
Abstract
A new method for reducing the inferior turbinate with the use of a microdebrider to remove submucosal tissue was introduced in 1998. The common complications of standard submucous resection of inferior turbinates such as excessive resection, postoperative bleeding, and crusting were largely avoided and limited to postoperative bleeding in 1.6% of patients. This technique was also included in mucosal sparing techniques in turbinate reduction. 6–8
Recently, temperature-controlled radiofrequency tissue volume reduction (TCRFTVR) has been used for the treatment of the hypertrophied inferior turbinates. It uses heat generated from radiofrequency energy to create ionic agitation in the surrounding tissue, which induces submucosal necrosis. The circumscribed area of submucosal necrosis is replaced overtime by fibroblasts. Wound contraction by fibrosis results in submucosal tissue volume reduction and relief of nasal obstruction without causing damage to the overlying mucosa. Previous reports reflected that there is a recovery in patient-reported symptoms of obstruction with more than 90% improvement being achieved 8 weeks after treatment. 9–11
Mucociliary function is an important defense mechanism that protects the respiratory system against bacteria and other foreign particles. Nasal mucociliary function is impaired in the majority of surgical reductions of the inferior turbinate. 5,12 A wider nasal cavity does not necessarily mean that the nose functions are better. The goal of the surgical treatment should be to diminish complaints while preserving functions and optimal volume reduction together. 13
In the present study, the aim is to compare two mucosal sparing techniques in a randomized and single-blinded manner by using both subjective symptoms and objective tests in treatment of nasal obstruction attributable to nonallergic chronic inferior turbinate hypertrophy.
MATERIAL AND METHODS
Study Design
A prospective randomized clinical study was conducted on 30 adult volunteer patients who were chosen from 48 patients who received follow-up care in our clinic with a diagnosis of turbinate hypertrophy. All of these 30 patients had symptoms and signs of nasal obstruction and stuffiness related to enlarged turbinates and were treated between August 2004 and September 2005. All patients gave their written informed consent before being included in the study, which was approved by the Local Ethics Committee. All procedures were performed by one author (K.C.).
Patients
Patients with previous turbinate surgery, septal deformities, nasal polyps or tumor, nasal radiotherapy, or recurrent sinusitis were excluded. Genetic disorders accompanied by ciliary dysfunction, usage of topical or systemic medication with adverse effects on mucociliary functions, smoking, diabetes mellitus, oral steroid use, coagulation disorders, cardiac pacemaker, and uncontrolled hypertension were additional exclusion criteria.
Patients had been treated previously with topical corticosteroids, antihistamines, decongestants, and topical anticholinergic agents. Patients whose complaints had not subsided at all were admitted to the study. Furthermore, patients who were selected to receive surgery had smaller inferior turbinates after the nasal application of topical vasoconstrictive agents.
Forty-eight patients enrolled in the study in the beginning. None of the patients had a history of allergy. The results of skin-prick test, nasal smears, and radioallergosorbent test for specific allergens were all negative when performed on the cases suggested as suspicious for allergic rhinitis with history and physical examination. All patients had a diagnosis of vasomotor dysfunction. Thirty completed the follow-up period. The mean patient age was 29.4 years (± 6.7 years SD). The first patient took TCRFTVR for the right side and resection with microdebrider (SMRM) for the left. The second patient took the operations vice versa according to the sides and operations for the rest of the group followed so forth. A neutral party kept the code as to which treatment modality was applied to which nasal side and disclosed it only at the end of data gathering.
Surgical Procedure
All surgical procedures were performed by the same surgeon (K.C.) in an outpatient facility of a tertiary care center. All of the procedures were carried out with the patient under sedation and local anesthesia (1% lidocaine). Conscious sedation with dormicum under monitorized anesthesic care was performed. Antibiotic therapy with amoxicillin-clavunate and analgesia with acetaminophen were given for 5 days postoperatively.
TCRFTVR
A cotton pledget soaked with 4% pantocaine was placed in the anterior portion of the inferior turbinate for 10 minutes. Afterward a local anesthetic solution of 1% lidocaine was injected. The maximum values of temperature, power, local energy, and duration of the procedure were set preoperatively to 75°C, 8 W, 350 J, and 2.5 minutes, respectively. The radiofrequency energy was delivered by the Somnus S2 radiofrequency generator (Somnus Medical Technologies, Inc, Sunnyvale, CA) successively to three different sites of each turbinate (to the upper and lower area of the anterior portion and to the middle portion).
SMRM
The procedure described by Friedman et al 6 was applied for SMRM. After the application of local anesthesia as described in the TCRFTVR section a 0.5 cm incision was made with a number 15 blade in a vertical manner in the anterior aspect of the inferior turbinate. A submucosal pocket was created with sharp dissection on the medial surface of the bony turbinate. The straight microdebrider with 4-mm tip and tricut blade was applied through the incision. Inferior aspect of the bony turbinate and some of the submucosal tissue was debrided at 3000-cps oscillating mode in a ventrocaudal manner. The entire procedure was performed under endoscopic guidance including the examination of the pocket for bleeding control. Hemostasis was achieved under direct vision with suction electrocautery when necessary. The incision was not closed. Sponge packing was used for 48 hours in case of minor bleeding.
Symptom Evaluation
Each patient used a 10-cm visual analogue scale (VAS) to grade general nasal obstruction (including day-time and night-time nasal obstruction) preoperatively (day 0), at 12th week, and 6th month after surgery. A score of 0 represented no obstruction and no episodes of nasal obstruction and a score of 10 indicated complete as well as constant and unremitting nasal obstruction.
Nasal Epithelial Function
Nasal epithelial function was evaluated at 12th week and 6th month after surgery and in vivo by the saccharin test and in vitro by ciliary beat frequency measurements. Saccharin transit time (STT) was measured after depositing 15 mg of 2% sodium saccharin including 1% indigotin on the floor of the nasal fossa at the level of the head of the inferior turbinate. The patient was asked to swallow every 30 seconds; immediately after he or she tasted the saccharin the test was stopped and the transfer was confirmed by direct viewing of the blue color of indigotin on the pharyngeal wall.
Superficial nasal mucosal cells were collected by brushing from the middle portion of the inferior turbinate under local anesthesia (5% lidocaine). Cells were immediately suspended in 5 mL tissue culture medium IP 199 (Eurobio, France), and ciliary beat frequency (CBF) was measured with a stroboscopic light microscope at room temperature on at least three separate areas and expressed in hertz as the mean of the various measurements.
Acoustic Rhinometry
Acoustic rhinometry (ARM) was performed with Eccovision AR-1003 acoustic rhinometry (Hood Laboratories Inc, Pembroke, MA) in the morning before the operation and repeated at 12th week and 6th month after the procedure. The nasal cavity volumes from nostril to 5 cm were obtained. The 0- to 5-cm range was chosen because it includes the functional nasal valve and much of the septal and lateral erectile tissues. 14,15 In addition, the accuracy of the nasal volume measurement decreases with increasing distance from the nares. 16 The measurements were obtained at the same time during the day from the patients in sitting position and at the same room temperature while the background noise was minimized. The patients were acclimatized for 15 to 30 minutes before taking the measurements that to minimize all mucovascular variations attributable to the decongestive effect of physical exercise. 15 No decongestion was performed to the turbinates during the measurements before or after the operation. 5
Assessment of the Need for Revision Operation
The rate of the need for the revision operation of each treatment modality group was determined between 6 and 12 months period postoperatively. The necessity for the revision operation was assessed depending on the re-evaluation of the patient's symptoms and objective findings. Patients whose symptoms had subsided partially or not at all had worse results in VAS and ARM measurements regarding the different sides of the nasal cavity when compared with preoperative measurements that were accepted as nominees for the revision operation.
Statistical Analysis
The sample size required for the study was calculated based on the primary outcome variable, that is, ARM difference levels. Power analysis identified at least 16 patients as the total sample size required to detect a 3 cm3 difference between preoperative and postoperative 12-weeks measurements with a power of 90% at 5% significance level. Because our sample size is 30 for each group, similar statistical power could be achieved for 1.5 cm3 difference.
Data analysis was performed by using SPSS for Windows, version 11.5. Data were shown as mean ± SD. The differences in means between groups were compared with the Student's t or Mann-Whitney U test, where appropriate. Comparisons within groups were made by using paired t test for CBF and STT, Friedman test for VAS and ARM. A P value less than 0.05 was considered to be statistically significant.
RESULTS
All the patients tolerated both procedures well. In TCRFTVR sides no mucosal erosion, bleeding, or adherent crust formation was observed. The most common complaints were pain and nasal discharge immediately after the treatment, which gradually decreased in 2 days.
In SMRM sides no uncontrolled bleeding was observed during the operation and suction electrocautery was performed in five patients under endoscopic guidance. Mucosal tears were fairly common in 14 (46.7%) of 30 patients, but there was no loss of mucosa. Synechia was observed in two (6.7%) patients. Minor bleeding in early postoperative period was seen in two (6.7%) patients and managed with sponge packing for 2 days. Statistical analysis showed no significant variation between the complication rates of each procedure (P = 0.492)
Subjective Change of Symptoms
In the sides with the inferior turbinates treated with SMRM, the subjective symptoms slightly worsened during the first 3 or 4 days and began to improve in the first postoperative week. Statistically significant improvement in VAS scores was observed at 12th week and persisted at 6th month postoperatively (P < 0.001).
The severity of nasal obstruction after TCRFTVR began to improve from the third day after treatment. Statistically significant improvement in the VAS scores was observed at 12th week and persisted at 6th month postoperatively (P < 0.001). Intergroup comparisons showed no significant difference in the measurements at 12th week and 6th month postoperatively (P = 0.396 and P = 0.451). The results are summarized in Figure 1.
Acoustic Rhinometry
ARM measurements revealed significant nasal volume decrease at 12th week and 6th month postoperatively when compared with preoperative measurements (P < 0.001) whereas, intergroup comparisons showed no significant difference preoperatively and at 12th week and 6 month postoperatively (P = 0.753, P = 0.357, and P = 0.191, respectively). The results are summarized in Figure 2.
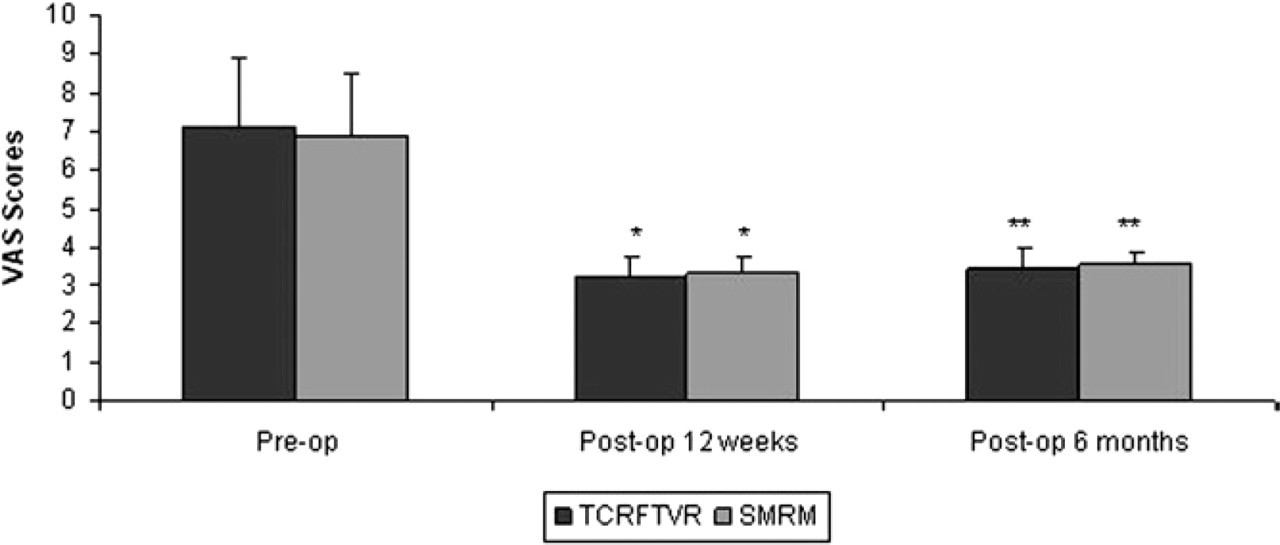
Patient graded mean nasal obstruction (VAS). *Significant difference compared to pre-op (P < 0.001). **Significant difference compared to pre-op (P < 0.001).
Nasal Epithelial Function
STT of the sides where TCRFTVR was performed measured (12.27 min [±1.72 min SD]) at 12th week postoperatively and (11.65 min [± 1.23 min SD]) 6th month postoperatively. The same measurements for SMRM sides were (11.85 min [± 2.03 min SD]) and (11.05 min [± 1.78 min SD]), respectively. The differences were observed as being not statistically significant when intergroup comparisons were made at 12th week and 6th month postoperatively (P = 0.391 and P = 0.134, respectively). The results are summarized in Figure 3.
The CBF on the sides where TCRFTVR was performed measured (12.6 Hz [±0.8 Hz SD]) at 12th week postoperatively and (12.8 Hz [±0.7 Hz SD]) at 6th month postoperatively. The same measurements for SMRM sides were (12.8 Hz [±1.1 Hz SD]) and (13.1 Hz [±0.9 Hz SD]), respectively. The differences were observed as being not statistically significant when intergroup comparisons were made at 12th week and 6th month postoperatively (P = 0.424 and P = 0.155). The results are summarized in Figure 4.
Assessment of the Need for Revision Operation
The necessity for the revision operation was assessed as 4 over 30 sides (13.3%) for the TCRFTVR operation and 2 over 30 sides (6.7%) for the SMRM operation. The intergroup difference was not statistically significant (P = 0.671).
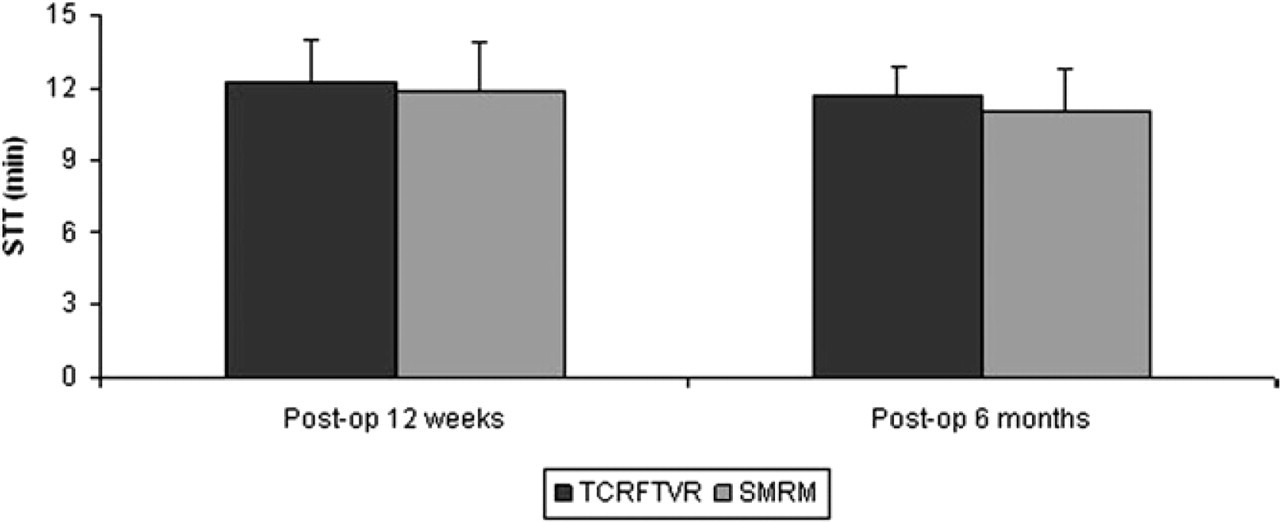
Mean saccharine transport time (STT) measurements.
DISCUSSION
In evaluating the various methods of turbinate reduction, above all, we must consider the function of the turbinates. All methods should be judged by two basic criteria: the efficacy of the technique in alleviating breathing obstruction and the side effects that occur in the short- and long-term. 5 In their review, Hol and Huizing 13 evaluated 13 surgical techniques that have been used for inferior turbinate hypertrophy over the past 130 years and concluded that intraturbinal turbinate reduction should be the method of choice. Any of the described techniques ought to achieve optimal volume reduction with preservation of function. The surgical methods are associated with varying morbidity, and the outcomes of various procedures are variable. Our study, which compares two methods of turbinate reduction, differs in several aspects from the previous reports in the literature. The comparison of two minimally invasive mucosal sparing procedures as TCRFTVR and SMRM, relatively long follow-up period and randomized, single-blinded, and controlled manner of the study design, are the points that make our study unique among others in the literature.
Inferior turbinate surgery is advocated for relief of symptoms in patients with chronic nasal congestion. Numerous reports substantiate the usefulness of inferior turbinate surgery. 17,18 Our patients had significant symptomatic relief after TCRFTVR and SMRM, and our findings are consistent with other techniques reported in the literature. Inter-group comparison shows no significant variation of symptomatic relief at 12th week and 6th month postoperatively.
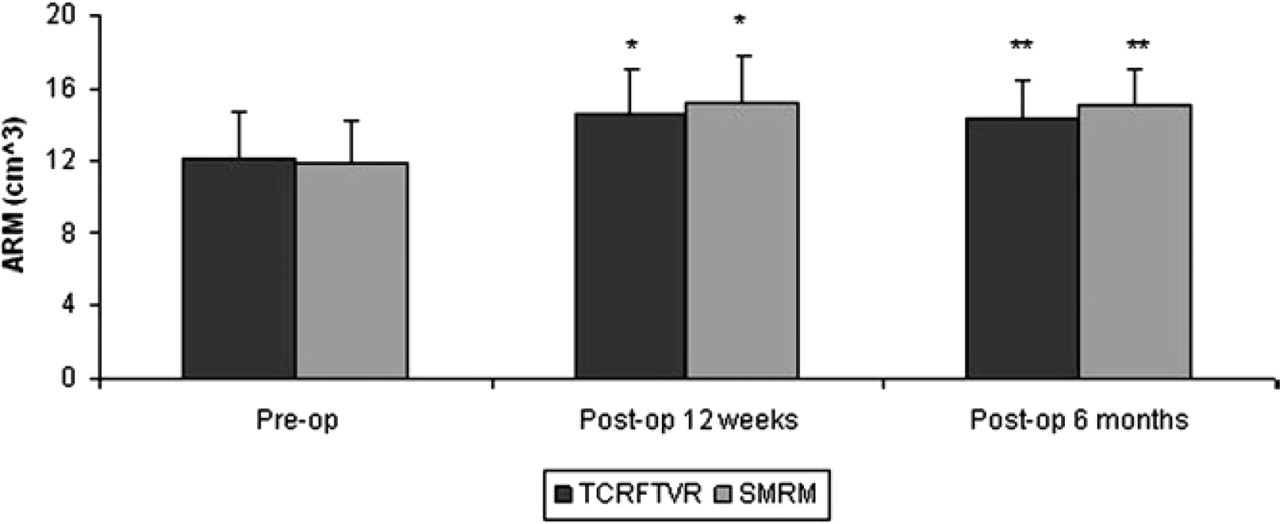
Mean acoustic rhinometric (ARM) measurements. *Significant difference compared to pre-op (P < 0.001). **Significant difference compared to pre-op (P < 0.001).
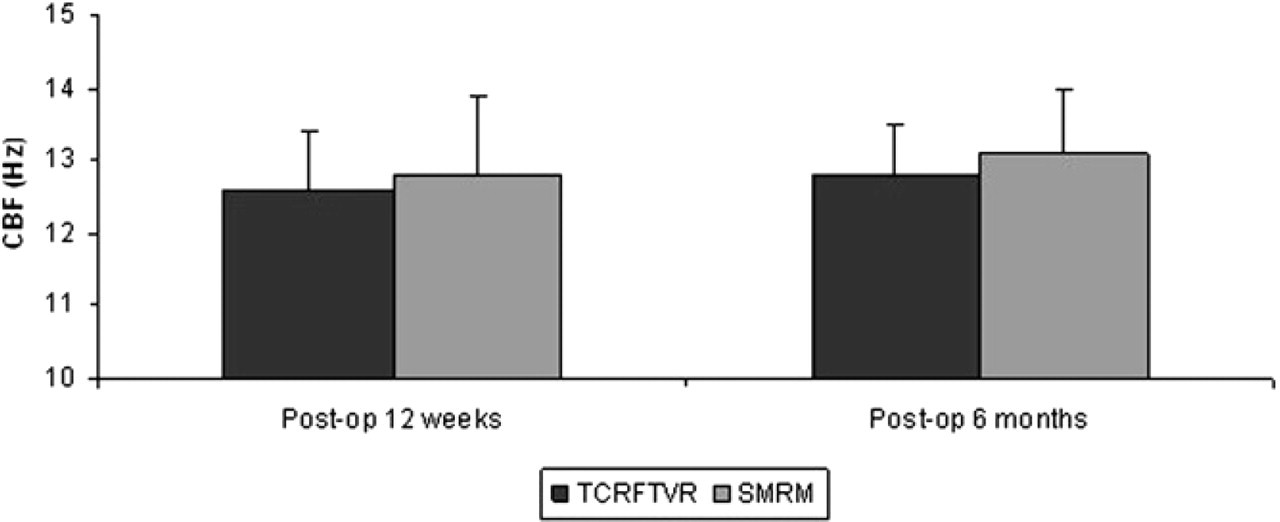
Mean cilliary beat frequency (CBF) measurements.
The ideal turbinate surgery would be limited to the erectile submucosal tissue and to the bony turbinate. Reduction of bone creates more space, whereas surgery on submucosal tissue creates scarring that minimizes the engorgement of the inferior turbinates of patients with vasomotor rhinitis. Preservation of mucosa improves the chances for continued function of the inferior turbinates to warm and humidify the inspired air. 6 Although the TCRFTVR technique does not deal with the bony portion of the turbinate, it leads indifferent results in objective and subjective parameters from the SMRM in our study. Excluding the intervention to the bony turbinate makes TCRFTVR an easier and more minimally invasive procedure than SMRM.
In TCRFTVR, the target tissue temperature can be maintained between 60° C and 90° C with relatively low energy and avoid damage to the surrounding tissue. 11,19 The intent of tissue volume reduction is to induce submucosal fibrosis of the turbinate, which will adhere the mucosa to the turbinate periosteum and will reduce blood flow to turbinate, and render it less prone to swelling and edema. Because of the aforementioned facts, TCRFTVR spare the mucosa itself and its functions.
Mucociliary transport is affected by ciliary movement and rheological properties of the nasal mucus. 19 In this study, CBF and STT of TCRFTVR revealed identical results when compared with SMRM as another mucosa sparing procedure. In a previous study, transmission electron microscopy performed 1 year after radiofrequency turbinate reduction showed that the epithelium was intact with ciliated and goblet cells. 9 Our study compared two mucosa sparing procedures as TCRFTVR and SMRM for the first time and exhibited identical CBF and was able to ensure effective mucociliary clearance as evaluated by the STT results. Other turbinate surgery techniques are unable to preserve the nasal epithelium and its function to this degree. 4 As in any nasal surgical procedure, it is always important to preserve the major epithelial function, that is, mucociliary clearance, which is the first line of defense of the airways.
Except for the article by Joniau et al 20 that emphasized the comparison of powered turbinoplasty and submucosal cauterization, the lack of prospective comparative studies on surgical techniques for turbinate reduction has been highlighted, especially those with long term follow-up. To ensure the ethical standards and statistical value of the study, the assessment of subjective and objective parameters were stopped in the end of the 6th month after the surgery. For the evaluation of the need for revision operation, an additional 6-month period was used. Although the difference for the necessity of revision operation with respect to two different interventions was not statistically significant, lesser rate in SMRM might indicate the need for arranging future studies with larger patient numbers and longer follow-up periods.
One theoretical concern about SMRM is the risk for epistaxis when compared with TCRFTVR. In our study, no postoperative major bleeding was encountered with either technique. The use of an endoscope provides excellent visualization of the surgical field in general and the location of intraoperative bleeding in particular allows precise cauterization with minimal collateral thermal damage. 20
In contrast to SMRM, TCRFTVR does not require nasal packing and thus increases the patient comfort. Although we used a 4 mm tricut blade that can be speculated to decrease the mucosal tears, bleeding, synechia, and packing requirements, the mucosal tears and synechia were observed in SMRM sides. This could be regarded as another factor giving advantage to the TCRFTVR against SMRM.
In this study, we demonstrated that TCRFTVR for the inferior turbinate hypertrophy is as effective as SMRM in improvement of nasal obstruction subjectively and objectively and in preserving nasal mucociliary function. The only disadvantage of this procedure in our country may be the high cost of the disposable needle tip compared with multi-use tips in SMRM. Thus, research on cost-effectiveness is needed for the future.
CONCLUSION
TCRFTVR for inferior turbinates reduces nasal obstruction and protects nasal epithelial functions as does SMRM. Indifferent results in objective and subjective parameters that include epithelial function tests, lack of need for nasal packing, absence of complications like synechia formation, and being more minimally invasive give advantage to TCRFTVR against SMRM, another mucosa-sparing procedure in inferior turbinate reduction.
ACKNOWLEDGEMENTS
The authors thank P.Sc. Salih Ergocen for the statistical analysis of the clinical data. Appreciation is expressed for the insight of Associate Professor Pasa Tevfik Cephe from Gazi University, English Literature Department, during the course of this manuscript preparation.
AUTHOR INFORMATION
From the Ministry of Health Ankara Training and Research Hospital, Ear, Nose and Throat Department, Ankara, Turkey.
Corresponding author: Kursat Ceylan, 4. Sok. Manolya Apt. 22/27, Sogutozu Ankara, Turkey.
E-mail address:
AUTHOR CONTRIBUTION
FINANCIAL DISCLOSURE
None.