
Abstract
Objective
To determine the diagnostic accuracy of specimens obtained by a surgeon performing office-based ultrasound (US)-guided fine-needle aspiration biopsy (FNAB) of thyroid nodules.
Subjects and Methods
From 2003 to 2006, a single surgeon performed 447 consecutive office-based US-guided FNABs without on-site cytological specimen evaluation. Adequate specimens had at least six clusters of follicular cells from at least two separate needle passes.
Results
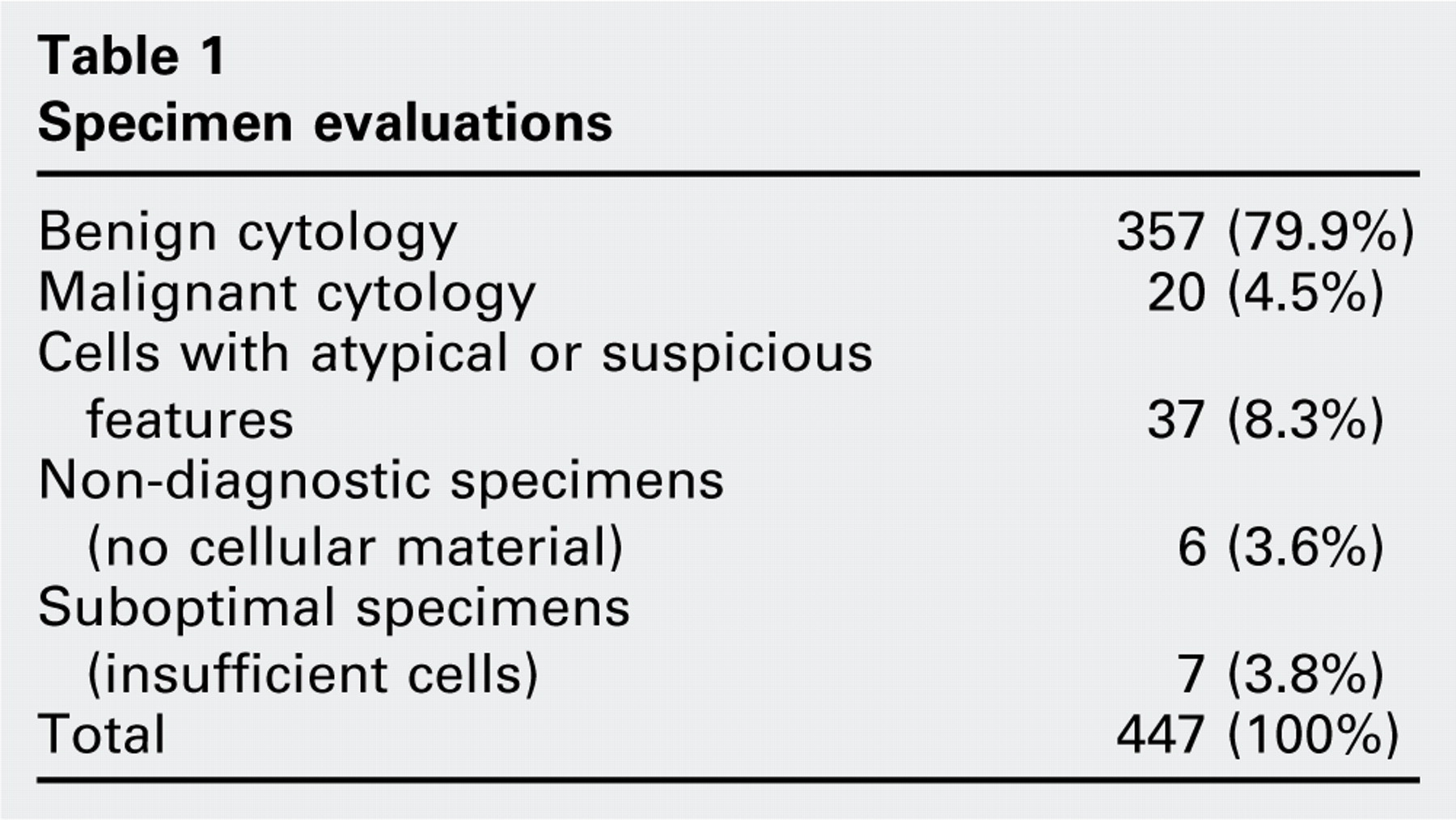
Non-diagnostic specimens occurred in 16 of 447 (3.6%) nodules, whereas suboptimal specimens occurred in 17 of 447 (3.8%). Adequate samples were obtained in 413 of 447 (92.6%) of specimens. Malignancy was present in 20 of 447 (4.5%) and atypical features were present in 37 of 447 (8.3%). Benign diagnoses were rendered in 357 of 447 (79.9%) of specimens, of which four of 357 (1.1%) represented false-negative results.
Conclusion
Prior publications recommend that obtaining adequate thyroid cytology specimens requires use of US-guided FNAB and on-site evaluation of cytology adequacy. This study demonstrates that a combination of experienced US guidance, both capillary and aspiration sampling, and three to four needle passes produce comparable results while conserving costs and resources.
The introduction of ultrasound (US) guidance has reduced the number of inadequate samples by half. Carmeci and associates 2 demonstrated a decrease in the non-diagnostic rate from 16 to 7 percent with the use of US-guidance, while Danese and colleagues 3 reported a similar decrease from 8.7 to 3.5 percent. US also significantly increased the sensitivity, specificity, and diagnostic accuracy of FNAB, while reducing the occurrence of false-negative results. 2 – 5 Consequently, US has become essential in improving the overall yield of thyroid FNABs.
To further improve the yield of FNAB specimens, some authors strongly advocate immediate on-site assessment of the specimen by experienced cytopathologists. 4 , 6 , 7 Several arguments are raised to support their position. Besides assessing the sample's adequacy, a clinician may render a preliminary diagnosis and determine the need for ancillary studies, thus avoiding treatment delays. Furthermore, repeat examinations, which result in higher costs and increased patient inconvenience and discomfort, are obviated. 4 , 6 , 7
Several single-armed, non-controlled, retrospective studies demonstrate FNAB inadequacy rates that decrease to 4 to 9.5 percent when US-guided FNAB is coupled with on-site cytological evaluation. 4 , 6 – 8 Despite design flaws in their studies, many of these authors conclude that immediate on-site adequacy assessment by an experienced cyto-pathologist is a requisite measure to produce the best yield.
However, experience in both ultrasonography and FNAB technique also contributes significantly to successful biopsy adequacy. 9 , 10 The head and neck endocrine surgeon who performs routine office-based ultrasound examinations and frequent FNABs possesses this unique combination of skills. His or her expertise may improve FNAB sample yield, as suggested by some authors, and obviate the increased cost and procedure time associated with on-site assessment of specimen adequacy. 9 – 10 This prospective cohort study aims to determine the diagnostic adequacy of cytology specimens obtained specifically by a surgeon performing office-based US-guided FNAB of thyroid nodules without immediate cytological assessment.
Subjects and Methods
After obtaining approval from an institutional review board, the authors prospectively enrolled consecutive subjects from 2003 to 2006. The senior author (D.L.S.) performed all US examinations and FNABs in a tertiary care, university-based practice. All consult cases with biopsies performed elsewhere were excluded.
All subjects had a comprehensive ultrasonographic examination of the neck, which included the central, lateral, posterior, and submandibular compartments. A linear array transducer (SonoSite TITAN [5-10 mHz] or Micromaxx [7-12 mHz]; SonoSite, Inc, Bothell, WA) was used to image the neck in both the transverse/axial and longitudinal/sagittal planes. Photographs were obtained for documentation. When multiple nodules were present, the largest and any sonographically suspicious (irregular borders, microcalcifications, peripheral vascularity) nodules were biopsied. Along with demographic information, the ultrasound results, total number of passes, and cytology results were recorded.
Procedure
The patient is positioned supine with the neck in extension. A pillow placed under the shoulders may help support some patients. Once the lesion in question is sonographically localized, the overlying skin is cleaned with alcohol and infiltrated subcutaneously with lidocaine 1 percent with epinephrine (1:100,000) with a 25-gauge needle. The needle is next advanced in the direction of the probe's long axis (longitudinal view), and the solution is deposited beneath the strap muscles, along the anticipated biopsy needle tract. With ultrasound guidance, the depth of the lesion as well as its proximity to the great vessels and the airway are all estimated, and the angle of needle insertion is determined.
Next a 22-gauge, 1.5-inch needle is inserted next to the mid-portion of the long axis of the transducer at a 45-degree angle to the skin. This technique allows visualization of the entire needle tract and confirms its entry into the nodule (Fig 1). Keeping the bevel of the needle facing upward towards the transducer enhances visualization of the needle tip, which is critical to minimize sample error. The authors prefer to obtain the first sample via the capillary technique, unless the nodule is cystic. The needle is agitated with multiple excursions across the center of the mass on its first pass. With this back-and-forth motion, the free needle edge shaves cells from within the mass. Microcores of the specimen can be additionally shaved by rotating the needle within the specimen. Holding the needle steady in place allows for maximal capillary action prior to withdrawal. The material is then deposited on a glass slide and smeared with another slide. Immediate fixation is integral to avoid desiccation artifact.
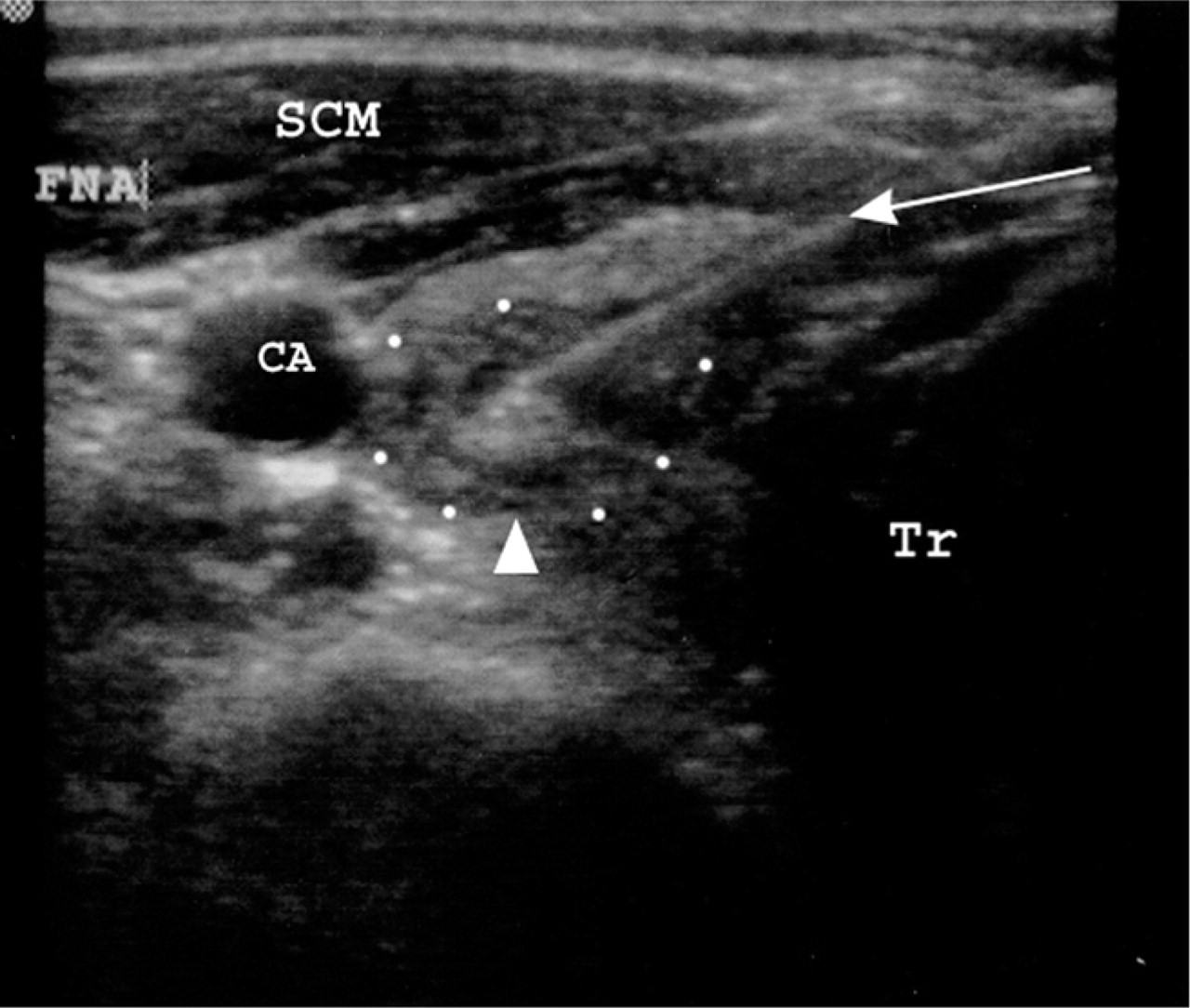
Axial ultrasound of right superior thyroid lobe during fine-needle aspiration biopsy of a nodule with microcalcifications (arrowhead). The needle's (arrow) entire tract is visible on sonog-raphy during the biopsy. Tr, trachea; CA, carotid artery; SCM, sternocleidomastoid muscle; FNA, fine-needle aspiration.
For subsequent passes, the suction aspiration technique is used. A 3-mL syringe with 1 mL of air is attached to the needle. Once the needle is sonographically confirmed to be within the lesion, 2 ml of negative pressure is applied to the syringe and several back-and-forth excursions of the needle again shave cells from within the lesion. Prior to removing the needle, the negative pressure is released. The aspirate is placed in a solution of CytoLyt fixative solution (Cytyc Corp, Boxbourough, MA). This process is repeated until a total of three to four passes are performed, each with a separate needle and fixative container.
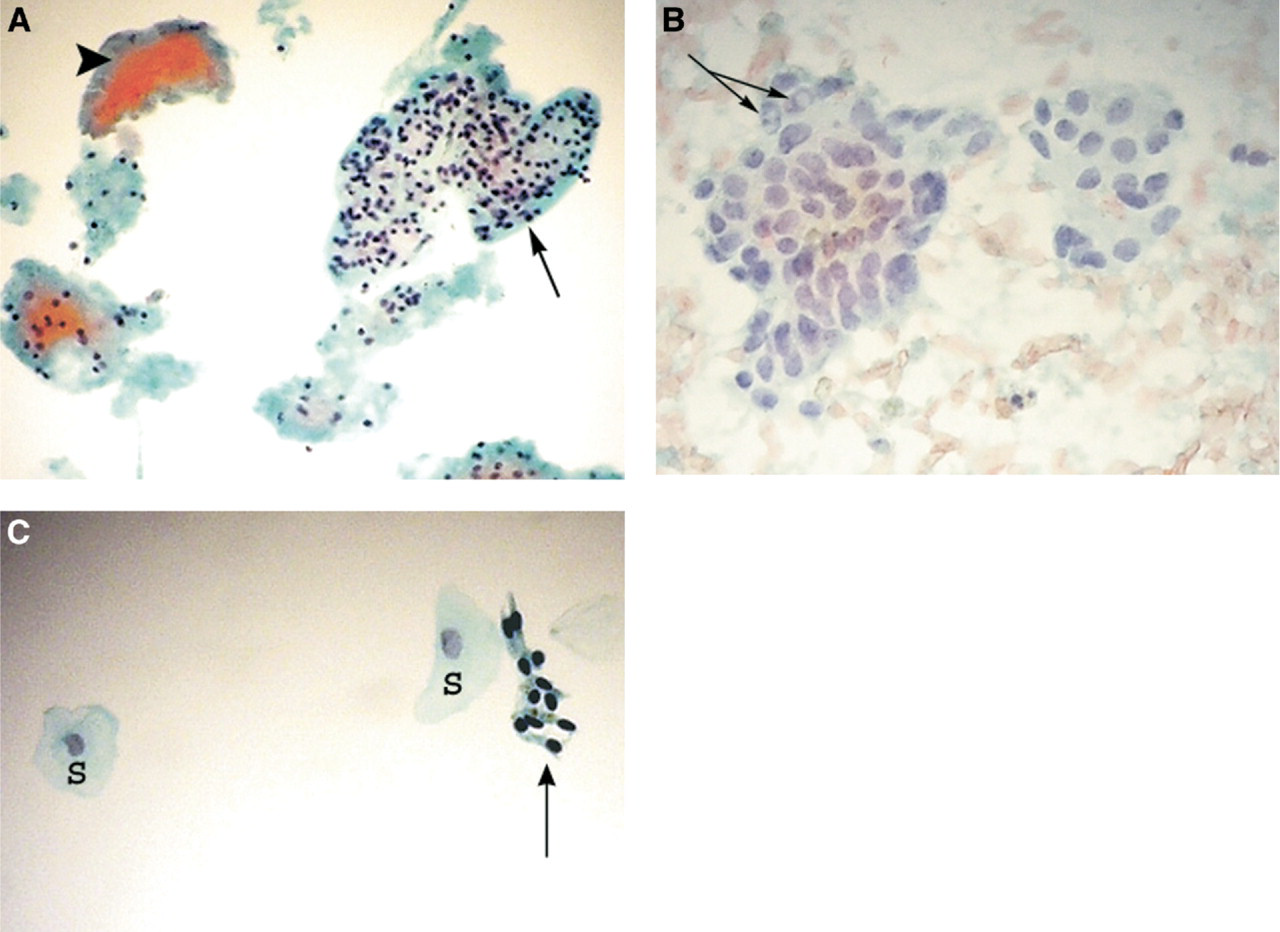
The specimens are then examined in the cytology lab over the subsequent days. An adequate specimen is defined as having at least six clusters of thyroid follicular cells (15-20 cells) for each specimen, from at least two separate needle passes (Fig 2A and B). Specimens producing no follicular cells are deemed non-diagnostic, and those with insufficient follicular cells (Fig 2C) are considered suboptimal. Both non-diagnostic and suboptimal samples are designated “inadequate” because neither produce a definitive diagnosis.
(
Results
A total of 447 US-guided FNABs were performed on 400 patients enrolled in the study. Women comprised 360 (90%) of the cases.
Non-diagnostic specimens occurred in 16 of 447 (3.6%) cases, whereas suboptimal specimens occurred in 17 of 447 (3.8%). The majority of the suboptimal and non-diagnostic specimens occurred in hemorrhagic cystic nodules, with specimens predominately containing hemosiderin-laden macrophages. Because both non-diagnostic and suboptimal specimens were considered insufficient, the sample inadequacy rate for this study was 7.4 percent. Adequate follicular specimens were obtained in 413 of 447 (92.6%) of specimens.
A malignant cytological diagnosis was rendered in 20 of 447 (4.5%) and atypical or suspicious features were present in 37 of 447 (8.3%) specimens. Benign cytological diagnosis was rendered in 357 of 447 (79.9%) specimens (Table 1). Of these patients, four of 357 (1.1%) had a false-negative cytology result. The FNAB procedure was well tolerated by all patients.
Specimen evaluations
There was one (0.2%) complication of a post-procedure hematoma in a patient with an underlying coagulopathy despite pretreatment with intravenous clotting factors. This hematoma was self-limited and spontaneously resolved.
Discussion
Recent studies that have attempted to quantify the benefit of immediate assessment of cytological adequacy have produced conflicting results. 4 , 6 – 9 , 11 , 12 Proponents claim that, along with a lower non-diagnostic specimen rate, enhanced patient convenience and comfort, cost savings, and expeditious results are some advantages of immediate adequacy assessment. 4 , 6 , 7 , 11 Others counter that if an FNAB is performed under US guidance, immediate cytological evaluation only prolongs procedure time, increases patient discomfort, and consumes valuable pathology and radiology resources, without any significant increase in the diagnostic yield. 9 , 12
Five studies evaluating the value of on-site adequacy assessment of US-guided FNAB report non-diagnostic sample rates ranging from 4 to 9.5 percent. 4 , 6 , 7 – 9 Although they show modest improvement with the addition of on-site assessment, the inadequacy rate of 7.4 percent demonstrated in this study clearly falls within their parameters. A surgeon's radiographic and biopsy skills, if expert, result in specimen yields similar to those of on-site assessment.
A study by Ghofrani and colleagues 9 strongly supports this concept. Their study failed to demonstrate a statistically significant difference between the non-diagnostic rate of 4.5 percent (with on-site assessment) and 7.1 percent (without on-site assessment) for US-guided FNABs. Moreover, when the US-guided FNABs were divided into two groups on the basis of radiologist experience, the non-diagnostic sampling rate showed a statistically significant decrease from 8.2 percent to 5.4 percent when inexperienced radiologists were compared with those with substantial expertise. The head and neck endocrine surgeon who performs routine office-based ultrasound is facile with sonographic and FNAB techniques and is most definitely such an expert.
Furthermore, the addition of immediate cytological assessment substantially extends the total duration of the procedure. O'Malley and colleagues 12 showed a significant increase in procedure time from 12.5 to 44.4 minutes without a concomitant improvement in cytological adequacy. The addition of on-site assessment in the setting of office-based US-guided FNAB would likely consume resources without a significant improvement in diagnostic yield.
The health care costs imparted by immediate on-site cytological assessment should also be considered carefully. A controlled, two-arm study by Eedes and coworkers 8 demonstrates a statistically significant decrease in their non-diagnostic rate of FNAB from 14.9 percent to 9.5 percent with the use of on-site adequacy assessment. However, this modest improvement was achieved at a cost of 220 minutes of cytologists' time for every specimen for which on-site assessment proved useful. In another study by Ceresini and colleagues, 13 on-site assessment improved diagnostic yield in only 6.7 percent of specimens. Therefore, 15 specimens underwent unnecessary analysis for every one specimen improved. Although the present study does not specifically investigate these economical implications, the costs of this additional expended time are considerable. The authors of this study agree with Eedes and colleagues 8 that it may be most cost-effective to obtain on-site adequacy assessment only under special circumstances such as large cystic masses, multiple large nodules, or repeat procedures.
Regardless of whether on-site evaluations are performed, complications of thyroid FNAB, such as hematoma or infection, are quite rare. One (0.2%) high-risk patient in our cohort experienced a self-limited post-procedure hematoma. This rate is well within published standards. 14
Furthermore, although both capillary sampling and aspiration techniques are widely described, an individual who is familiar with and frequently employs them must perform these procedures meticulously. The specific method of sampling in this study is not solely accountable for our data, but it is possible that the routine use of three to four passes, instead of the minimum two, may result in an improved yield. The authors also strongly believe that the integral combination of both a highly proficient ultrasonographer with a biopsy technique perfected with specific training and practice is necessary to obviate on-site cytological evaluation. The head and neck endocrine surgeon who performs routine office-based ultrasound examinations and frequent US-guided FNABs indeed possesses this unique skill set.
Conclusion
Through a prospective cohort, our study demonstrates that adequate specimens can be obtained by surgeons who perform office-based US-guided FNAB with multiple needle passes performed by a combination of capillary sampling and aspiration techniques. However, expertise in US, meticulous FNAB technique, and open communication with the interpreting cytopathologist are all critical in optimizing the diagnostic utility of this method.
Author Contributions
Financial Disclosure