
Abstract
Management of ABRS primarily involves treatment with an oral antimicrobial agent, although about 40 percent of cases will resolve with placebo treatment. 2 Several oral antibiotics have been approved by the Food and Drug Administration (FDA) for treatment of ABRS. The choice of an oral antibiotic depends on factors such as severity of symptoms, comorbid medical conditions, prior antibiotic treatment, antibacterial resistance in the local community, tolerability, convenience, and cost of treatment. 3 Recent studies suggest that anti-inflammatory therapy (specifically intranasal steroids) might reduce the severity and shorten the duration of symptoms when used either in combination with antibiotics or as monotherapy for ABRS. 4,5
There has been an attempt to use topical nasal antibiotics as an alternative treatment modality for the management of patients who have chronic rhinosinusitis that is refractory to other treatments. 6–8 Although these preliminary studies show some promising results, they can be criticized. In particular, the role of bacteria in chronic rhinosinusitis (as opposed to acute exacerbations of chronic rhinosinusitis) is often questioned, and the pathophysiology of the disease is increasingly thought to be related to chronic inflammation. Few studies have explored the effect of intranasal administration of antibiotics on objective end points of ABRS such as nasal bacterial and inflammatory cell counts. The major limitation of currently published studies is that they cannot be performed easily on human subjects. We previously developed a mouse model of ABRS after intranasal inoculation with Streptococcus pneumoniae that mimics the disease in humans, is easy to manipulate, and allows objective measurement of infection. 9
Our purpose in the current study was to determine whether treatment of ABRS in mice with topical ciprofloxacin and/or dexamethasone results in a decrease in the number of bacteria and inflammatory cells involved in the disease process.
METHODS
Experimental animals
Pathogen-free, 6- to 8-week-old C57B1/6 female mice were purchased from Jackson Laboratories (Bar Harbor, ME). Each group of animals was kept isolated from the other groups in a biohazard containment facility. All animals were used in protocols approved by the Animal Care and Use Committee of the University of Chicago.
Bacteria
S pneumoniae (ATCC 49619) was used for induction of acute rhinosinusitis as described previously. 9,10 The strain is antigenically similar to type 19 S pneumoniae, the most common strain cultured from human maxillary sinuses during ABRS. S pneumoniae was grown on blood agar plates, and bacterial colonies were suspended in sterile saline solution immediately before inoculation of the mice. A turbidity equivalent to McFarland number 3 was used, which corresponds to approximately 1.2 × 10 9 colony-forming units per millimeter (CFU/mL).
Experimental design
The mice were allowed to acclimate for 1 week in a pathogen-free environment. Then 25 μL of S pneumoniae suspension was placed in each nostril of each mouse. Because mice are obligatory nasal breathers, the fluid was drawn into their nasal passages during inhalation. Treatment was started 1 day after intranasal inoculation with S pneumoniae (Fig 1). Twice daily, 50 μL of each drug was placed in each nostril. There were three groups of 10 mice per time point; 2 mice were uninfected, untreated, and used as controls. The three treatment groups were placebo, Ciprodex Otic Sterile Suspension (0.3% ciprofloxacin/0.1% dexamethasone; Alcon Laboratories, Fort Worth, TX [Ciprodex is a registered trademark of Bayer AG, licensed to Alcon, Inc]), and 0.1% dexamethasone suspension (Alcon Research, Ltd). Investigators were blinded to the drugs. As described in Figure 1, the mice were killed on the mornings of days 3 and 10, and a nasal lavage was performed to count the number of S pneumoniae colonies. The sinuses were harvested and prepared for flow cytometric analysis.
Nasal cultures
Immediately after the mice were killed, the nasal lavage was performed with 200 μL of phosphate-buffered saline (PBS). The lavage liquid was then serially diluted (neat, 1:10, 1:100, 1:1000, and 1:10,000) and, at each dilution, plated onto Columbia sheep blood agar plates. The plates were incubated for 24 hours; then the bacterial colonies were counted. The results were quantified as colony-forming units per millimeter.
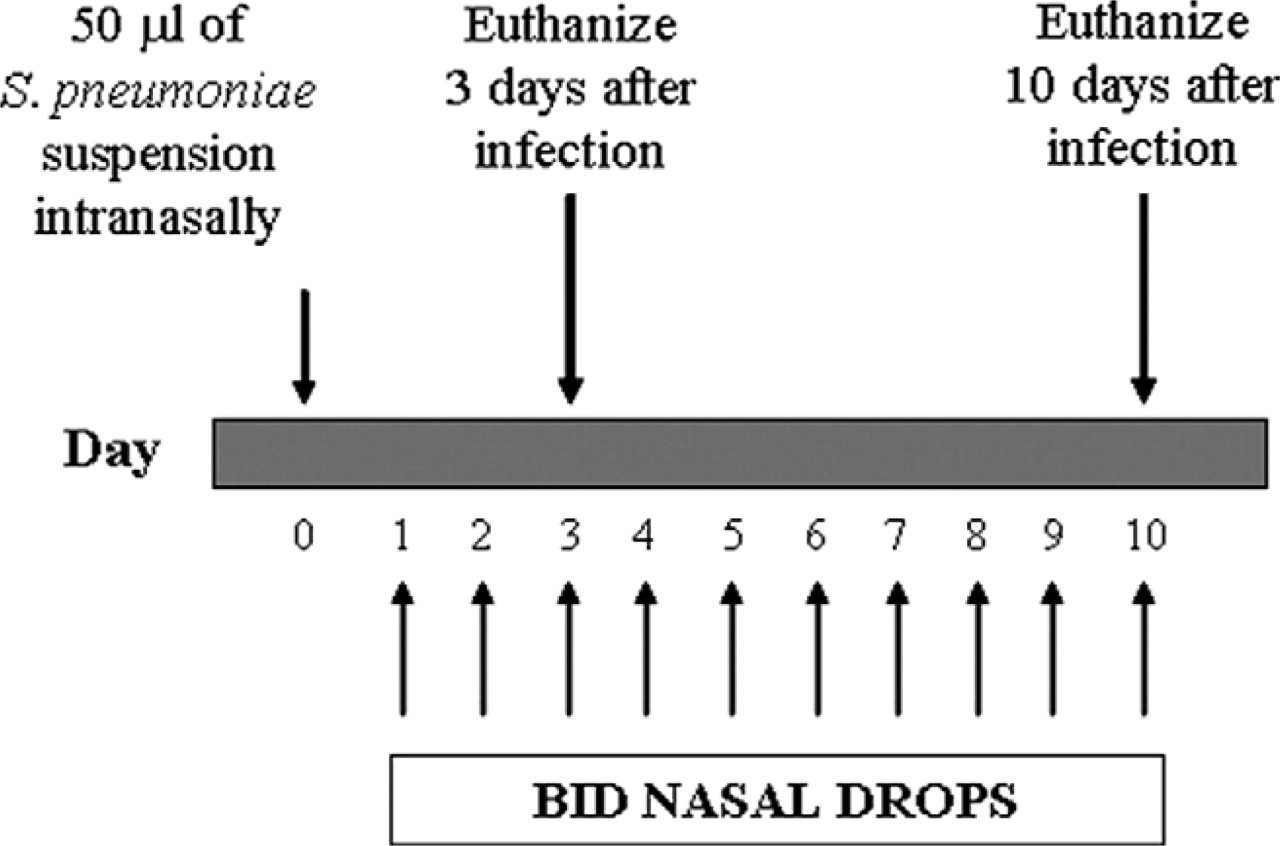
Schematic drawing of study protocol.
Tissue harvesting and processing
Flow cytometric analysis was used for quantifying the cells present in the sinuses. The spleen of each mouse in the control group was harvested as a positive control. We removed the skin and tissue from the head of all mice and then sagittally bisected the skull to expose the sinuses. The tissue from the sinuses was removed manually. The harvested tissue was placed in 2 mL of PBS with collagenase P (Roche Diagnostics, Indianapolis, IN) at a final concentration of 1 mg/mL and incubated at 37°C for 1 hour in a water bath shaker. After tissue degradation, the suspension was passed through a Nytex filter (Sefar-America Inc, Depew, NY), and the cells were recovered in Dulbecco minimum essential medium with 5-percent fetal calf serum (medium). Next, we centrifuged the cells at 1350 rpm for 5 minutes at 4°C and then discarded the supernatant. The centrifuge conditions were the same for all experiments.
We then resuspended the cell pellet in 2 mL of the medium and quantified cells with 0.4% trypan blue on a hemocytometer. Using the calculated live cell number, we aliquoted cells to a concentration between 1 × 10 5 and 5 × 10 5 per tube. All of the tubes were filled with buffer and centrifuged. We then added 20 μL of 2.4 G2 (an anti-FcγRII/III antibody that stops nonspecific binding [BD Biosciences Clontech Labs, Palo Alto, CA]) and incubated the tubes for 15 minutes at room temperature. Next, we added 10 μL of the antibody or antibodies diluted to the titration amount; then the tubes were incubated for 45 minutes at 44°C. After incubation, we again added buffer, and the mixture was centrifuged. Finally, we added 300 μL of buffer. Flow cytometry was performed on a 3-detector BD FACScan or a 6-detector BD LSR (both from BD Bio-sciences Clontech Labs). Cells were stained with antibodies against GR1 (neutrophils), CD11b (macrophages), and CD4 and CD8 (T cells).
Statistical analysis
The number of animals required for the experiment was determined according to a standard power formula. We determined the number of mice needed to provide 90-percent power to detect a difference between groups of animals killed on day 3 for the primary outcome variable (the number of bacteria recovered). We used a 2-tailed significance level of 0.05. Standard deviations from the previous experiments were used in the sample-size calculations, and the specified differences to be detected were those observed previously. The data from our previous studies suggested that the standard deviations of our primary outcome variables were proportional to their means; thus, we used a logarithmic transformation to stabilize the variances. We concluded that eight mice at each time point provided adequate power, and we assumed that two mice would be lost from each group for technical reasons.
Log conversion of the flow cytometric and culture data was performed for normalization of the data. First, 1-way analysis of variance (ANOVA) was applied to the data. If significance was obtained, parametric 2-tailed t tests were used to make comparisons between groups and treatments. A 2-tailed P value < 0.05 was considered statistically significant.
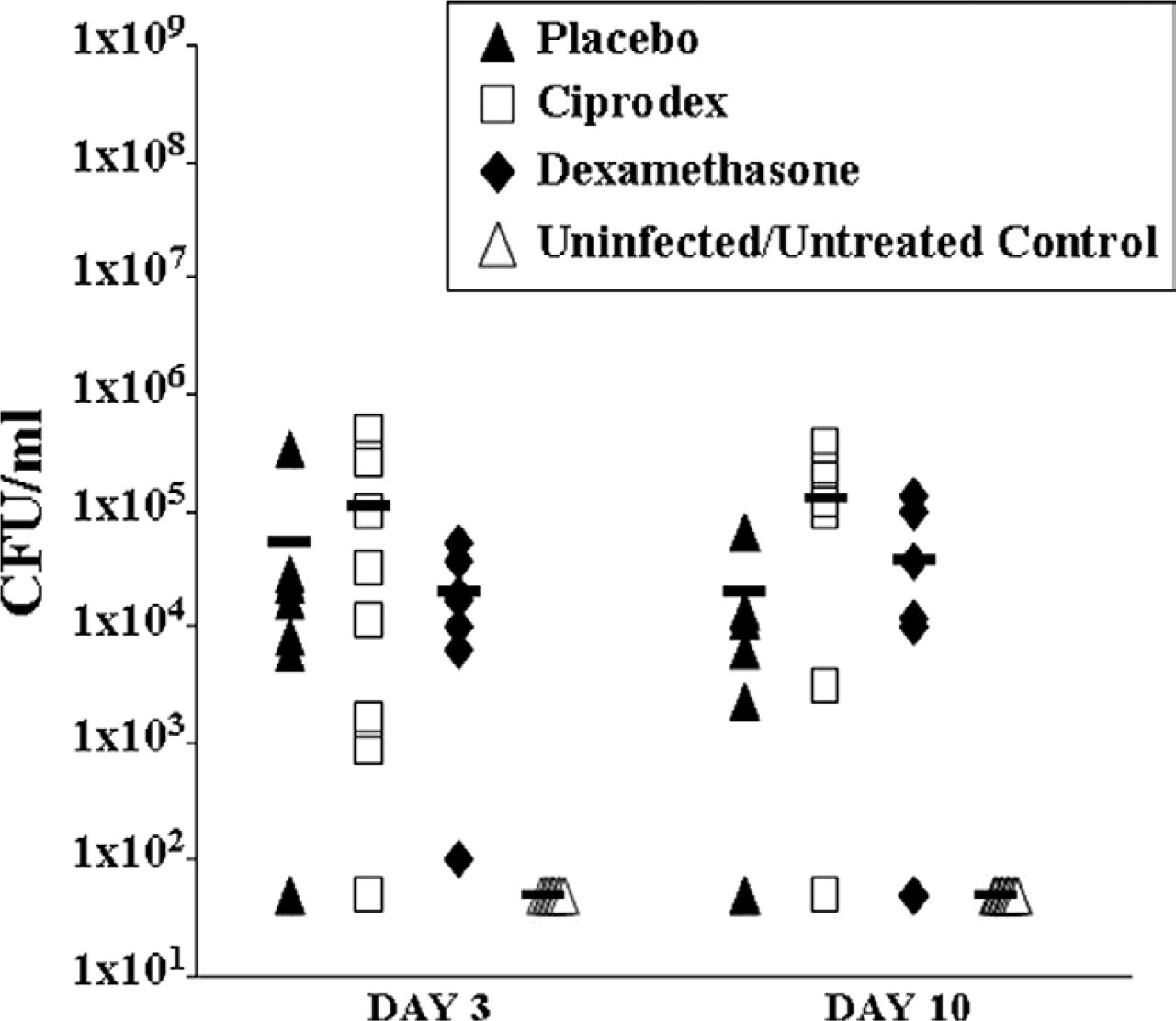
Results of nasal lavage cultures on days 3 and 10. Each symbol represents the result for one mouse. Horizontal bars represent the mean for the group. The infected groups had significantly more bacteria than the uninfected group, and there were no statistical differences among the infected groups regardless of treatment.
RESULTS
After the inoculation of S pneumoniae, the mice did not appear to be ill, except for one mouse in the Ciprodex group. This mouse had partial hair loss on one leg and seemed somewhat lethargic on the third day after treatment with the nasal drops had begun, but it recovered spontaneously.
Day 3 changes
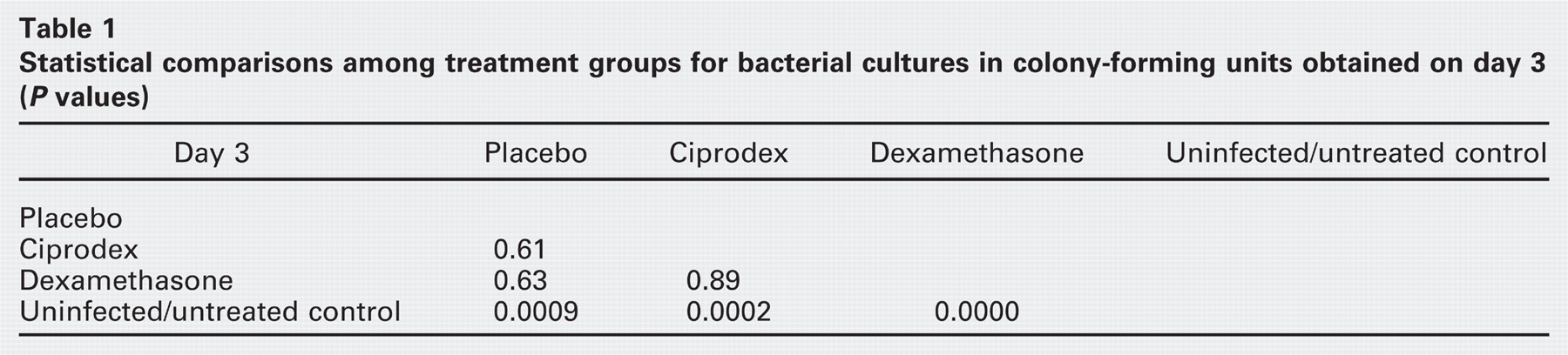
We first compared the number of bacteria recovered from nasal lavage cultures 3 days after infection with S pneumoniae. There was a significant difference among groups (ANOVA P < 0.0001; Fig 2). The number of bacteria recovered from all treatment groups was significantly greater than that from the uninfected control group; Table 1 provides data regarding P values. We observed a lack of effect of both Ciprodex and dexamethasone on the number of bacteria recovered from nasal lavage cultures compared with placebo (Fig 2).
We then compared the number of inflammatory cells (granulocytes, monocytes, CD4+, and CD8+ cells) in the sinuses of the animals obtained by flow cytometric analysis 3 days after infection with S pneumoniae. There was a statistically significant difference in the number of granulocytes and monocytes among all groups (ANOVA P = 0.0067 and P = 0.0144, respectively; Fig 3). The number of CD4+ and CD8+ cells did not differ among the groups (ANOVA P = 0.42, P = 0.30, respectively; Fig 4). There was a significant increase in the number of granulocytes and monocytes of all infected mice compared with the uninfected control group (P < 0.05 for all; Fig 3). We did not detect significant differences among infected groups of mice in the number of any inflammatory cells.
Day 10 changes
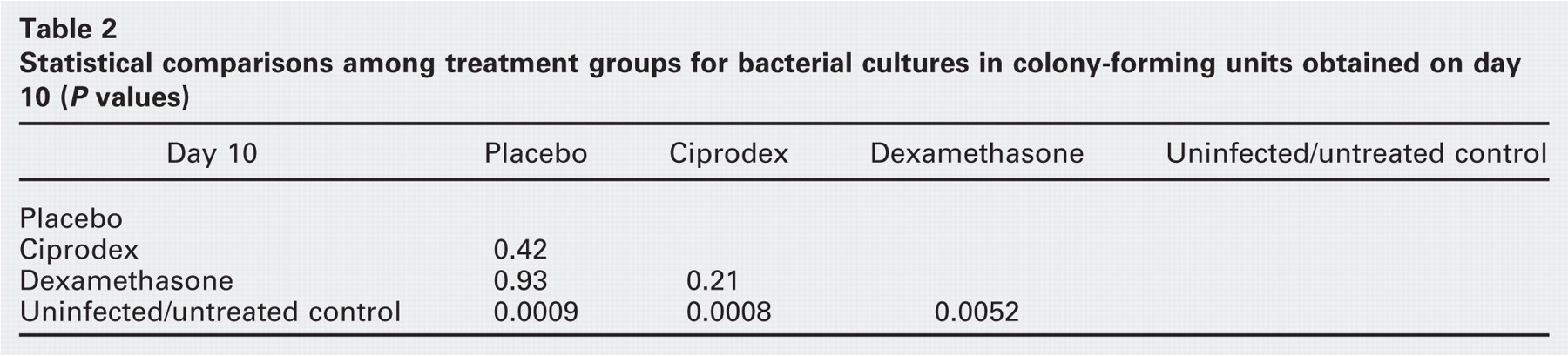
We compared the three treatment groups on the basis of the number of bacteria recovered from nasal lavage cultures 10 days after infection with S pneumoniae. There was a significant difference among groups (ANOVA P = 0.0021). The number of bacteria recovered from both treatment groups was significantly higher than bacteria recovered from the uninfected control group; Table 2 lists P values. There was no difference in the number of bacteria among the treatment groups.
We compared the three treatment groups on the basis of the number of inflammatory cells in the sinuses of the animals obtained by flow cytometric analysis 10 days after infection with S pneumoniae. We did not detect significant differences among infected and uninfected groups of mice in the number of inflammatory cells in the sinuses. Similarly, no significant differences were observed in the number of inflammatory cells in any of the treatment groups (Figs 3 and 4).
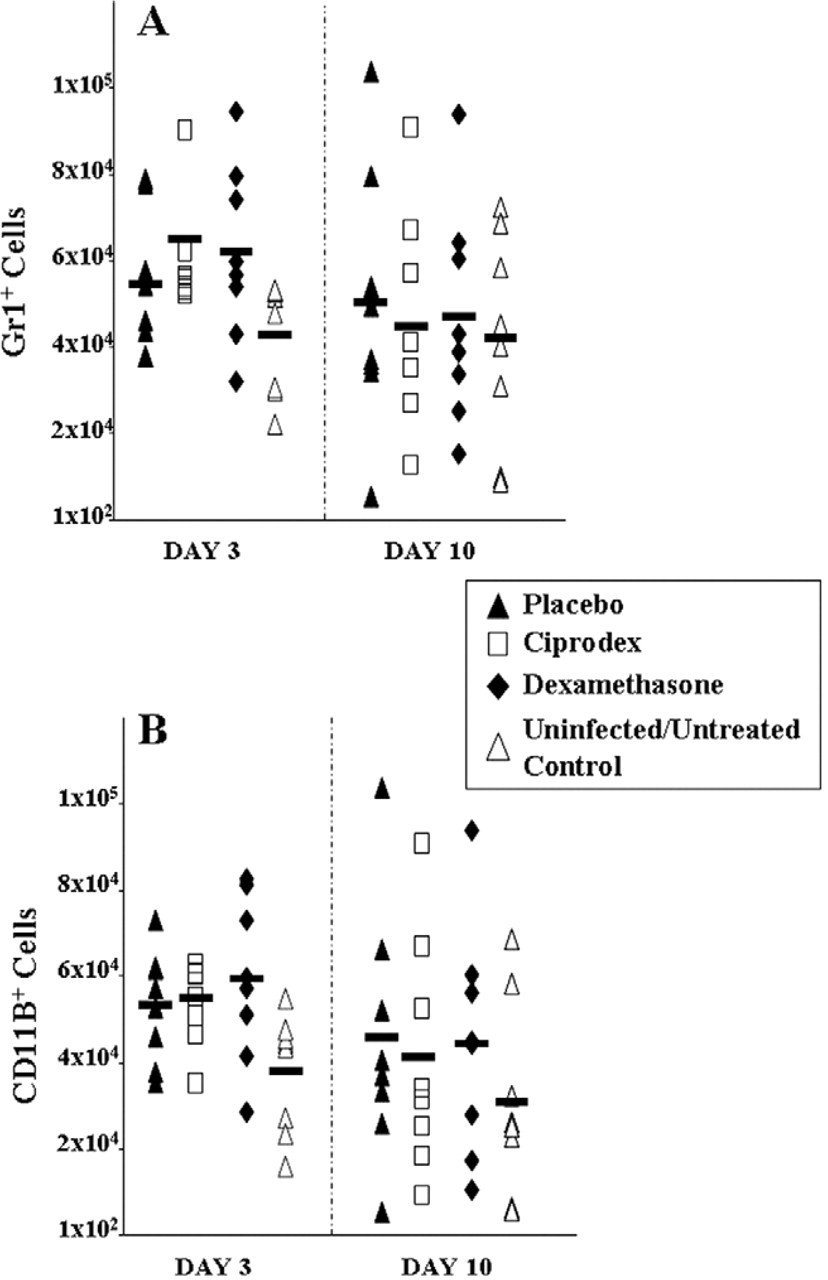
Sinus cellular response on days 3 and 10. (A) GR1 + cells, (B) CD11B + cells. Each symbol represents the result for one mouse. Horizontal bars represent the mean for the group. The infected groups had significantly more bacteria than the uninfected group. There were no statistical differences among the infected groups regardless of treatment.
Day 3 vs Day 10
Next, we compared the three treatment groups on the basis of the effect of each treatment on the number of bacteria and inflammatory cells recovered from nasal lavage cultures on days 3 and 10.
Placebo group. Although the numbers of bacteria had decreased on day 10, placebo nasal treatment had no statistically significant effect on the number recovered from nasal lavage cultures (P = 0.8014). Similarly, there was no substantive difference in the number of any of the inflammatory cells after treatment with placebo drops.
Ciprodex group. Nasal culture results after 10 days of treatment with nasal Ciprodex drops did not differ significantly from nasal culture results on the third day of treatment (P = 0.9152). However, nasal Ciprodex drops caused an almost statistically significant decrease in the number of granulocytes after 10 days of treatment (P = 0.0522). The number of monocytes tended to be lower posttreatment; however, this difference did not reach statistical significance (P = 0.094). No substantive differences in the numbers of CD4+ and CD8+ cells were found in a comparison of day 3 with day 10.
Dexamethasone group. Intranasal treatment with dexamethasone drops had no statistically significant effect on the number of bacterial counts in recovered nasal lavages (P = 0.4325). Although the numbers of granulocytes and monocytes were lower on day 10 than on day 3, this difference did not reach statistical significance (P = 0.15 and P = 0.15, respectively). Similarly, the number of CD4+ cells and CD8+ cells did not show any substantive difference posttreatment.
DISCUSSION
The benefits of local delivery of medications to the nasal cavity include direct contact of the medications with the diseased mucosa, the potential for higher local concentrations of the drugs, decreased systemic exposure, avoidance of first-pass metabolism by the liver, and rapid onset of action. 11,12 The use of topical medications in chronic rhinosinusitis is common. These medications include corticosteroids, antihistamines and, occasionally, antibiotics. 13 Topical intranasal corticosteroids are commonly prescribed to decrease mucosal edema and nasal inflammation, whereas topical antibiotics have been used to treat local infections, particularly vestibulitis, in the nasal cavity. The role of these topical medications in ABRS has not been thoroughly studied.
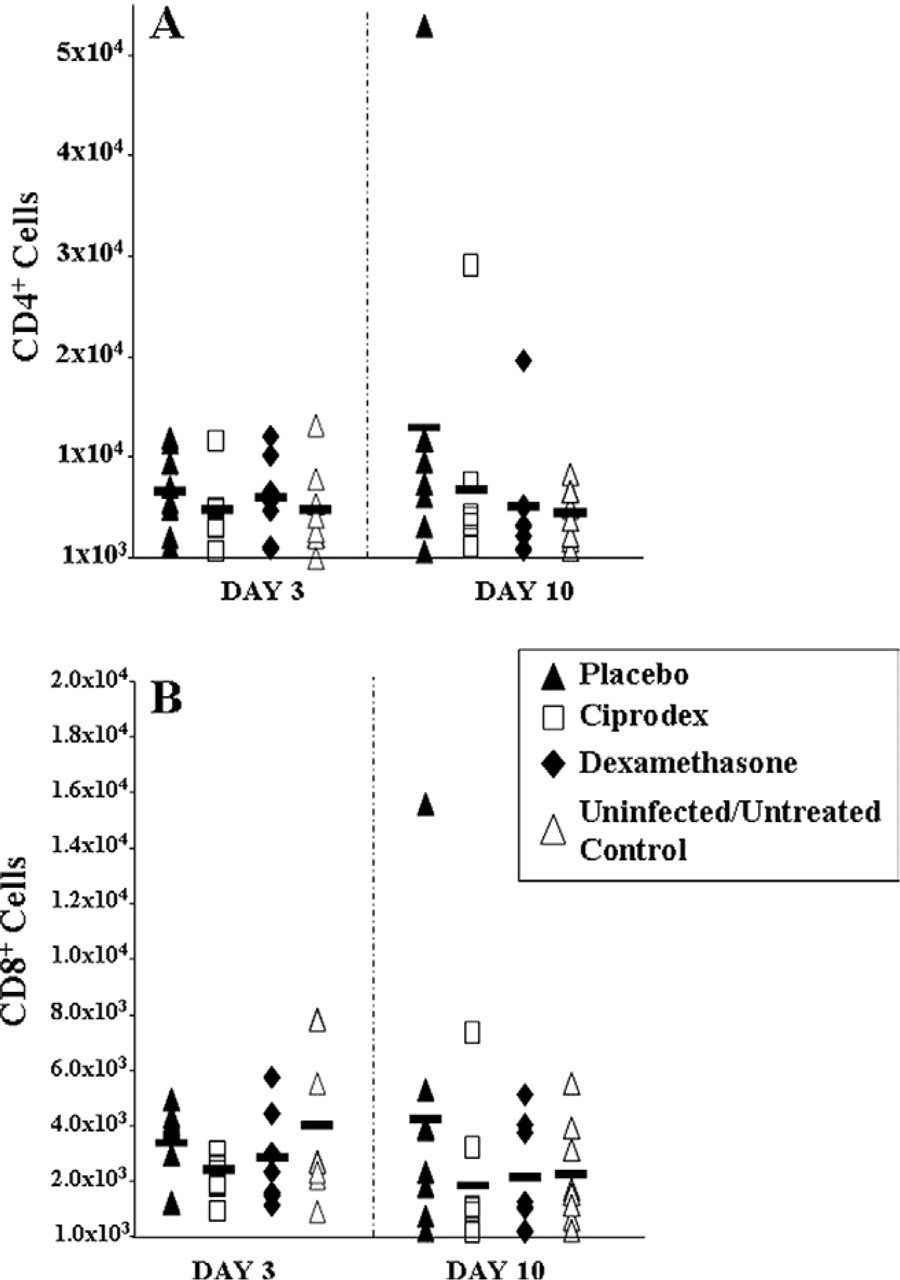
Sinus cellular response on days 3 and 10. (A) CD4+ cells, (B) CD8+ cells. Each symbol represents the result for one mouse. Horizontal bars represent the mean for the group. The infected groups had significantly more bacteria than the uninfected group. There were no statistical differences among the infected groups regardless of treatment.
We evaluated two topical drugs that could potentially be used for the treatment of ABRS. These drugs included dexamethasone and Ciprodex (a combination of dexameth-asone with ciprofloxacin). Because Ciprodex is approved as an effective treatment for patient with acute otitis media through tympanostomy tubes (AOMT) due to S pneumoniae, we did not include a ciprofloxacin-only arm. Our goal was to determine which treatment provided the best clearance of S pneumoniae and the greatest reduction in the associated inflammation in the sinuses.
The response to placebo treatment was typical for our model. 9 The bacterial counts were significantly increased; this increase was accompanied by a rise in inflammatory cells within the sinus mucosa. We have previously shown that the bacterial counts in nasal lavage correlate strongly with sinus tissue cultures. 14 We used lavage cultures in this study, because we cannot culture the sinus and perform flow cytometry on the same animals. We would also have expected that the topical antibiotics would have their most direct effect on the nasal cavity and the adenoids, areas that the nasal lavage samples well.
Our previous studies with oral antibiotics in this model demonstrated some degree of efficacy in the course of the infection. 15 The combination of ciprofloxacin/dexametha-sone suspension, which is effective in the treatment of AOMT, did not have a significant impact on the acute bacterial murine sinus infection. Ciprodex-treated mice had approximately the same numbers of bacteria in their lavages on the third and tenth days of treatment. Granulocytes were the only inflammatory cells that decreased significantly after Ciprodex treatment. Interestingly, in a previous study we performed using our model in which we used oral moxifloxacin—a quinolone similar to ciprofloxacin—we had to increase the frequency of dosing to four times a day to obtain a significant effect, even though the bacteria were exquisitely sensitive to the antibiotic in vitro. 16 A possible explanation may have been the extremely rapid metabolism of moxifloxacin by the mice. The rapid metabolism of ciprofloxacin, when applied locally, is also a possible explanation for our current results, although the route of administration differed in each of the two studies.
The reason that Ciprodex worked in the ear and not in this sinus model may be related to the dosing and fate of the drug. In ears with infection, there is no surface clearance of the drug, but there is rapid clearance in the nose, leading to a decrease in contact time between the drug and the mucosal membranes. Other possible reasons for the failure of topical antibiotics to work on ABRS in mice include the drugs' distribution in the nasopharynx and the nasal cavity. It is presumed that the bacteria enter the nose and are carried to the nasopharynx, where they colonize the adenoid tissue. Blowing and other mechanisms are thought to carry the bacteria into the sinuses, where they proliferate. It is possible that the drug did not reach the bacteria in the sinuses and that, after administration of the drug and its transit to the gastrointestinal tract, the bacteria from the sinuses repopulated the nasopharynx. The pharmacokinetics of the drug delivered topically in the nose is unknown. It is possible that mucociliary transport cleared the drug so rapidly that exposure of bacteria to the drug lasted less than 20 minutes. Thus, S pneumoniae, which replicates every 20 minutes, had the opportunity to increase 235 between treatments.
We observed that 3-and even 10 days—of treatment with topical dexamethasone did not result in an increase or decrease in the number of bacteria obtained by nasal lavage. Compared with placebo, however, dexamethasone-treated mice had equivalent numbers of granulocytes in their sinuses. Because dexamethasone is absorbed systemically from the nasal mucosa, we do not know whether any changes within the sinuses result from a systemic distribution of the drug or are secondary to local changes within the nose, which secondarily affected the sinuses.
A recent report by Desrosiers et al 17 demonstrated that treatment with a topical intranasal corticosteroid is associated with lower recovery rate of bacteria, mainly Staphylococcus aureus and coagulase-negative Staphylococcus species, from the ethmoid cavities in individuals undergoing surgery for chronic rhinosinusitis than those receiving no steroid treatment prior to surgery. In our study, intranasal dexamethasone had a slight beneficial effect on the reduction of inflammation without eradication of the bacterial infection. Importantly, this arm of the study showed that the bacterial infection did not worsen. The overall clinical implication, if this study in mice can be applied to humans, is that patients treated for allergic rhinitis with intranasal steroids do not need to stop using them if an acute bacterial sinus infection develops. However, although our animal model of acute sinusitis has great utility for studying the disease, the various differences between mice and humans must always be considered when extrapolating the results of animal tests to predict effects on humans.
Otolaryngologists have been using different forms of nasal irrigation with varying concentrations of antimicrobial agents including tobramycin, gentamicin, ciprofloxacin, povidone-iodine, and other antimicrobials compounded by their local pharmacies. 18 These agents have not been shown to be efficacious in treating acute or chronic rhinosinusitis. Various studies suggested a reduction in the number of recurrent episodes and in the severity of reported symptoms in these patients. 6,12 One study 7 that compared the efficacy of nebulized topical saline-tobramycin solution with saline-only solution in patients whose chronic rhinosinusitis was refractory to medical and surgical therapy showed that both solutions improved the symptomatology and objective parameters. Because addition of tobramycin provided a minimal benefit, the authors suggested that it was the effect of the saline solution lavage that had been useful by cleansing the sinus surfaces and reducing local concentrations of bacteria and their inflammatory toxins. It is also worth noting that most of the described studies have been performed in postoperative patients, and that the likelihood of success of topical treatments in nonoperated patients is probably even smaller because of the lack of penetration of the agent into the sinus cavities.
CONCLUSION
We analyzed the effect of two topical medications on acute rhinosinusitis. We found that neither dexamethasone nor a combination of ciprofloxacin and dexamethasone had any effect on the clearance of bacteria in our model of acute bacterial sinusitis. The lack of topical, intranasal efficacy of ciprofloxacin and dexamethasone at the dosages used in this study (150 μg and 50 μg per nostril, twice daily, respectively), delivered in the form of drops, could be attributed to subpotent dosage, rapid nasal clearance, or inability of the drops to reach the site of infection in the sinuses. Topical dexamethasone alone did not significantly alter the course of the bacterial infection.
AUTHOR INFORMATION
From the Department of Surgery, Section of Otolaryngology—Head and Neck Surgery (Drs Sahin-Yilmaz, Baroody, and Naclerio) and the Department of Pathology, (Dr Thompson), The University of Chicago; and Alcon Research, Ltd (Dr Wall), Fort Worth.
Corresponding author: Robert M. Naclerio, MD, Professor and Chief, Section of Otolaryngology—Head and Neck Surgery, The University of Chicago, 5841 S Maryland Ave, MC 1035, Chicago, IL 60637.
E-mail address:
AUTHOR CONTRIBUTIONS
FINANCIAL DISCLOSURE
This paper was partly supported by a grant from Alcon and by the McHugh Otolaryngology Research Fund.