
Abstract

Since the 1980s there has been considerable interest in stereotactic radiosurgery and other forms of focused radiation therapy for nonmalignant conditions. One of the concerns raised by radiation treatments for acoustic neuroma, which has somewhat limited their use, is the potential for radiation to induce other intracranial tumors, including malignancies. 3 , 4 Because such cases are rare, it has been difficult to establish a reliable estimate of their occurrence to guide selection of treatment and patient counseling. We report a case that we feel should be taken into consideration when estimating the risk of radiation-induced malignancy. Institutional Review Board approval was obtained.
A 58-year-old woman presented to the emergency department complaining of increasing ataxia for the past two weeks. She also noted numbness and tingling in the right face and body, diplopia, blurred vision, nausea, and vomiting for the same period. On the morning of admission she experienced a severe pressure headache at the right mastoid process, which spread to include the left side within a few hours. The past medical history was significant for microsurgical excision of a right acoustic neuroma two years previously. This was conducted as a two-stage procedure at another center. A few months postoperatively she received an osseointegrated implant for single-sided deafness. The patient's family history was negative for cancer, schwannoma, and neurofibromatosis types I and II. On examination she avoided head movement. There was brisk spontaneous right-beating nystagmus with eyes open. Right facial numbness was reported. There was also decreased light-touch sensation on the left extremities and torso. The deep tendon reflexes were 2+ and strength was 5/5 throughout. The general physical and neurologic examinations were otherwise unremarkable.
Magnetic resonance imaging (MRI) (Fig 1) showed a lobular, infiltrating mass with necrotic centers involving the right tegmentum, midbrain, pons, middle cerebellar peduncle, and cerebellum. The enhancing area in the right posterolateral cerebellar hemisphere measured 2.5 cm in largest diameter. The lesion was accompanied by significant edema, evident on T2-weighted MR sequences, though there was no evidence of hydrocephalus. A stereotactic biopsy performed the morning after admission was suggestive of glioma. Stereotactic maximum safe resection of the tumor in the right cerebellum and brain stem was carried out. Postoperatively there were no new neurologic deficits. Numbness of the right face and left body persisted, and the diplopia resolved. Examination of permanent histologic sections revealed WHO grade 4 glioblastoma multiforme (Fig 2). Many tumor cells showed strong immunoreactivity to glial fibrillary acidic protein and epidermal growth factor. Ki67 labeled 10% to 15% of cells in most regions of the tumor. Many cells were immunoreactive for p53 and bel-2.
Discussion
Most authors point out that the occurrence of a second tumor following radiation does not prove a causal relationship; however, the citation of the “Cahan criteria” and the publication of a case generally does imply causation. It is well recognized that radiation damages DNA and is tumorigenic and carcinogenic. There is no such suspicion regarding microsurgery. The occurrence of glioblastoma adjacent to the site of microsurgical resection of an acoustic neuroma points out the hazard of assuming that there is a causal relationship when two events are associated, ie, that radiation was the cause of all tumors observed following radiation. It would be desirable if more secure criteria, such as molecular markers, were available to differentiate spontaneous versus radiation-induced tumors. Although deletions in chromosome 10 have been found in both benign and higher-grade meningiomas and intracranial malignancies associated with radiotherapy, definitive markers that differentiate spontaneous from radiation-induced tumors have yet to be identified. 4 , 5
Author Information

Axial T1 post-gadolinium MRI two years after surgical removal of acoustic neuroma, demonstrating a 2.5-cm enhancing right posterolateral cerebellar lesion suggestive of glioblastoma.
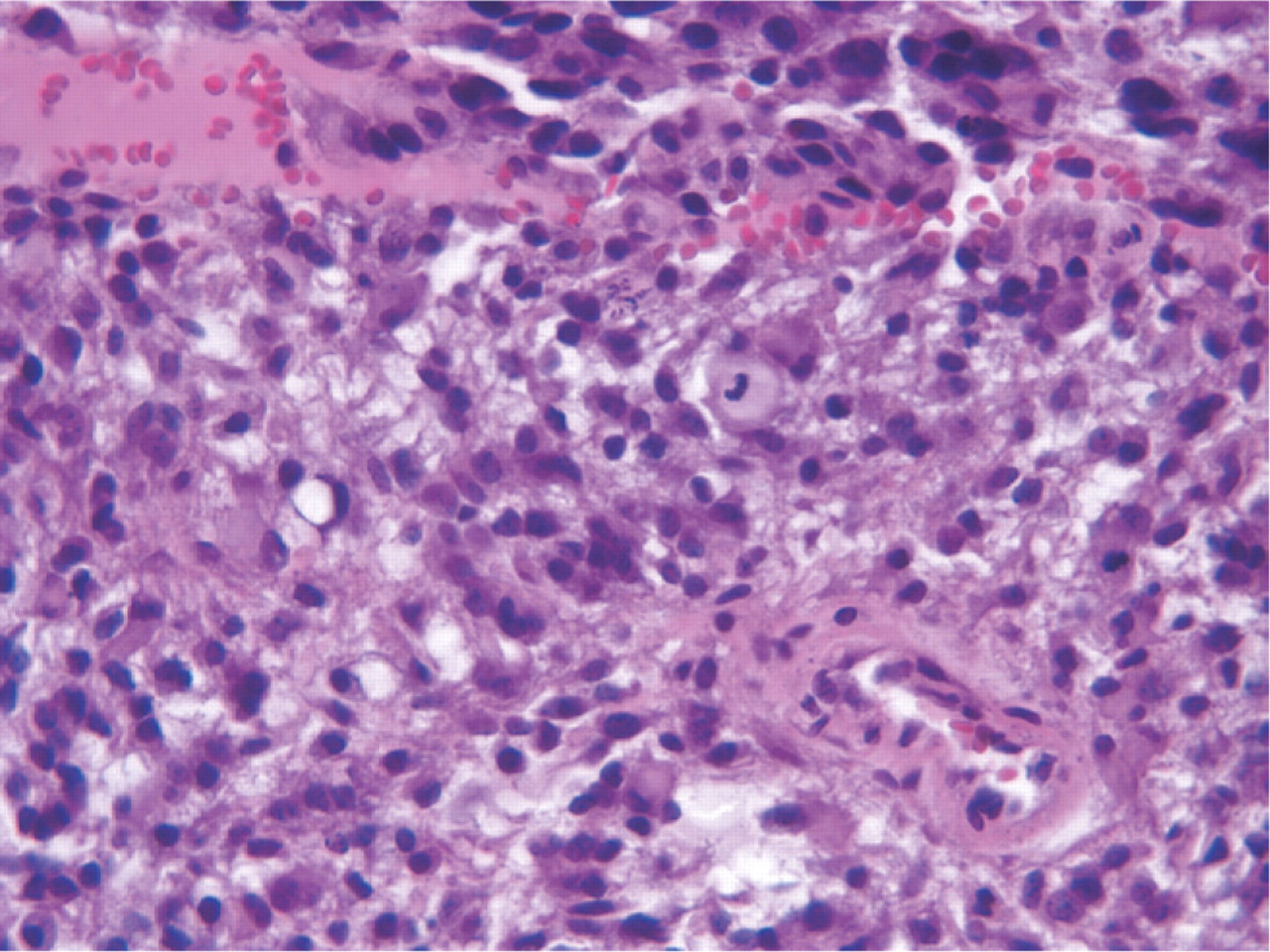
Histopathology of the lesion on hematoxylin and eosin staining of permanent histologic sections showing an infiltrative glial neoplasm composed of poorly differentiated fibrillated and small cells. The cells contain either irregular or rounded nuclei, many showing considerable nuclear atypia and atypical mitotic figures. There is microvascular proliferation with fibrin thrombi present in scattered vessels. Small areas of microcystic degeneration are noted as well as foci of connective tissue proliferation. The tumor engulfed the VIIIth nerve. The VIIIth nerve was sectioned and did not appear to be the origin of the tumor.
Author Contributions
Financial Disclosure
None.