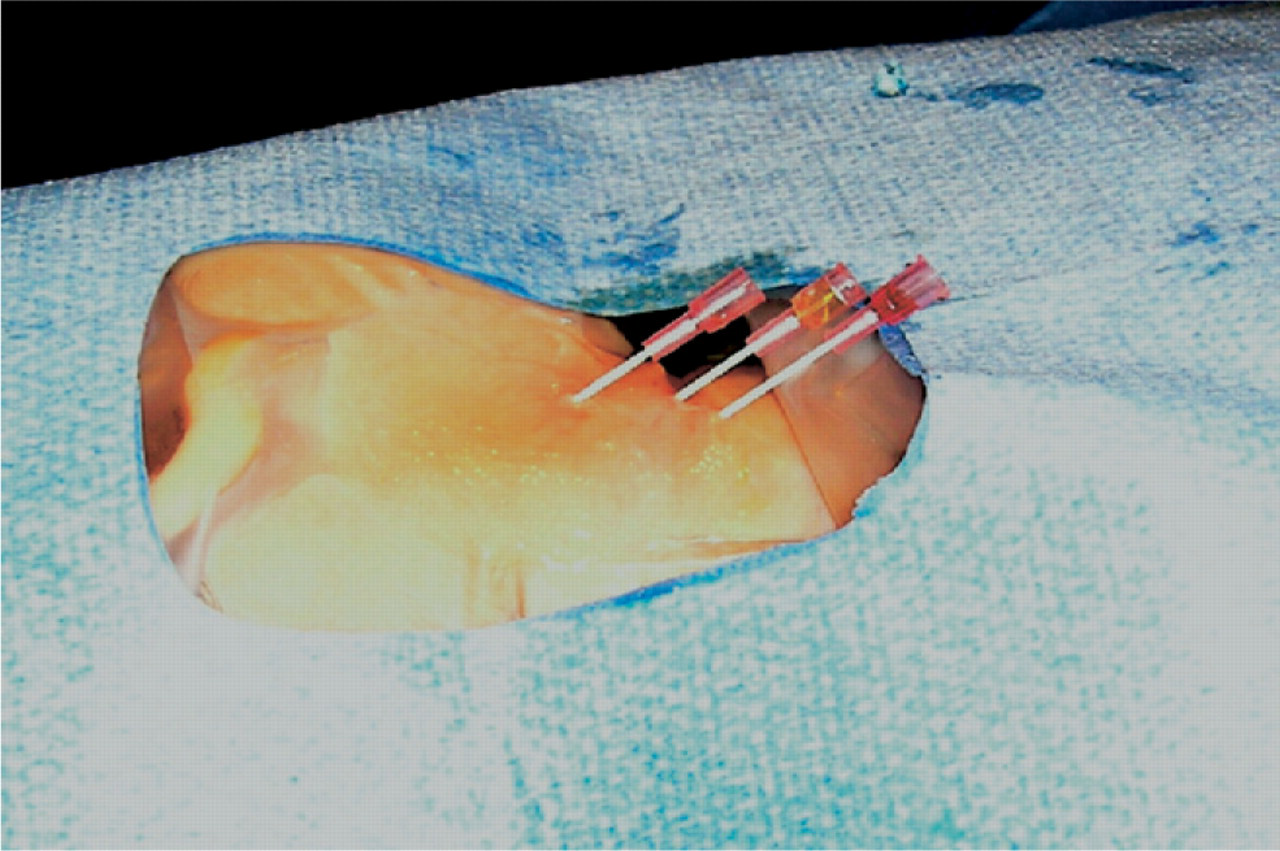
A patient with neck lymphatic malformation prepped and draped for sclerotherapy. Three 20-gauge Gelco catheters have been placed into each individual cyst within the lymphatic malformation and will be drained until the cyst is decompressed.
Doxycycline was diluted in normal saline solution to a concentration of 10 mg/mL. The solution was then infused into the cavity in a 1:1 ratio of the fluid removed or until the cavity was shown on ultrasound to be filled with sclerosant. Ultrasound was used to confirm the reinjection. In the cases of multiple separate cystic cavities found on contrast injection, the procedure was repeated for each cyst. The catheter was then removed, and a sterile dressing was applied to the area. A Cook Dawson Mueller catheter (Cook Medical, Bloomington, IL) was left to passively drain hemorrhage into or excess edema around the cavity in three patients who had a compromised airway as a result of the anatomic location of the lymphatic malformation. Minimal drainage ensued, leaving the majority of the sclerosant within the cavities. These catheters were removed when the lesions had proven stable. There were no immediate complications of the procedures.
Results
All seven patients who have had appropriate follow-up have had either a complete resolution of the lymphatic malformation or a marked reduction in the size of the lesion. Follow-up is limited but ongoing for these patients and ranges from one month to one year after treatment. Patients seen in follow-up with negative physical examination findings were not categorically reimaged, although four patients did have postprocedural imaging to document the radio-graphic response to the treatment. The cosmetic deformities and all symptoms of pain, drainage, or infection have resolved. Five patients have been lost to follow-up, with unsuccessful attempts to arrange posttreatment clinic visits.
There were no immediate complications of the sclero-therapy procedures. Pain, fevers, chills, or other constitutional symptoms were not reported. However, one patient returned three weeks after the procedure with hemorrhage into the cystic cavity. The decision was made to treat the complication conservatively, and the swelling later resolved.
Discussion
Doxycycline was used in the present study as an alternative to OK-432. The exact mechanism of action of doxycycline as a sclerosant is unknown, but, similar to OK-432, an inflammatory reaction results in the fibrosis and eventual involution of endothelial-lined cavities. The injectable form of doxycycline is readily available from pharmacies with compounding capability and requires reconstitution in a normal saline solution at a concentration of 10 mg/mL. It is inexpensive and is comparable to the oral form of the antibiotic, costing $20 for a standard 10-day course. Potential risks involved with percutaneous sclerotherapy include the development of constitutional symptoms as well as pain, local erythema, and surrounding edema at the injection site.2
We are encouraged by our preliminary experience with doxycycline sclerotherapy for head and neck macrocystic lymphatic malformations. We plan to continue to use this modality of treatment in the primary management of selected lesions as an alternative to surgery or OK-432.