
Abstract

The capsule endoscope has revolutionized small-bowel inspection, which before was limited to indirect studies, such as barium radiography, scintigraphy, and angiog-raphy, or to direct but invasive push enteroscopy. It provides a direct, yet minimally invasive, visualization of the small bowel. Capsule endoscopy is approved by the FDA for detection of small-bowel mucosal abnormalities. To date its major application has been evaluation of occult gastrointestinal (GI) bleeding. The device has been used in 340,000 patients worldwide, with 105,000 procedures in the US within the last year. As its applications increase to include evaluation of conditions such as Crohn's disease, small-bowel polyps, and abnormal small-bowel radio-graphic studies, its utilization will increase (sales increased by 18% over the last year), and clinicians should be aware of its complications. Three cases of capsule endoscope aspiration have been reported in gastroenterology literature to date. This is the first report in otolaryngology literature. Although rare, this complication is potentially fatal and should be considered an emergency.
A 67-year-old man with history of anemia was referred for capsule endoscopy to evaluate for occult GI hemorrhage. Due to a past medical history of hypertension, diabetes mellitus, cerebrovascular accident, and intermittent dyspha-gia, endoscopic placement of a capsule endoscope (M2A, Given Imaging, Ltd, Duluth, GA) was recommended. However, the patient declined and chose to swallow the capsule, immediately after which he began to cough and exhibit dysphonia, which resolved. There was no respiratory distress, but he developed a persistent cough. Within 3 minutes the patient became tachypneic and tachycardic, but his oxygen saturation remained above 95%. There were ronchi, but no stridor. The physician recognized the possibility of interrogating the capsule endoscope to determine its location. Images from the capsule endoscope were downloaded and analyzed within 5 minutes and definitively revealed that the device was aspirated promptly after it was swallowed (Fig 1). This process took less time than obtaining plain radiographs.

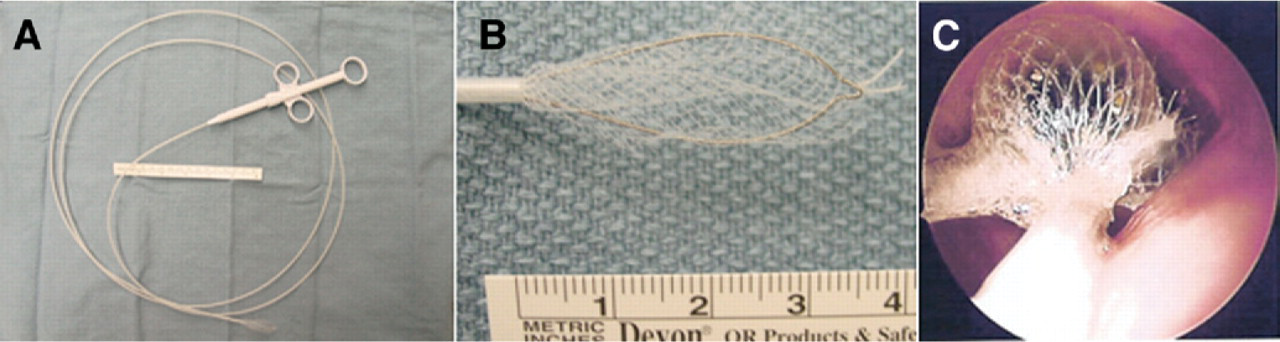
Images from capsule endoscope. (
The patient was taken to the operating room for retrieval of the capsule. He was intubated and ventilated using a rigid bronchoscope. A Hopkins rod endoscope was used to inspect the tracheobronchial tree, and the capsule was found in the left main bronchus. An expandable basket foreign body retriever (Roth Net, US Endoscopy, Mentor, OH) (Fig 2) was passed through the rigid bronchoscope to retrieve the capsule. The surgeon advanced the Roth Net device into the airway, deployed the basket, and manipulated it to capture the foreign body, while manipulating the bronchoscope to maintain visualization of the capsule throughout the procedure. The bronchoscope and the Roth Net device containing the capsule endoscope were withdrawn together. The patient was taken to the post-anesthesia care unit in stable condition and recovered uneventfully.
Discussion
To date there have been three reports of capsule endoscope aspiration. In two, the patient was able to cough up the capsule.1,2 In the third, the capsule had to be retrieved at emergent rigid bronchoscopy using a grasper forceps in conjunction with an expandable endoscopic basket.3 Advanced age, poor general condition with dehydration or myopathy, dysphagia, poor dentition, alcohol or drug use, and underlying neurologic disease are risk factors for aspiration and indications for endoscopic placement of the capsule.
We herein report the first case of aspiration of a capsule endoscope in otolaryngology literature. Coughing or the sensation of the capsule being “stuck in the throat” or any persistent symptom localizing to the larynx, pharynx, or esophagus suggest possible aspiration. If there is any possibility of aspiration, diagnostic investigations should be undertaken, because any delay in diagnosis could lead to airway compromise. Routine radiographic diagnostic techniques such as plain chest and abdomen radiographs or CT chest have been suggested, but they are time consuming and can be dangerous if an unstable patient has to be transported to the radiology suite. We propose downloading video from the capsule endoscope as a novel, more rapid (taking less than 5 minutes), and direct (photographs instead of radiographs) method of localizing its position. Once confirmed, the controlled environment of the operating room is the optimal setting for retrieval of an aspirated capsule endo-scope. The capsule endoscope is approximately cylindrical in shape, 2.5 cm in length, and 1 cm in cross-sectional diameter. Its relatively large size and smooth surface precludes removal with routine graspers and conventional forceps. The Roth Net foreign body retriever was very useful in this setting and allowed the capsule endoscope to be removed quickly and with minimal trauma.