
Abstract
Human temporal bone experiments have assessed the acoustic effect of prostheses used in ossiculoplasty. 8 , 9 To our knowledge, reconstructed middle ear transmission with and without the malleus has not been assessed. Therefore, these experiments were performed to evaluate the acoustic role of the malleus on middle ear reconstruction using human cadaveric temporal bones.
Materials and Methods
Sixteen fresh human temporal bones, consisting of males ranging from 61 to 87 years with a mean age of 72.1 years, were extracted from human cadavers within 48 hours of death using a Schuknecht bone saw at the time of autopsy. The cored specimens were wrapped in gauze, placed in a 1:10,000 solution of Merthiolate in normal saline, and stored at 5†C. All measurements were performed within six days of death. For each temporal bone, the tympanic membrane (TM) and middle ear were inspected under an operating microscope to ensure that the ear appeared normal. Bones with an abnormal TM or middle ear were not used. Due to its nature, this study did not require Institutional Review Board approval.
Following removal of any attached connective tissue, the anterior bony wall of the external auditory canal was drilled down to a 2-mm rim, leaving the annulus intact. A simple mastoidectomy and posterior hypotympanotomy were performed and part of the vertical and the horizontal segment of the facial nerve was removed to allow a good view of the stapes footplate through the facial recess. A plastic tube (8.5 mm internal diameter, 25 mm length) was fixed around the bony ear canal using clay so that the axis of the tube was perpendicular to the TM. The tube contained an earphone adapter on the side near the lateral end with a probe tube opening 2 mm from the medial end. An opening in the mastoid cortex was performed for the insertion of prostheses and stapes displacement measurements. The remainder of the temporal bone was embedded in Hydrock dental cement (Kerr, Romulus, MI), creating a solid specimen block. Reflective microbead targets were placed on the center of the stapes footplate. The opening in the mastoid cavity was then sealed by building up the sides with modeling clay and placing a glass cover slip on top. The bone was then secured in a temporal bone holder.
Measurements were taken using the SYSid 6.5 audio band measurement and analysis system (Ariel Co., Berkeley, CA). With a DSP-16+ processing board, this software program produces an output signal used to drive the sound source, and synchronously measures and averages the magnitude and phase angle of two input signals at each frequency using fast Fourier transformation. The sound stimulus consisted of stepped tones swept at 100 logarithmically spaced frequency points from 0.1 to 10 kHz. For each input frequency, a 4096-point response signal was averaged 15 times.
Sound was presented at the side of the lateral end of the plastic tube using a #2955 Knowles hearing aid receiver (www.knowles.com). The open end was closed with a thin glass cover slip held in place with petroleum jelly. The sound pressure in the plastic tube was measured within 3 mm of the TM using an ER-7C microphone (Etymotic Research, Elk Grove Village, IL) attached to a probe tube inserted through an opening in the plastic tube. The sound signal was amplified by a D-75 power amplifier (Crown, Elkhart, IN) and fed through a 200-ohm resistor to the earphone that gave each tone an intensity ranging from 80 to 120 dB Sound Pressure Level (SPL). The results were calculated relative to an input of 80 dB SPL at the TM.
The stapes footplate velocity was measured using a laser Doppler vibrometer (LDV; HLV-1000; Polytec, PI, Costa Mesa, CA). The LDV sensor head was connected to a joystick-operated HLV-MM2 micromanipulator, which was mounted over the lens of an operating microscope and allowed the beam of a helium-neon laser to be directed onto one of the reflective targets at the center of the stapes footplate. The velocity of the stapes footplate was divided by the cosine of 55 degrees to correct the measured velocity for the angle of measurement (55 degrees). Velocity was converted to peak-to-peak displacement in nanometers (nm) for comparison purposes. All displacement measurements of the stapes footplate were performed twice and averaged. Phase measurements were also obtained using the SYSid analysis system but are not included.
The probe tube microphone and LDV magnitude and phase calibration procedures have been described previously. 10
Effect of the Malleus
After baseline measurements of stapes displacement in eight intact temporal bones, the incus was removed carefully via the facial recess. The incus was then shaped to function as a replacement prosthesis. After the long process of the incus was removed, a small depression was created in the end of the short process with a cutting burr to receive the stapes head and the length adjusted to fit snugly between the mid malleus handle and stapes head. The sculpted incus then was placed between the mid malleus handle and stapes head, and the measurement was repeated (Fig 1). The periosteum of the manubrium was then incised longitudinally with a very sharp angled lancet knife. The TM, together with the periosteum, was detached from the manubrium, the suspensory ligaments and tensor tympani tendon cut, and the malleus removed carefully via the facial recess. Great care was used to separate the malleus umbo from the TM without producing a perforation. Another banked incus was sculpted to snugly fit the new, longer distance between the TM and stapes head, and was placed between the same site on the TM and stapes head. This incus prosthesis was always slightly longer than the prosthesis used when the malleus was present. The goal was to make the tension the same for both conditions. The displacement of the stapes footplate center was again measured, and the baseline and two test conditions were compared.
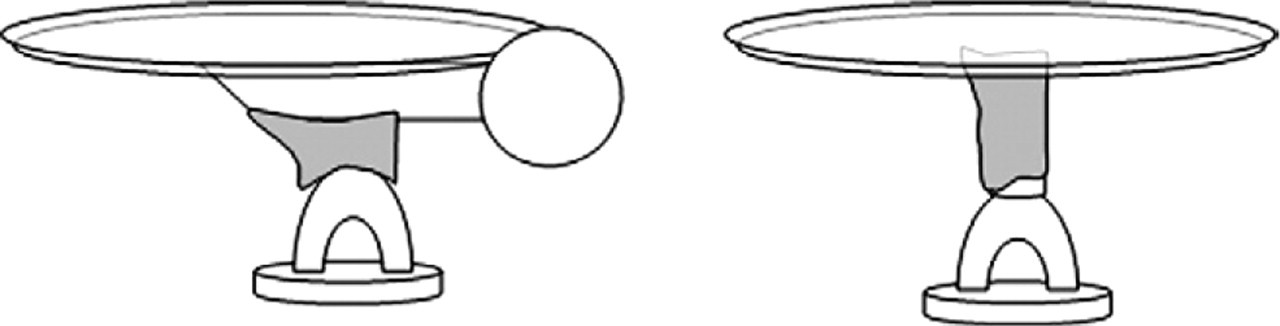
Schema of reconstruction of the ossicular chain with malleus present
Influence of Cartilage Insertion
Eight temporal bones were used in this study. A piece of cartilage was harvested from the external ear canal and stored in 70% alcohol at 5†C. The cartilage was trimmed to a thickness of 0.5 to 0.7 mm and three different diameters of cartilage (2 × 4, 4 × 6, and 6 × 7 mm) were used to evaluate the influence of interposed cartilage in reconstruction without a malleus. After the malleus was removed, one of the three cartilage disks was inserted in random order between the TM and sculpted incus. The stapes footplate displacement was measured after placing each cartilage and compared to the baseline intact middle ear measurement (Fig 2). In order to maintain the same tension, the incus prostheses in these experiments were shortened, usually around 0.5 mm.
Results
Effect of the Malleus
Figure 3 shows the mean displacement of the center of the stapes footplate for the eight specimens relative to the ear canal pressure. The displacement was calculated for an ear canal pressure of 80 dB SPL in front of the TM. The mean curves of the baseline stapes displacement were in agreement with previous studies. 8 , 11 The mean change in dB of stapes displacement after reconstruction with and without a malleus, compared to the intact middle ear, is shown in Figure 4. Below 0.6 kHz, the gain after reconstruction with and without the malleus was nearly identical. The gain for reconstruction with the malleus in place was slightly better than without in the 0.6-kHz to 3.0-kHz range but never exceeded a 7-dB difference. The malleus present condition results tended to be worse above 4.5 kHz compared to reconstruction without the malleus; however, there were no significant differences at any test frequency. Table 1 shows the results of a Student t test of stapes footplate displacement at eight representative frequencies.
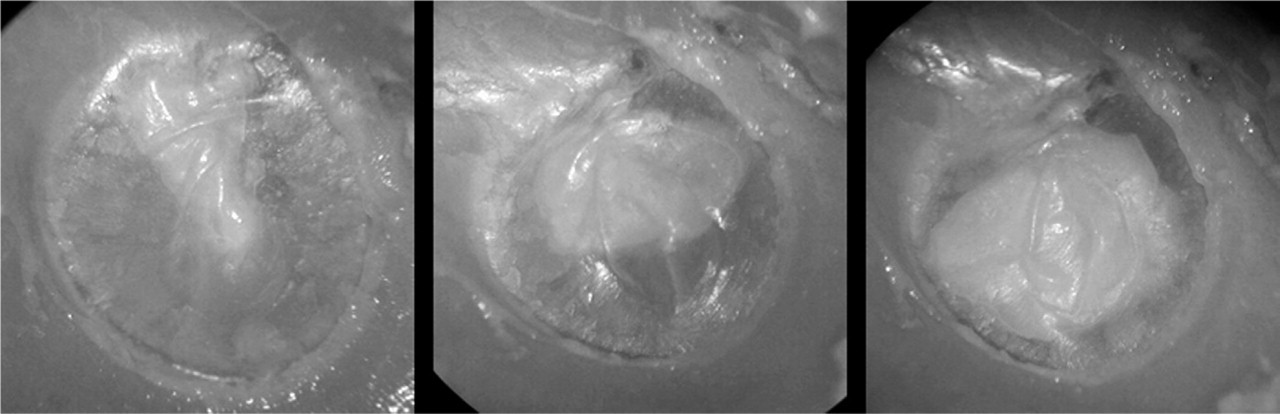
Photographs of reconstruction with cartilage insertion after malleus removal.
Influence of Cartilage Insertion
Figure 5 shows the mean change in stapes displacement in dB compared to the baseline normal ear (0 dB) for reconstruction when three different cartilage sizes were inserted between the TM and the sculpted incus. Table 2 shows the results of statistical analysis between the different conditions at eight representative frequencies. Below 1.0 kHz, the medium-diameter cartilage produced the best result and the large-diameter cartilage the worst, with the small-diameter cartilage in between. No significant differences were found between the small-diameter and medium-diameter cartilage at any test frequency. There was a significant difference in small-diameter cartilage versus large-diameter cartilage and medium-diameter cartilage versus large-diameter cartilage at 0.25 kHz and 0.5 kHz (P < 0.05). At 1.0 to 2.0 kHz, the difference in stapes displacement with the three cartilage diameters was small, but in the 2.0-kHz to 10.0-kHz range, the large-diameter cartilage was better than the small- and medium-diameter cartilages. There was a significant difference in medium-diameter cartilage versus large-diameter cartilage at 3.0 kHz and 4.0 kHz (P < 0.05), with near-significant differences at higher frequencies. Near-significant differences between the small-diameter cartilage and large-diameter cartilage inserts were present at 3.0 and 4.0 kHz and above.
Discussion
These experiments were performed to determine whether a significant difference exists in reconstructed middle ear transmission with or without a malleus using a human temporal bone model. In this study, reconstruction with a malleus present showed no significant difference compared to reconstruction without a malleus (Figs 3 and 4, Table 1). Goode et al 12 reported that the best theoretical location on the malleus for a prosthesis was as close to the umbo as possible while maintaining minimal prosthesis angulation. This site has the largest displacement for a given SPL at the TM. In these experiments, the sculpted incus was placed between the stapes and mid manubrium in order that angulation of the prosthesis would not exceed 30 degrees.
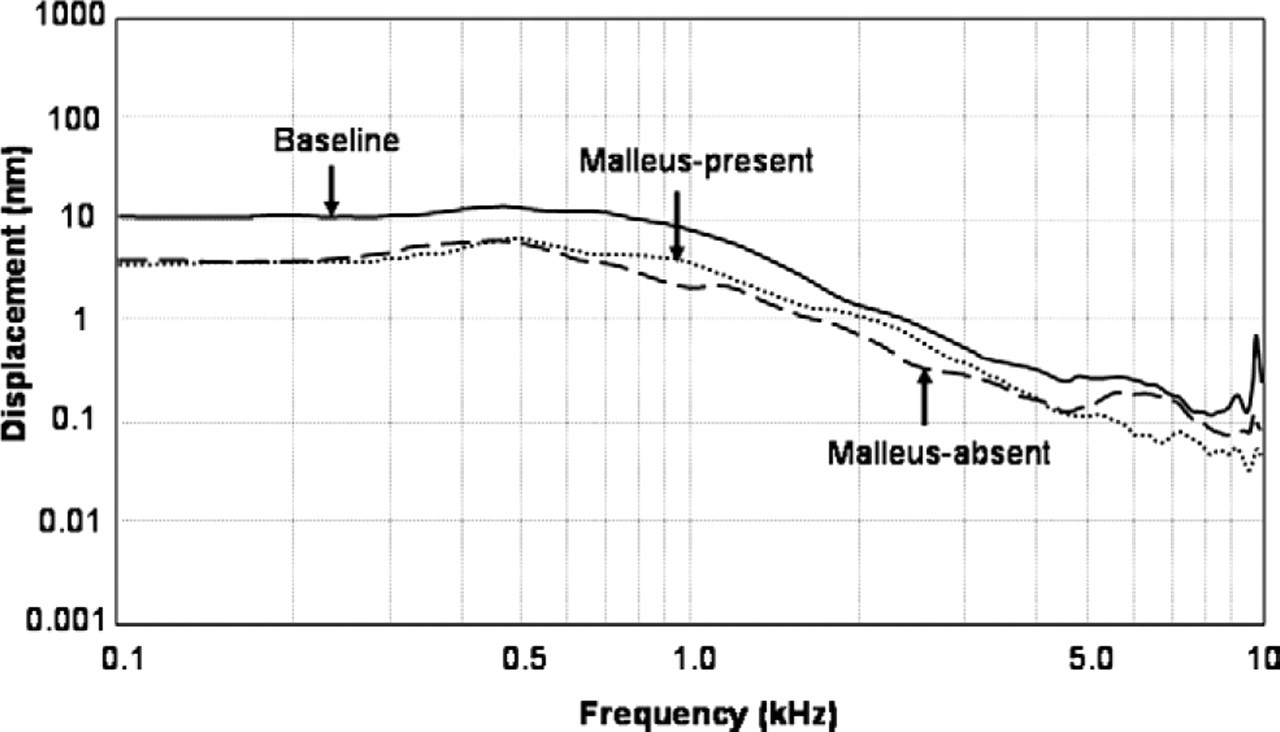
Mean displacement in nanometers of the center of the stapes footplate for eight specimens.
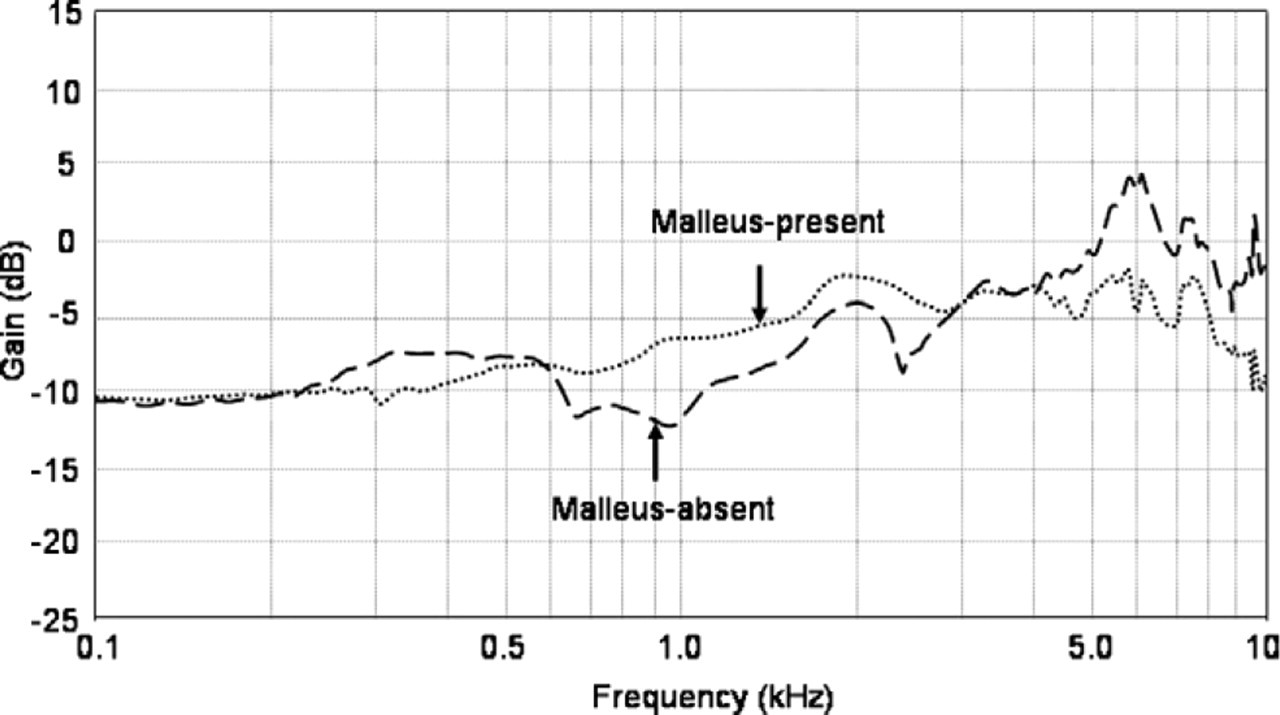
Mean change in decibels in stapes displacement for the malleus-present and malleus-absent reconstruction.
Mean change (dB) in stapes displacement at eight representative frequencies for reconstruction with and without malleus, compared with intact middle ear
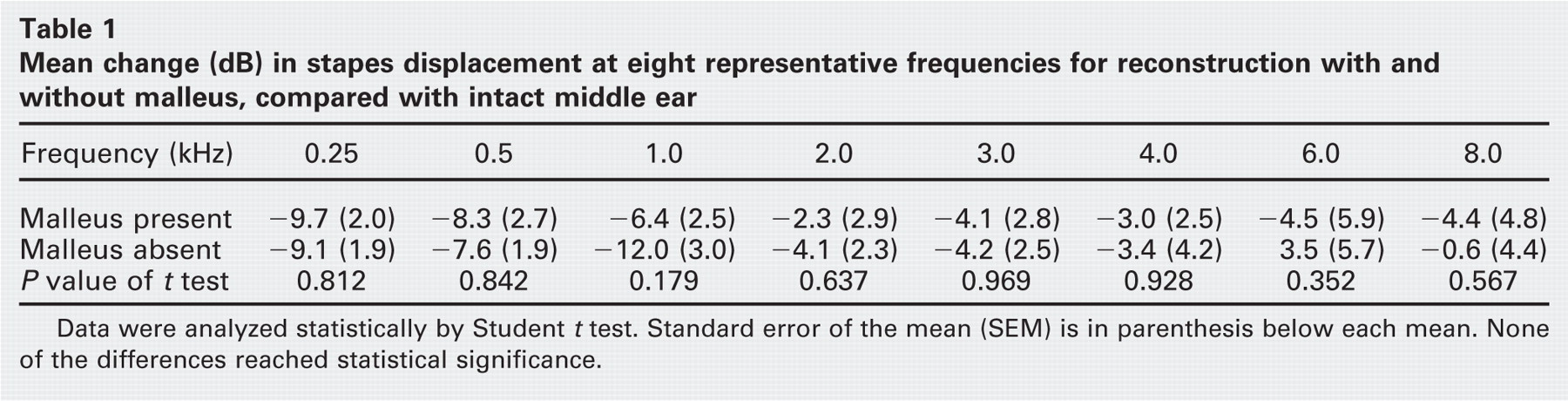
Data were analyzed statistically by Student t test. Standard error of the mean (SEM) is in parenthesis below each mean. None of the differences reached statistical significance.
The absence of the malleus makes the TM flat instead of conical. Bance et al 9 reported that a prosthesis connection from the malleus to stapes head performed better than a TM to stapes head. They speculated that the results were associated with the catenary principle of the TM, which is based on the curvature of the TM. However, this theory is controversial.
In cases of severe TM retraction or cholesteatoma, a piece of cartilage has been successfully used to reinforce the TM as well as decrease late extrusion of prostheses contacting the TM. Recently, reports on reconstruction of the TM reinforcing the entire TM with a cartilage graft have been published. 7 , 13 The diameter of the cartilage may affect sound transmission to the stapes when the malleus is absent. Mürbe et al 14 reported that a 4-mm-diameter cartilage graft gave better acoustic transfer characteristics than a 7-mm-diameter graft at 1.0 to 4.0 kHz in an auditory canal-TM model. Morris et al 15 found that smaller cartilage grafts between the tympanic membrane and an ossicular replacement prosthesis provided improved performance at lower frequencies compared to larger grafts. In clinical practice, however, some authors have reported results to the contrary, suggesting hearing results after tympanoplasty with large-diameter cartilage to be no different than those for fascia. 7 , 13 We assessed the effect of three different diameters of cartilage inserted between the TM and sculpted incus after removing the malleus in the human temporal bone model. As shown in Figure 5, the medium-diameter cartilage produced the best result below 1.0 kHz. Interposing cartilage with a larger diameter improved the high-frequency response the most at the expense of the low-frequency response. This improvement at higher frequencies would appear to be due to a stiffening effect on the TM produced by the larger-diameter cartilage. Zahnert et al 16 reported on the role of the prosthesis head diameter in the reconstructed middle ear using three different head size gold prostheses. Their results were similar to those of our cartilage diameter experiments and those of Morris et al. 15 They found that a reduction in the prosthesis head diameter resulted in a middle ear sound transfer loss at higher frequencies.
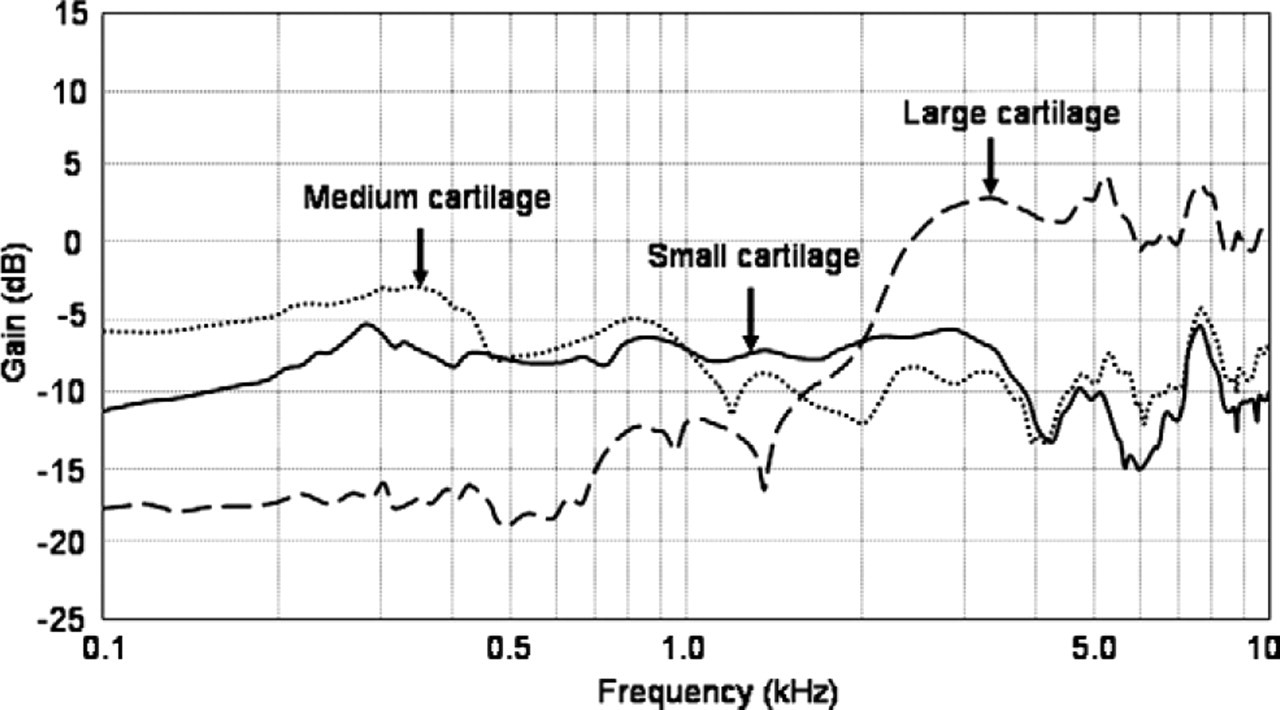
Mean change in decibels in stapes displacement with three different size cartilage grafts.
Cartilage thickness may also influence the sound transmission to the stapes. Zahnert et al 17 recommended cartilage grafts 0.5 mm thick because they are similar to the tympanic membrane in their acoustic properties. We used 0.5- to 0.7-mm-thick cartilage grafts in our study from this point of view. The mass of the cartilage inserts would be slightly different and might have some effect; the mass was not measured in these cartilage experiments.
While the fresh human temporal bone model used in these experiments appears to be the best available laboratory method to study the acoustic effect of different middle ear prostheses as well as other middle ear modifications, such as removing the malleus, it does have limitations. Controlling the prosthesis tension, an important variable, 18 from temporal bone to temporal bone is difficult, since the tension is determined by the surgeon performing the experiments and at this time cannot be quantified. This difficulty exists in all temporal bone experiments where a prosthesis is used to replace one or more ossicles. Angulation of the prosthesis may vary slightly from bone to bone but is easier to control and would produce only a small difference. The use of cadaver material does not appear to have a significant effect compared to live ears. 19 , 20
Mean change (dB) and SEM at eight representative frequencies for reconstruction with three different cartilage grafts using one-way analysis of variance (ANOVA) for statistical analysis
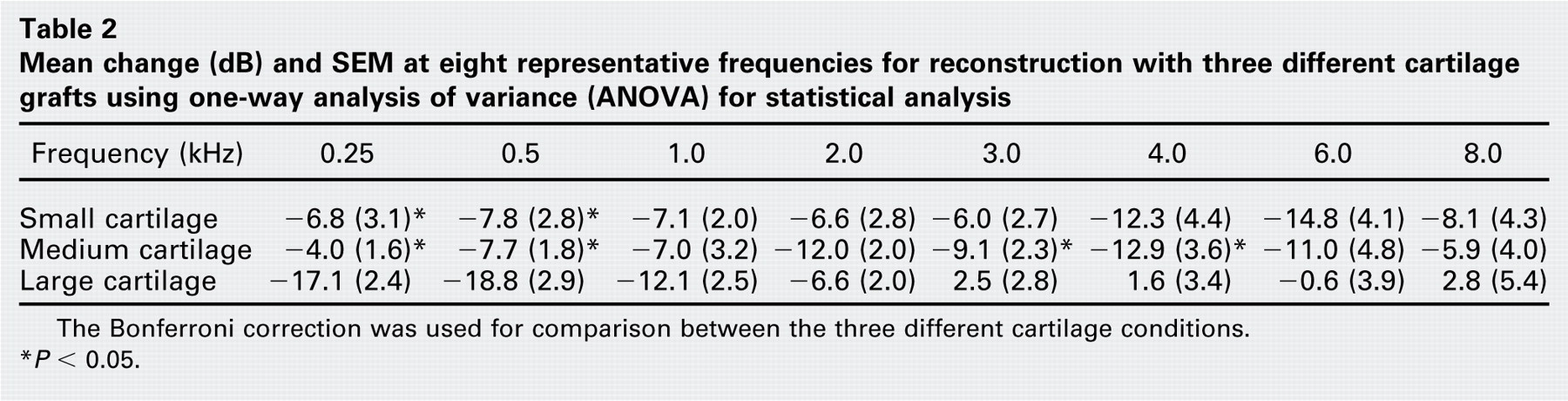
The Bonferroni correction was used for comparison between the three different cartilage conditions.
* P < 0.05.
Conclusions
We examined the acoustic effect of the presence of the malleus in middle ear reconstruction in a temporal bone model. Absence of the malleus impaired middle ear sound transmission slightly in the mid frequencies and improved it at higher frequencies compared to reconstruction with the malleus present. None of the effects were statistically significant. Interposing a large-diameter cartilage between the TM and a sculpted incus improved the high-frequency response the most at the expense of the low-frequency response.
Author Information
Author Contributions
Financial Disclosure
None.