
Abstract
Annual cost of medication to treat AR in the United States was estimated to be $3.1 billion in 1997, with 77% spent on prescription pharmaceutical products. 9 More recent direct medical cost estimates are as high as $4.5 billion. 2,3 Allergic rhinitis is also responsible for 3.8 million days lost yearly from school and work in the United States. 3,4,8 When indirect costs are included, the economic impact of AR may be as high as $7.9 billion. 2,3
Along with the classic triad of nasal obstruction, rhinorrhea, and sneezing, 10 patients with AR often report nonnasal symptoms that involve the ears, eyes, and throat, including cough. 11,12 Allergic eye symptoms such as itching, redness, and tearing, also referred to as allergic conjunctivitis (AC), are extremely common in patients with AR. 1,3,5 Coexistent nasal and ocular allergy symptoms are often termed rhino-conjunctivitis. Because nasal and ocular symptoms are so interwoven in AR, precise estimates of the economic impact of ocular symptoms are difficult to obtain. Current data clearly indicate, however, that ocular allergy symptoms diminish patients' quality of life and represent a considerable socioeconomic burden. 13
Intranasal corticosteroids (INSs) have proven efficacy in relieving nasal and nonnasal symptoms of AR. In particular, clinical evidence increasingly supports their efficacy in reducing the symptoms of rhinoconjunctivitis. 10,14,15 The purpose of this article is to provide a better understanding of the pathogenesis of ocular symptoms associated with AR and to examine the evidence for the use of INSs in the management of these burdensome symptoms.
CLASSIFICATIONS OF ALLERGIC CONJUNCTIVITIS
Allergic conjunctivitis encompasses several ocular allergic diseases of varying severity. Vernal and atopic keratoconjunctivitis are more serious diseases that can lead to blindness (patients with this condition do not present with nasal symptoms, and thus are not the subject of this review). 1 Seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC) often coexist with the nasal symptoms of seasonal allergic rhinitis (SAR) and perennial allergic rhinitis (PAR).
Perennial AR and SAR are the 2 most common types of AR; PAR is found in 10% to 20% of the population and SAR in about 10% of the population. 16 These classifications are not mutually exclusive, as some cases involve a combination of conditions, such as PAR with seasonal exacerbation. It has been estimated that approximately 40% of AR patients have both seasonal and perennial symptoms. 16
Seasonal allergic conjunctivitis is the most common form of AC and accounts for 25% to 50% of ocular allergy cases, usually classified as mild to moderate. 17 Seasonal release of airborne pollen allergens from trees, grasses, or weeds triggers the typical ocular symptoms that usually affect both eyes simultaneously. The associated ocular discharge is usually scant or watery, and the cornea is rarely involved. 18,19
Perennial allergic conjunctivitis frequently results from chronic exposure to indoor and occupational allergens. 20 Symptoms are milder and less prevalent than those associated with SAC, 21 but they may persist for more than 9 months annually. 16 As with AR, there is frequent overlap between patients with SAC and PAC. For example, up to 87% of patients with PAC report seasonal exacerbations, particularly in the autumn, when exposure to dust mites and fungal allergens is highest. 17
EPIDEMIOLOGY OF OCULAR SYMPTOMS
Symptoms associated with AC are commonly seen in a number of allergic conditions including AR, asthma, and food allergies. 12 Of 898 new patients referred to an allergy clinic in Italy, 363 (40%) had symptoms consistent with AC, and 66% of these were diagnosed with SAR. Allergic rhinitis was the most common concurrent allergic condition in these patients. 21,22 In a study 23 of Japanese patients with pollinosis, concurrent AC was seen in approximately 90% of cases.
Isolated AC is relatively uncommon. Among newly diagnosed hay fever patients, 85% were diagnosed with rhinoconjunctivitis, whereas conjunctivitis alone or rhinitis alone was diagnosed in only 8% and 7%, respectively. 24 An opposite pattern was noted when patients were grouped by symptom severity: severe symptoms were experienced by 31% of patients with rhinitis alone compared with 22% of those with conjunctivitis alone and 9% of those with rhinoconjunctivitis. Moderate symptoms were experienced similarly by all 3 groups (51% to 54%). The authors concluded that conjunctivitis symptoms are at least as severe as rhinitis symptoms for approximately 70% of SAR patients. 24
The prevalence of ocular symptoms also depends on the sample population. A survey of 2500 United States symptomatic and/or treated AR patients found that 40% of responders complained of frequent watery eyes during allergy season. 25 The majority of these responders reported that red/itching eyes and watery eyes were extremely or moderately bothersome and 15% stated that their most bothersome symptoms were ocular in nature. 25 In a survey of untreated Swiss subjects with seasonal rhinoconjunctivitis, 75% had ocular symptoms that were moderate or severe. 24 The primary complaints were rhinoconjunctivitis (53%), AC (22%), and rhinitis (25%). This study also found that patients with isolated conjunctivitis were less likely to experience concurrent asthma (10%) than were patients with rhinoconjunctivitis or isolated rhinitis (32%, 35%, respectively). Age also seems to affect the prevalence of AC. In the above Swiss study, a bimodal pattern was observed with peaks at 15 years and 35 to 40 years. 24
PATHOPHYSIOLOGY OF ARASSOCIATED OCULAR SYMPTOMS
Early and Late Phase Responses
SAC and PAC can follow typical mast cell-mediated hypersensitivity reactions in which direct allergen exposure cross links receptor-bound IgE on conjunctival mast cells, leading to acute mast cell degranulation and release of preformed mediators (such as histamine) and newly formed mediators such as leukotrienes. 17,21 Preformed mediators, primarily histamine, cause neuronal stimulation, conjunctival vasodilatation, increased vascular permeability and thus the itching, redness, swelling, and lacrimation associated with the early phase response (EPR). 17,19,26 Signs and symptoms of EPR start within 1 to 15 minutes after allergen challenge and peak approximately 15 to 20 minutes post-challenge. 27–29 Maximal tear levels of the inflammatory mediators histamine and tryptase are seen 20 minutes post-challenge and return to prechallenge levels by 40 minutes. 28
Although the ocular symptoms of SAC and PAC often quickly resolve once the offending allergen is removed, signs and symptoms of ocular inflammation may persist in some patients. Symptoms of this late phase response (LPR) include redness, itching, tearing, discomfort, and the sensation of a foreign body in the eye. 21,28 The classic model of LPR is a recurrence of signs and symptoms of ocular inflammation beginning 4 to 8 hours after the acute reaction. 28 In the real world, however, the time course and pattern of symptoms in the LPR is highly variable, and ranges from continuous symptoms from provocation through the LPR to intermittent symptoms to the classical response.
The recrudescence of symptoms hours after the initial provocation coincides with a second peak in mediators in tear samples, such as histamine and eosinophilic cationic protein, along with increased numbers of inflammatory cells in the conjunctiva and tear samples. 28,30 In tear samples, early increases in neutrophils are followed by increases in eosinophils, lymphocytes, and monocytes 6 to 24 hours after the initial challenge. 21
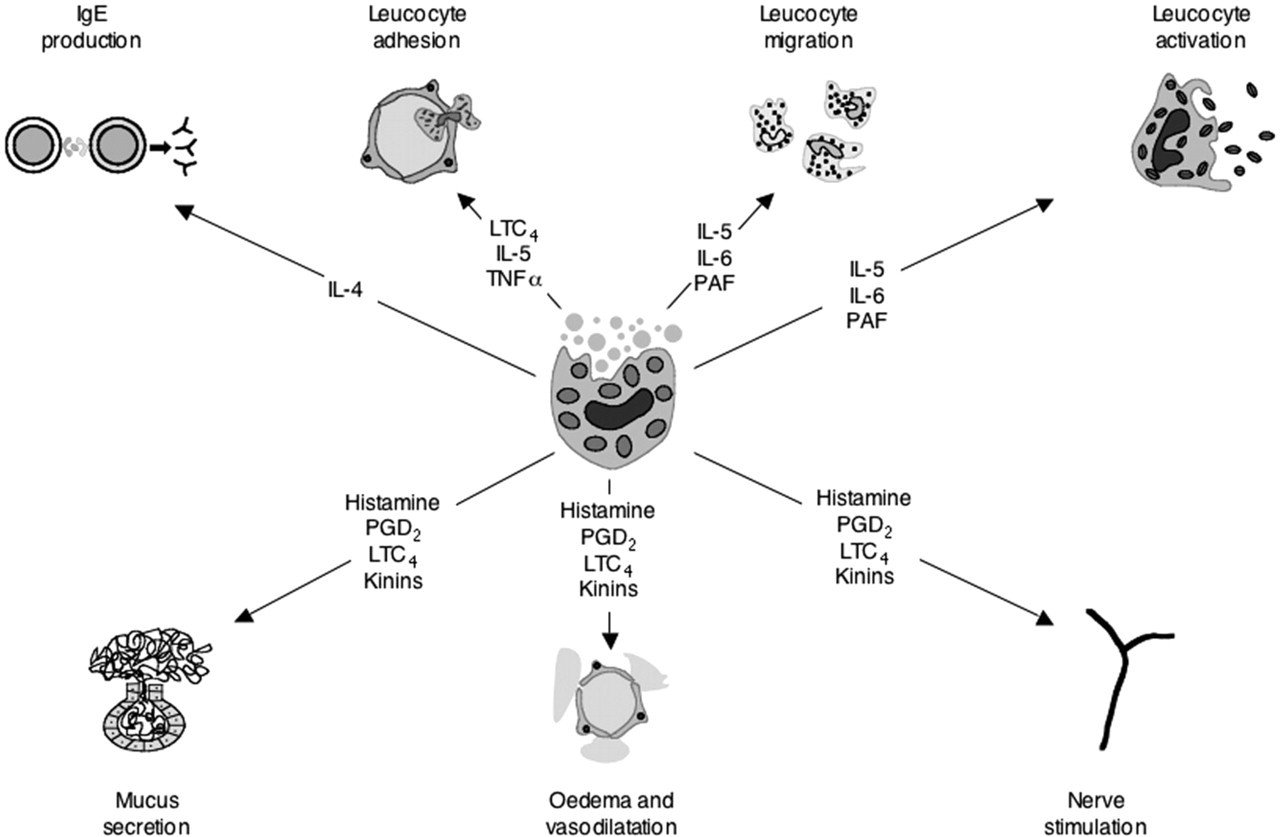
Profile of products released from activated mast cells and their suggested mechanism(s) of action. (PGD2, prostaglandin; LTC4, leukotriene; PAF, platelet activating factor.) (Reprinted with permission from McGill 1998. 17 )
Infiltration of inflammatory cells into the conjunctival epithelium and tear samples is likely due to a cascade of events initiated by mast cell-derived mediators released during the EPR. 31 Histamine, leukotrienes, and chemotactic cytokines found in mast cells and epithelial cells, such as IL-4, IL-5, IL-6, and TNF-alpha, promote migration of eosinophils, lymphocytes, and neutrophils, which then infiltrate the conjunctival surface through dilated capillaries (Fig 1). 31,32 Expression of ICAM-1 on conjunctival epithelial cells, which is essential to eosinophil adhesion, is also upregulated after conjunctival allergen provocation. 31
Nasal allergen challenge in AR patients leads to activation of circulating basophils, as evidenced by increased secretion of IL-13 and increased expression of FceRIb (b chain of the high-affinity receptor for IgE). 33 These priming effects may augment the LPR in AC. 35 Studies have also shown that in AR patients, nasal allergen provocation results in increased numbers of eosinophils and basophils and their progenitor cells in bone marrow and blood. 34,35 A model of cell trafficking has been proposed in which progenitor inflammatory cells migrate into the target tissues where they differentiate into mature inflammatory cells. 34 Therefore, the enlarged pool of mature and progenitor inflammatory cells, which is observed in AR, may allow for more rapid and intense infiltration of inflammatory cells into the conjunctiva after direct conjunctival allergen provocation.
In SAC and PAC, development of the LPR varies by patient. 27 However, severity of the EPR is likely linked to development of the LPR. 19 When patients with SAC were provoked with a low dose of topical allergen, clinical symptoms and local cytologic changes were noted only at the 20-minute assessment. As the dose was increased, the duration of the inflammatory response also increased (up to 1 hour in the higher antigen concentrations and up to 6 hours in the highest dose group, respectively). 27 This suggests that the clinical and cytologic changes associated with a conjunctival LPR are a continuous process, in which low-dose provocation leads to a self-limiting EPR, whereas at higher doses or in subjects with higher allergen sensitivity, a more intense and prolonged cell recruitment is induced, followed by a LPR. 27
Some authors have suggested that the LPR is the bridge between the self-limiting inflammation of the EPR and the long-term structural changes seen in chronic inflammatory disease. 28 Mast cells, which are typically not seen in conjunctival samples from nonatopic subjects, are a common feature of SAC. 36,37 Data regarding the upregulation of eosinophils and neutrophils are less consistent. In 2 studies that assessed conjunctival inflammatory cells in SAC patients or controls during allergy season, 1 study found higher numbers of eosinophils and neutrophils in SAC patients, 30 and the other study found no significant differences between these 2 groups. 37 These differences may reflect variability in the progression of the ocular allergic response from early to late to chronic inflammation.
Neural Reflex Pathways
Direct allergen contact with the conjunctiva undoubtedly contributes to the mechanism underlying allergic ocular symptoms in SAC and PAC. However, ocular symptoms can occur without evidence of direct conjunctival exposure to allergen. Lebel et al 38 found that ocular symptoms were reported by approximately 20% of SAR patients in whom allergen provocation was isolated to the nasal mucosa. In a more recent study by Baroody et al, 39 unilateral nasal provocation with ragweed or grass pollen resulted in ocular symptoms (itching and watery eyes) and increased ocular secretions bilaterally in SAR patients. Histamine and albumin in ocular secretions were not elevated, which indicates an absence of mast cell degranulation in the eye. In nasal secretions, biologic markers associated with an allergic response (histamine and albumin) were noted only on the side that was challenged, whereas the weight of nasal secretions increased bilaterally. Because no nerves are known to communicate from one side of the nose to the other, 40 the response on the unprovoked nostril is likely due to a centrally mediated nasonasal reflex, traveling afferently via the second branch of the trigeminal nerve and efferently by the parasympathetic nerves to glands and vessels in the conjunctiva and nasal mucosa. Pretreatment with azelastine at the site of provocation abolished both the ocular symptoms and the contralateral nasal symptoms, which suggests that histamine produced at the site of provocation initiates the reflex.
The nasal ocular reflex is described as chemical and mechanical stimulation of the nasal mucosa leading to lacrimation. 41 Philip et al 40 found that nasal application of capsaicin produced lacrimation within 10 seconds. Furthermore, nasal and ocular responses diminished with repeated capsaicin application, which supports the concept of a nasal ocular reflex pathway.
Allergic inflammation alters neuronal function at multiple levels, including primary afferent sensory nerves, autonomic ganglia, and integrative centers of the central nervous system, in ways that may provoke or exacerbate allergic symptomatology. 42 In vitro animal and human studies have shown that allergic mediators stimulate neural pathways through direct and indirect mechanisms. Although the direct mechanisms underlying allergen-induced changes in neural reflexes have not been completely elucidated, histamine in isolated animal nerve models increases the depolarization sensitivity to mechanical stimuli in afferent nerves, thus enhancing neural excitability and nerve discharge. 42 Because afferent nerves are involved in the sensation of itching, hyperresponsiveness of these nerves may enhance the perception of ocular allergic symptoms. 42 Allergic inflammation also increases sensitivity to neuroactive compounds involved in reflex pathways. Riccio et al 43 found that sensitivity to intranasal provocation with bradykinin, which induces symptoms of AR such as sneezing and rhinorrhea, is greater in PAR and in-season SAR patients than in nonatopic or out-of-season SAR patients. 43 In symptomatic patients, unilateral provocation with bradykinin increased nasal secretion (rhinorrhea) on the ipsilateral and contralateral side, whereas no effect on the nasal mucosa was seen in asymptomatic patients. Furthermore, this effect was blocked by atropine, 43 supporting the conclusion that the allergic reaction enhances neural responsiveness and may increase reflexive neuronal activity important to the development of ocular allergic symptoms. 42
Blockage of nasolacrimal ducts has also been proposed as a cause of AR-associated lacrimation. A study by Sanke et al 44 proposed that nasal inflammation leads to mechanical obstruction of the nasolacrimal duct and epiphora. However, subsequent research 45 has shown that blockage of the lacrimal drainage apparatus does not worsen eye symptoms in response to an ocular antigen challenge. In addition, lacrimal duct patency, demonstrated by a positive Jones test, was maintained in patients with clear symptoms of nasal and ocular allergy following nasal and ocular allergen provocation. 46
QUALITY OF LIFE AND ECONOMIC COSTS ASSOCIATED WITH ALLERGIC CONJUNCTIVITIS
Although allergic eye symptoms are often deemed by health care providers to be trivial in comparison with those relating to other diseases, their impact on patient quality of life and health care costs is substantial. The impact of ocular symptoms on daily activities, emotions, and satisfaction with treatment was assessed in an ophthalmology clinic setting using the Eye Allergy Patient Impact Questionnaire (EAPIQ). Of the 132 subjects with allergic eye symptoms, 17% were unable to perform tasks any day when they had symptoms. Dry eyes and itchy/burning eyes were the most frequent symptoms, and fatigue and difficulty being outdoors were the main quality-of-life complaints. 47 A study of 88 German patients with seasonal eye allergy symptoms in the ophthalmology clinic setting found that itchy/burning eyes was the most frequently reported symptom (89%), followed by swollen/puffy eyes (68%). These patients also reported significant fatigue and difficulty being outdoors, as well as difficulty reading. 48
The economic impact of SAC has been assessed in private, specialist clinic patients and public, primary care clinic patients. In a primary care clinic study 49 in Oxfordshire, England, patients who presented with symptoms of SAC had lower weekly earnings, worked fewer hours, experienced a greater degree of pain and discomfort, and had a lower perception of health compared with controls, as determined by individual responses to multiple health and quality-of-life questionnaires. Estimated total annual costs of SAC ranged from £64 to £124 per patient. In a private tertiary care setting, Spanish patients with SAC also had lower quality-of-life scores than controls, in terms of self-perceived overall health, overall vision, distance vision, ocular pain, mental health issues, role limitations, and dependency. Twenty percent reported taking time off from work, and total mean annual costs per SAC sufferer were estimated at €348. 12 The differences in estimated costs between the 2 studies were primarily felt to reflect the greater willingness to pay for treatment in the private, self-pay Spanish population. 12
EMERGING ROLE OF INTRANASAL CORTICOSTEROIDS FOR MANAGEMENT OF OCULAR SYMPTOMS
Allergic rhinitis symptoms are treated with a variety of topical and systemic pharmaceutical products, both prescription and over the counter. Intranasal corticosteroids and antihistamines are the most commonly prescribed classes of medications. 50
Intranasal corticosteroids have a well-established clinical record for superior efficacy and safety in the treatment of nasal congestion and other nasal symptoms of AR. More recent data also support the use of INSs to treat ocular symptoms associated with AR. The potential for an expanding role for INSs in the comprehensive management of AR has been acknowledged in expert guidelines, including the 2006 ARIA update and the 2006 International Primary Care Respiratory Group Guidelines. 10,51 These reports noted the beneficial anti-inflammatory effects of INSs throughout the respiratory system, as well as the positive effects on ocular symptoms.
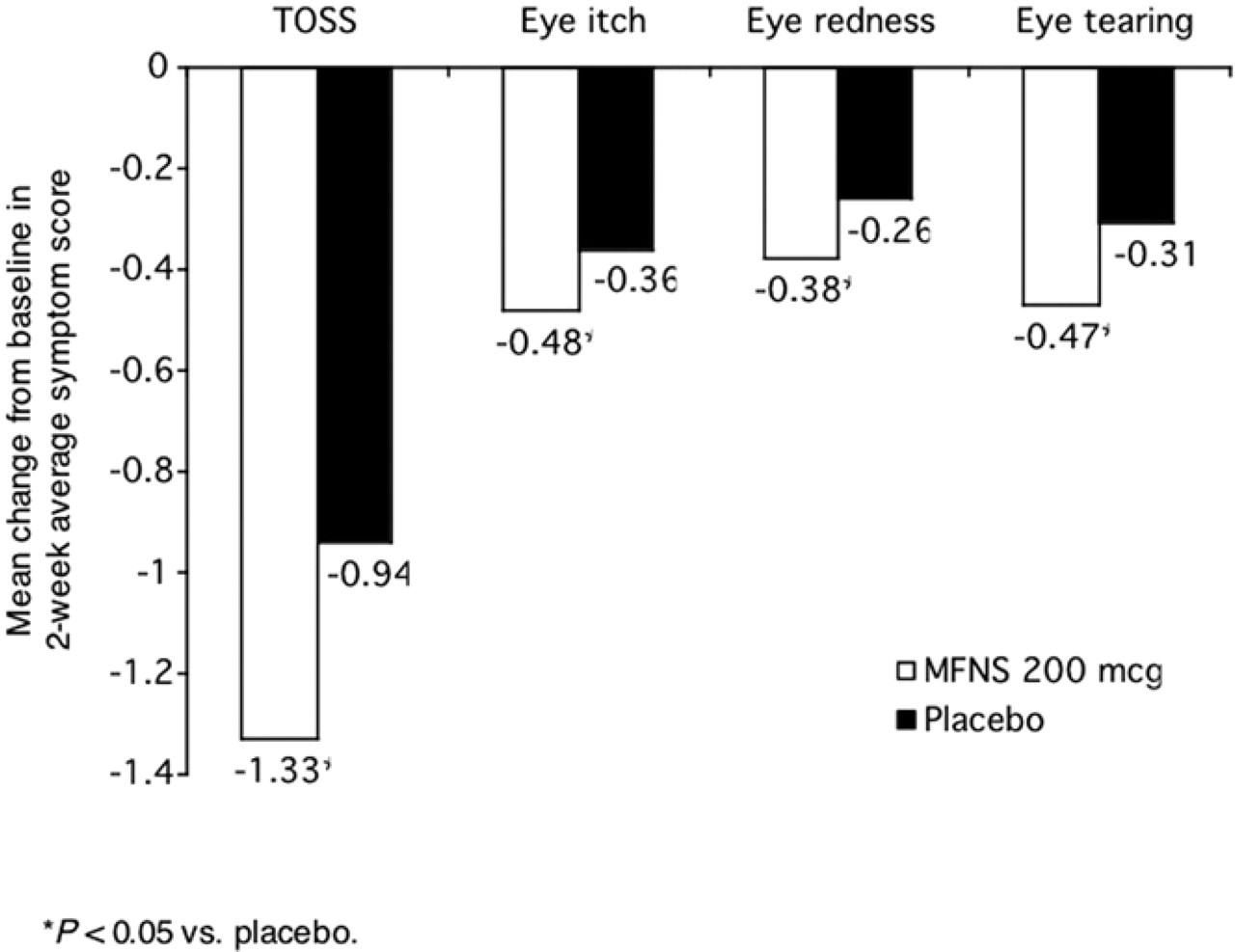
Although ocular symptoms are common in AR patients, interpatient severity is variable, and baseline ocular symptoms have typically not been criteria for eligibility in clinical trials that assess INS treatment for AR. Nevertheless, ocular symptoms are a common outcome variable, and a number of studies have found that INSs are significantly more effective than placebo in reducing ocular symptoms in AR patients (Table 1). 13–15,52–57 In an early trial, total ocular symptoms were significantly lower after treatment with triamcinolone acetonide vs placebo. 58 In a three-arm trial comparing budesonide, fluticasone propionate, and placebo, budesonide, but not fluticasone propionate, significantly reduced total eye symptoms. 58 However, no significant differences in efficacy between the 2 active treatment arms were observed.
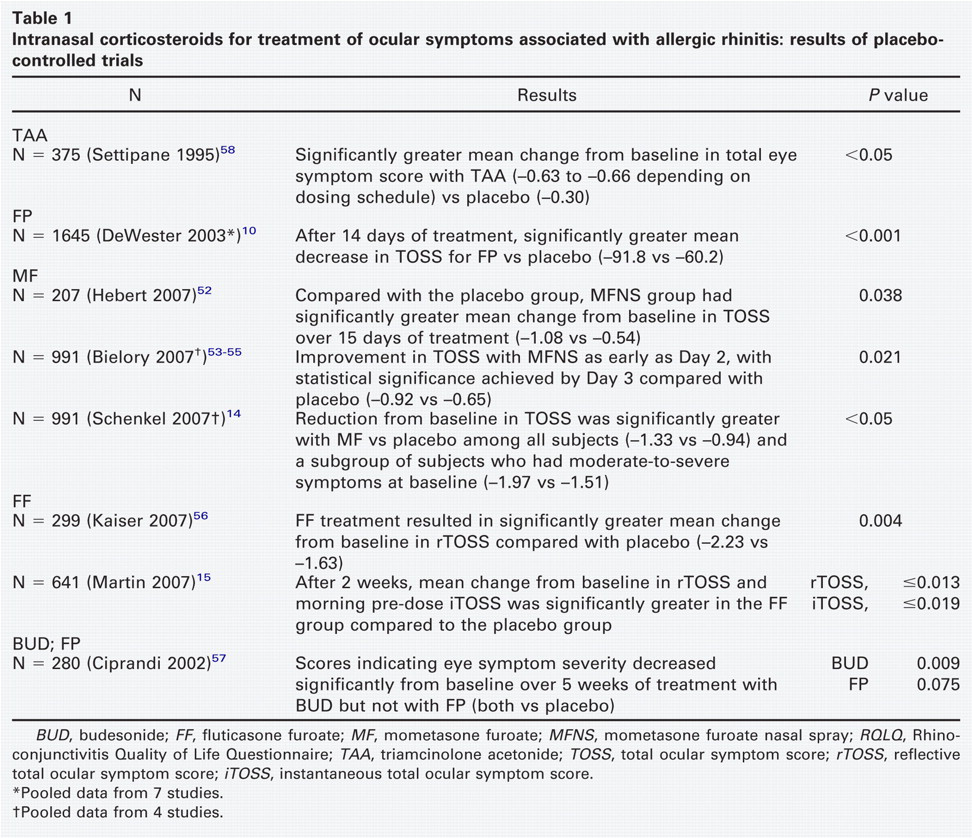
Recently, assessments including total ocular symptom score (TOSS) and component symptom scores for itching, tearing, redness, and puffiness have been used to measure effectiveness of INSs. In a pooled, retrospective analysis of data from 7 randomized, double-blind trials (N = 1645) that compared the efficacy of fluticasone propionate and placebo in SAR patients, fluticasone propionate was found to be significantly more effective than placebo in reducing baseline TOSS after 1 and 2 weeks of treatment (Fig 2). 10
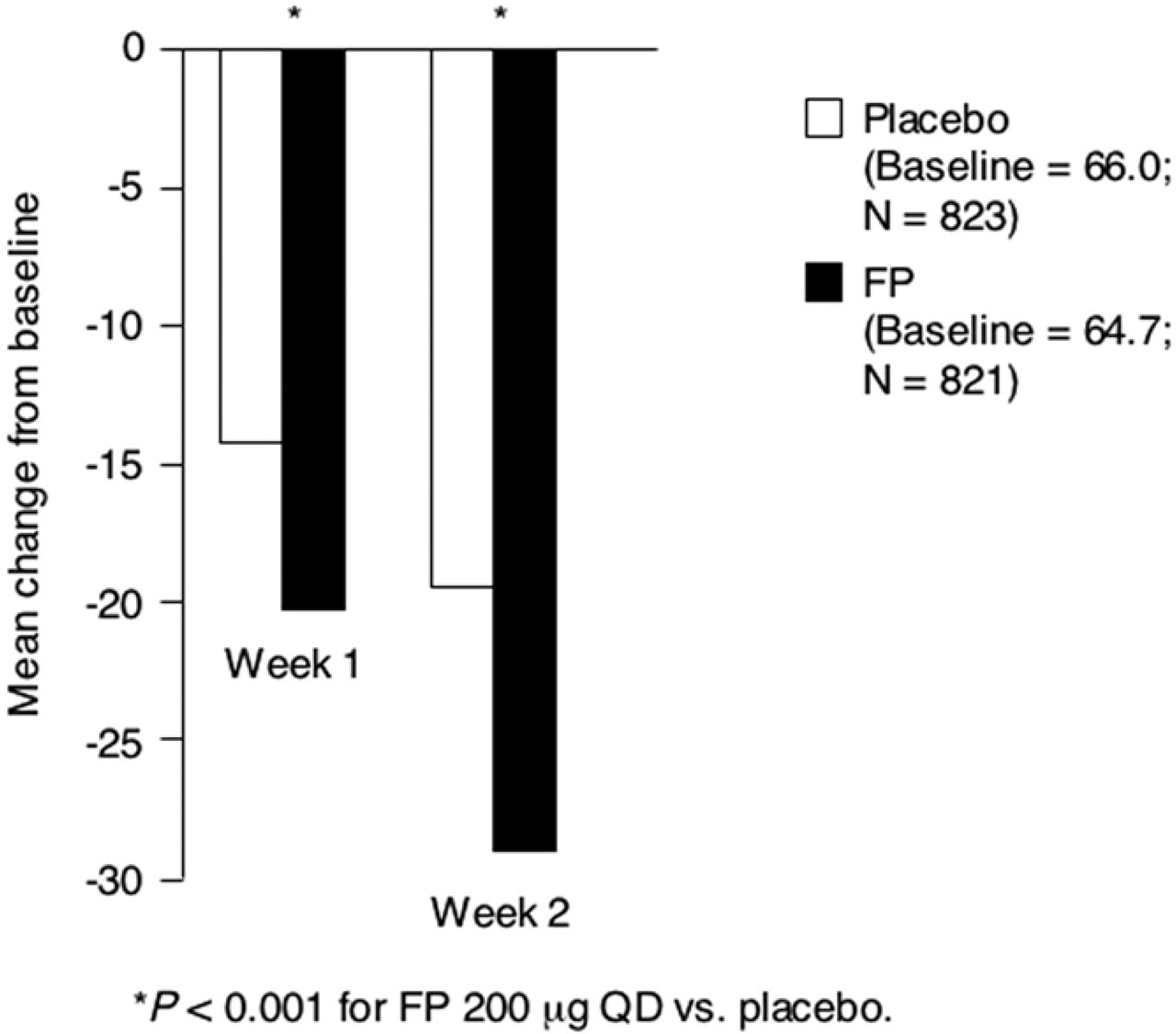
Retrospective analyses assessed ocular symptom data from subjects with SAR who were randomized to receive mometasone furoate or placebo as part of 4 phase III, double-blind trials. 52 Subjects who entered the studies were not required to have ocular symptoms at baseline, and despite the low baseline TOSS, and thus low potential for improvement, significantly greater improvement in TOSS was found with mometasone furoate vs placebo over the 2-week treatment period (Fig 3). Pooled analyses of data from the 4 phase III trials also showed significantly greater reductions in the 3 TOSS component symptoms (itching, redness, and tearing) as well as in TOSS 14 across all degrees of symptom severities at baseline. 55 Benefit was seen as early as day 2, reaching statistical significance at day 3 53 and was sustained throughout the dosing interval. 54
Recently published data indicate that fluticasone furoate is also more effective than placebo in reducing ocular symptoms associated with SAR. In a 2-week, dose-ranging study 15 of fluticasone furoate (55 mcg, 110 mcg, 220 mcg, and 440 mcg, all once daily) in patients with SAR, mean change in reflective TOSS and Rhino-conjunctivitis Quality of Life Questionnaire (RQLQ) eye symptom domain score were significantly greater in all active treatment groups compared with placebo. Comparison of once-daily intranasal fluticasone furoate with placebo in subjects with SAR who had moderate-to-severe TOSS at baseline concluded that mean reductions from baseline were significantly greater with fluticasone furoate than with placebo for TOSS and each of the ocular symptoms. 56
A limited number of studies that compared the effectiveness of different INSs in reducing ocular symptoms in AR patients have been published. In addition to the previously discussed trial comparing budesonide, fluticasone propionate, and placebo, 57 once-daily mometasone furoate (200 mcg) was compared to twice-daily beclomethasone dipropionate (200 mcg) over a 1-month treatment period. 59 Mometasone furoate and beclomethasone dipropionate were superior to placebo in reducing total nasal and nonnasal symptom scores, which included itching, tearing, and redness of the eyes and itching of the ears or palate. No statistically significant differences between the 2 active treatment groups were noted. Triamcinolone acetonide and fluticasone propionate, both once-daily, were compared over a 3-week treatment period in SAR patients. 60 In the ocular outcome variable that was assessed in this study (the eye symptom domain of RQLQ), triamcinolone acetonide and fluticasone propionate were both superior to placebo and were not significantly different from each other.
BUD, budesonide; FF, fluticasone furoate; MF, mometasone furoate; MFNS, mometasone furoate nasal spray; RQLQ, Rhino-conjunctivitis Quality of Life Questionnaire; TAA, triamcinolone acetonide; TOSS, total ocular symptom score; rTOSS, reflective total ocular symptom score; iTOSS, instantaneous total ocular symptom score.
*Pooled data from 7 studies.
† Pooled data from 4 studies.
Intranasal Corticosteroids vs Oral Antihistamines
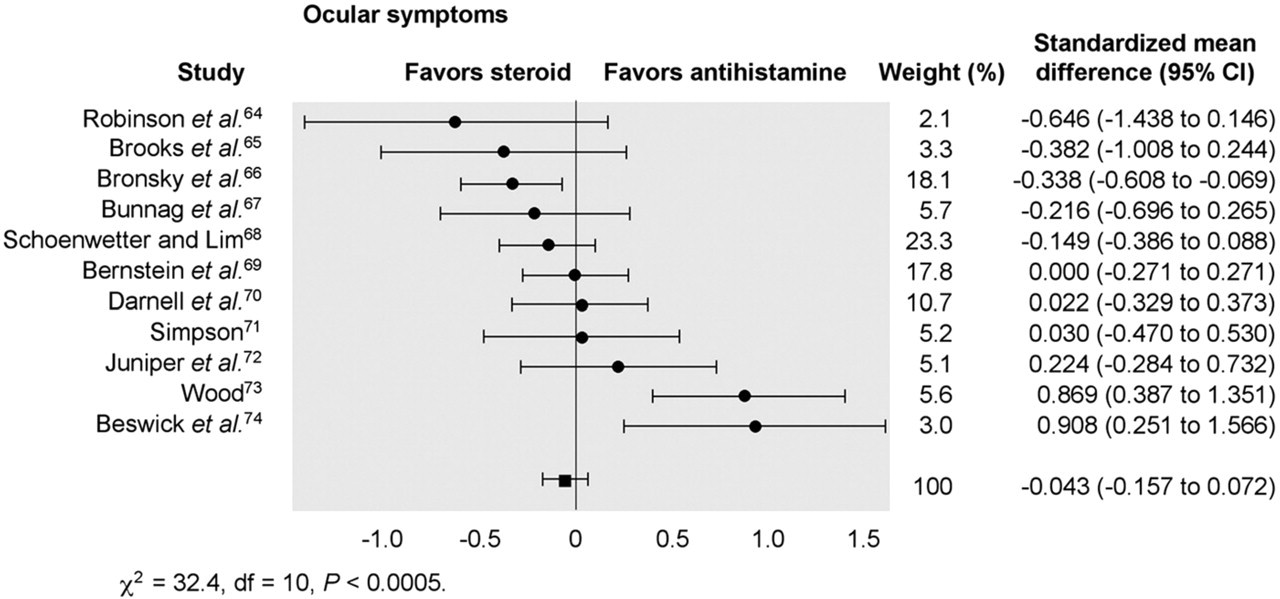
Although INSs are considered first-line therapy for moderate-to-severe AR, because they are especially effective for nasal congestion, 61 nonsedating antihistamines have been recommended over INSs for relief of ocular symptoms. 23,61,62 Contrary to expert opinion, a meta-analysis by Weiner et al 63 of 16 randomized, controlled trials conducted between 1966 and 1997 found that oral antihistamines are not superior to INSs for the relief of ocular symptoms (Fig 4). 63–74 Subsequent to the meta-analysis, loratadine was compared to both fluticasone propionate 75 and triamcinolone 76 in 28-day, randomized, controlled trials for SAR. Treatment with fluticasone propionate was associated with significantly greater reductions in TOSS and individual ocular symptoms compared with loratadine. The percentage of patients who reported relief from ocular symptoms was also higher with triamcinolone than with loratadine, although these differences only became significant in weeks 3 and 4.
Intranasal Corticosteroids vs Topical Antihistamines
Topical ocular antihistamines are noted for their rapid onset of action and are associated with lower rates of sedation and dry eye than first-generation oral antihistamines. 77 There is a perception among physicians that nonsedating oral antihistamines may be preferable to treat coexisting nasal symptoms present in the majority of SAC and PAC patients. 21 A study by Abelson et al 78 (N = 500) demonstrated significant relief of sneezing, itchy nose, and runny nose with olopatadine 0.2% vs placebo (P < 0.05). 78 However, a meta-analysis of findings from 4 published clinical trials that compared the effects of INSs to topical (ocular) antihistamines on ocular symptoms in AR demonstrated no overall significant difference between the 2 treatment modalities (Fig 5). 79,50,79–82
Mean change from baseline total ocular symptom score at weeks 1 and 2 (P < 0.001 versus placebo). Patient-reported data were pooled from 7 studies that included subjects with seasonal allergic rhinitis who were randomized to either once-daily fluticasone propionate nasal spray or placebo (N = 1645). (FP, fluticasone propionate.) (Reprinted from DeWester 2003. 13 )
Proposed Mechanisms of Action of Intranasal Corticosteroids in Ocular Symptoms
The mechanism of action of INSs in relieving nasal symptoms of SAR likely involves multiple pharmacologic actions that address the early- and late-phase allergic reactions found in the nose. These agents have potent anti-inflammatory effects that work by suppressing production of multiple proinflammatory mediators such as cytokines and prostaglandins while inhibiting the action, recruitment, and migration of inflammatory cells. 1 Intranasal corticosteroid therapy has also been found to inhibit seasonal increases in serum levels of circulating IgE antibodies. 83
Though the mechanism of action of an INS spray in relieving ocular symptoms is not fully understood, several mechanisms have been proposed. By decreasing nasal inflammation, INS may modulate or normalize the excess stimulation of reflex neural activity that occurs during allergic reactions and thereby reduce ocular symptoms. 10,29,42,43,84 In addition, by inhibiting local nasal inflammation, ie, production of cytokines and infiltration of inflammatory cells, INSs may have indirect systemic effects that reduce the recruitment of inflammatory cells in other tissues, including the eyes. 85
Some authors have suggested that INSs increase drainage in inflamed nasolacrimal ducts, thereby reducing conjunctival exposure to allergens and inflammatory mediators. 13,75 However, as noted earlier, duct patency has been found to be maintained in subjects with symptomatic allergic response after ocular challenge. 46
Mean changes from baseline in total and individual ocular symptom scores over 14 days. Patient-reported data were pooled from four studies including patients with seasonal allergic rhinitis who were randomized to either once daily mometasone furoate or placebo (N = 991). (MFNS, mometasone furoate nasal spray; TOSS, total ocular symptom score.) (Reprinted from Schenkel 2007. 14 )
Although corticosteroids have potent systemic antiinflammatory effects, systemic absorption of the INS is below the level that would be expected to produce local effects in distant tissues like the eye, especially after it has been diluted by the blood. Therefore, it is unlikely that INSs act systemically to relieve ocular symptoms. 10,75,86 Long-term (1-year) treatment with fluticasone propionate, mometasone furoate, or beclomethasone diproprionate was not found to produce increases in intraocular pressure (IOP) beyond normal limits in adult or pediatric patients. 87,88 In addition, cataracts or glaucoma were not reported among adults who were treated for 12 months with fluticasone propionate. 89 A retrospective analysis of 286,078 oral corticosteroid and INS users found that there was no increased incidence of cataract among INS users. 90 In a study of adolescent and adult subjects who received fluticasone furoate (n = 605) or placebo (n = 201) for 52 weeks, increased IOP was reported in 12 subjects who received fluticasone furoate: 2 subjects at week 12 (21 mm Hg) and 10 subjects at week 52 (21 mm Hg, n = 5; 22 mm Hg, n = 4; and 24 mm Hg, n = 1). Between weeks 6 to 52, 4 subjects in the fluticasone furoate group showed reductions in IOP from a baseline measurement ≥21 mm Hg. None of these changes in pressure were statistically significant or accompanied by changes in the optic disc, a sign of glaucoma. There were 2 cases of posterior subcapsular cataracts not present at baseline, 1 of which was in the placebo group. 91 The risk of cataract formation associated with intranasal steroids is somewhat controversial and may be agent-specific. A population-based survey that incorporated detailed lens assessment found a dose-dependent relationship between lifetime exposure to beclomethasone and cataract formation. 92 It should also be noted that intranasal beclomethasone has a much higher systemic bioavailability (44%) than newer agents such as mometasone furoate and fluticasone propionate (<1%). 93
Meta-analysis compares intranasal corticosteroids and oral antihistamines on allergic rhinitis-related eye symptoms. Significant heterogeneity in findings was related to studies involving the intranasal corticosteroid beclomethasone. Overall, there was no measurable difference in treatment effect between the 2 modalities. (CI, confidence interval.) (Reprinted from Weiner 1998. 63 )
It has been suggested that intranasal steroids might travel through the nasolacrimal duct, exerting their anti-inflammatory effect directly on the conjunctiva. Although blowing smoke through one's lacrimal duct is an occasional party trick, the lack of steroidal side effects such as glaucoma and cataracts indicate that the movement through the nasolacrimal duct is not a mechanism for the ocular effects of INSs.
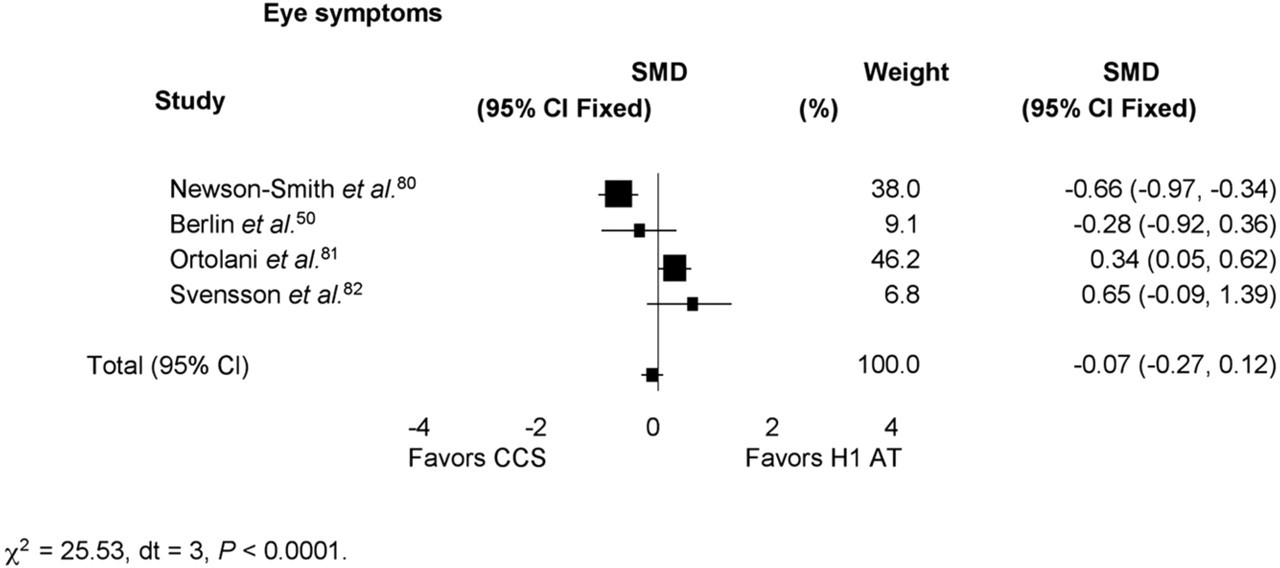
Pooled SMD between intranasal corticosteroids and topical antihistamines on eye symptoms. Width of horizontal line represents 95% confidence interval around point estimate. Size of point estimate represents relative weight (% weight) of each trial in the pooled summary estimate. (CCS, intranasal corticosteroid; CI, confidence interval; H1 AT, topical antihistamines; SMD, standard mean difference.) (Reprinted from Yanez 2002. 79 )
CONCLUSIONS
Ocular symptoms associated with AR represent a major cost to society and significantly reduce the quality of life of sufferers. Those with nasal and/or ocular symptoms associated with AR may benefit from INS treatment, which has demonstrated efficacy in both symptom domains. An agent that has comprehensive coverage of the allergy syndrome will provide benefits to the patient in terms of reduced side effects and increased level of convenience, which is likely to improve compliance. It might even reduce the need for topical intraocular medications, reducing the overall health care costs of treating the disease. Several mechanisms have been proposed to elucidate how a nasal spray also alleviates ocular symptoms, but much remains unknown. Increased knowledge of the pathophysiology of AR-associated ocular allergy will build further understanding of this treatment modality.
AUTHOR INFORMATION
From the University of Chicago Hopsitals.
Corresponding author: Robert Naclerio, MD, University of Chicago Hospitals, 5841 S. Maryland Avenue, MC 1035, Chicago, IL 60637.
E-mail address:
FINANCIAL DISCLOSURE
Editorial support was provided by Adelphi Inc and was funded by Schering-Plough Corporation. The author did not receive an honorarium in connection with the development or submission of this manuscript.