
Abstract
Various minimally invasive and conservative techniques have recently been developed for stone removal, including extracorporeal and intracorporeal lithotripsy, interventional sialography and basket retrieval, and sialoendoscopy. 6 – 8 However, the rate of success of these new techniques has been found to vary and to decrease for large stones with a diameter >7 mm and for stones located in the hilum. We have therefore adopted a method of transoral removal of stones in the hilum of the submandibular gland. In a previous report, 9 we suggested that a new opening of salivary outflow in the submandibular duct overlying the stones may prevent symptom recurrence. That study, however, consisted of a small case series of submandibular calculi with no randomization. We therefore established a hypothesis that hilar submandibular stones can be transorally removed and that symptom recurrence can be prevented by following sialodochoplasty procedure. The aim of this study was to assess the utility of transoral stone removal followed by sialodochoplasty in patients with hilar submandibular stones and assess the functional outcomes of the glands after surgery.
Patients and Methods
Patients and Study Design
Between 2004 and 2006, 59 consecutive new patients (32 men and 27 women) with symptomatic stones in the hilum of the submandibular gland were enrolled into this prospective, randomized, case-controlled study. The patients were initially treated with transoral surgery to remove the symptomatic stones. Following stone removal, the patients were randomized to the additional creation of a neo-ostium (sialodochoplasty) or not. The two groups were matched according to age, gender, stone size, and palpability of stones. Recovery of salivary function and symptom recurrence between two groups were compared. The salivary function was measured by scintigraphy scanning, and recurrent symptoms were defined as recurrence of the preoperative symptoms, such as painful swelling or sialoadenitis. The study protocol was reviewed and approved by the institutional ethics committee, and all patients provided written informed consent.
The sample size was calculated for the detection of a significant difference (80% power, two-sided 5% significance level). A sample size of 30 in each intervention group was planned. On the basis of the results of the present study, a power analysis was performed. Two groups with/without sialodochoplasty were randomly allocated by an assistant. All other contributors to the study were blinded to generation and implementation of the treatment assignment. The outcome assessment and data analysis were also blinded.
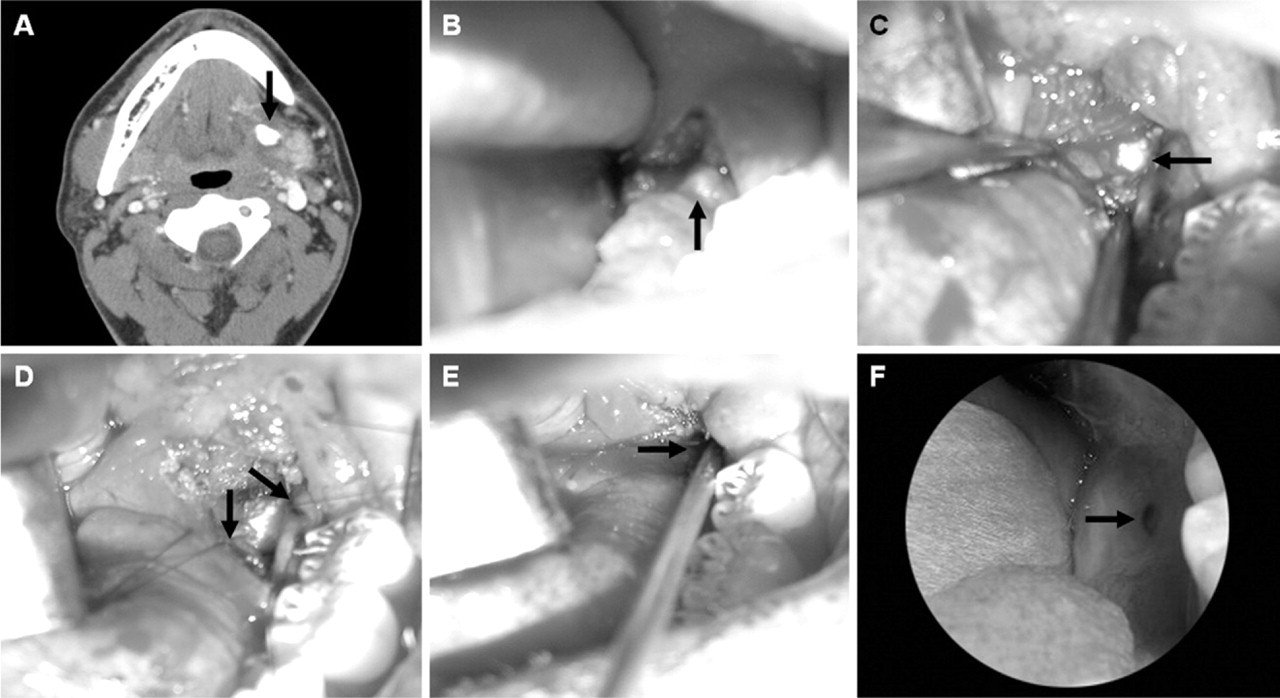
Photographs showing the operative procedure and outcome of transoral removal of a hilar submandibular stone and sialodochoplasty. An axial computed tomography showed a stone in the hilum of left submandibular gland
The mean age of the patients was 34 years (range 7-72 years). Fifty-seven (96.6%) patients complained of painful swelling of the gland, and 12 (20.3%) complained of recurrent infection. The mean duration of symptoms was 19 months (range 1-62 months). The mean size of the removed stones was 7 mm (range 3-15 mm). All stones were preoperatively defined by ultrasonography or CT. The stones were palpated in 40 patients but could not be palpated in 19.
Surgical Procedure
Stones in the hilum of the submandibular gland were transorally removed under general anesthesia. An incision was made in the floor of the mouth to expose the submandibular duct, which was traced back to the hilum of the gland. The stones were localized by bimanual palpation with upward pressing on the affected submandibular area. Once the stone had been visualized, it was released by a longitudinal incision in the duct. The lingual nerve crossing the duct was identified and carefully preserved. If the stones could not be easily localized by intraoperative palpation, the orifice of the duct was identified, and the duct was cannulated with a lacrimal probe, laid open at the mid or proximal portion, and dissected proximally to reach the stones. Scrupulous hemostasis was performed for clear visualization of the structures. Following stone removal, the duct was irrigated with saline.
For patients randomized to additional sialodochoplasty, the incised salivary ductal margins were sutured with oral epithelium using 5-0 Vicryl, creating a neo-ostium (Fig 1). For patients without sialodochoplasty, the incised duct and mucosa were left open. If stones could not be found intraoperatively, the proximal and hilar ductal roofs were incised and only sialodochoplasty was performed, on the basis of a hypothesis that the neo-ostium might prevent symptom recurrence though the stones remained in the hilum.
All patients were discharged the day after surgery. They were treated with antibiotics and analgesics for 1 week, as well as rinsing of their mouths with water.
Salivary Scintigraphic Examination
Salivary gland scanning was performed before and 6 months after surgery for quantitative assessment of function so as to compare the affected and unaffected sides and to compare pre- and postoperative values. All subjects refrained from eating, drinking, or smoking for a minimum of 90 minutes prior to scanning. None of the subjects had a history of medication to reduce salivation at the time of scintigraphy. Scintigraphic images were obtained 10 and 20 minutes after intravenous injection of 10 mCi technetium-99m pertechnetate and after salivary stimulation with lemon juice; a triple-detector gamma camera (Triad XLT 20; Trionix, Twinsburg, OH) was used. The uptake ratio of the gland before stimulation was obtained by dividing glandular uptake by background uptake at the shoulder area. Functional fraction was calculated as (maximal uptake ratio - minimal uptake ratio)/minimal uptake ratio before stimulation. Excretion fraction was calculated as (maximal uptake ratio after stimulation - maximal uptake ratio before stimulation)/maximal uptake ratio before stimulation.
Statistical Analysis
Results in each group are expressed as incidence or mean ± standard deviation. The Statistical Package for the Social Sciences for Windows, version 12.0 (SPSS Inc, Chicago, IL) was used for statistical analysis. Mann-Whitney U test was used for between-group comparisons of continuous variables; Wilcoxon signed rank test was used to compare paired samples; Fisher exact test was used to compare categorical data between groups. The quantitative values of the affected gland were compared with those of the unaffected normal gland, as well as between pre- and postoperative values and between patients who did and did not undergo sialodochoplasty. Differences were considered statistically significant at P < 0.05.
Results
Fifty-four of 59 (91.5%) patients showed complete removal of hilar submandibular stones: all 40 patients with palpable stones and 14 of 19 patients with impalpable stones (P = 0.002) (Fig 2). Of these 54 patients, 28 underwent additional sialodochoplasty and 26 did not. All five patients who did not show complete stone removal underwent sialodochoplasty.
The patients were followed for a mean of 24 months (range 12-46 months) after surgery and were assessed at each visit for surgical complications, symptom recurrence, and patency of the new ductal opening. Temporary lingual nerve hypoesthesia was experienced by three patients, whereas none developed ranula after surgery. Recurrent symptoms were observed in four of the 54 (7.4%) patients who underwent successful stone removal: two sialodochoplasty patients and two no-sialodochoplasty patients. Of these four patients, two underwent intraoral removal of recurrent salivary stones in the distal Wharton duct and two were managed conservatively. Recurrent symptoms developed in four of the five patients who did not show complete stone removal and only underwent sialodochoplasty; of these, two underwent gland resection and two were lost to follow-up.
The 54 patients who underwent successful stone removal were examined by salivary scintigraphy. Preoperatively, the mean salivary secretary value of the affected glands was significantly lower than that of the unaffected glands (P < 0.05). A comparison of the preoperative and postoperative scans of the affected gland showed significant improvement in 38 of 54 (70.4%) patients. Overall, the salivary function of the affected gland increased to that of the unaffected gland after surgery. Moreover, the difference between the groups who did and did not undergo sialodochoplasty was not statistically significant (P > 0.1; Table 1). At last follow-up, 24 of 28 (85.7%) patients who underwent complete stone removal and sialodochoplasty maintained the patency of their new ductal openings in the posterior floor of the mouth (Fig 1F). When the affected submandibular glands were massaged, saliva spilled from the openings. However, four patients with a stenosis of the neo-ostium had no symptom recurrence during follow-up. One of 26 (3.8%) patients who underwent complete stone removal and no sialodochoplasty maintained the patency of the previous marsupialization site.
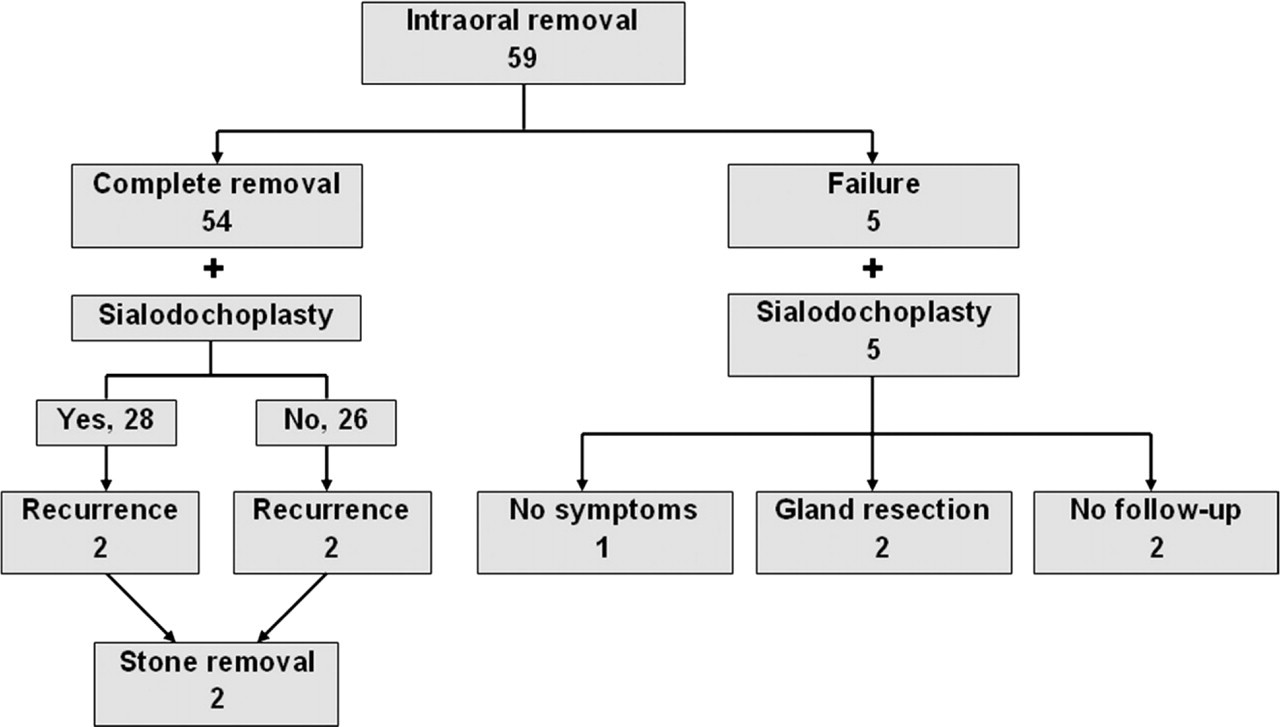
Schematic diagram for patients undergoing transoral removal of stones in the hilum of the submandibular gland.
Submandibular gland function of patients treated with and without sialodochoplasty after transoral removal of hilar submandibular gland stones
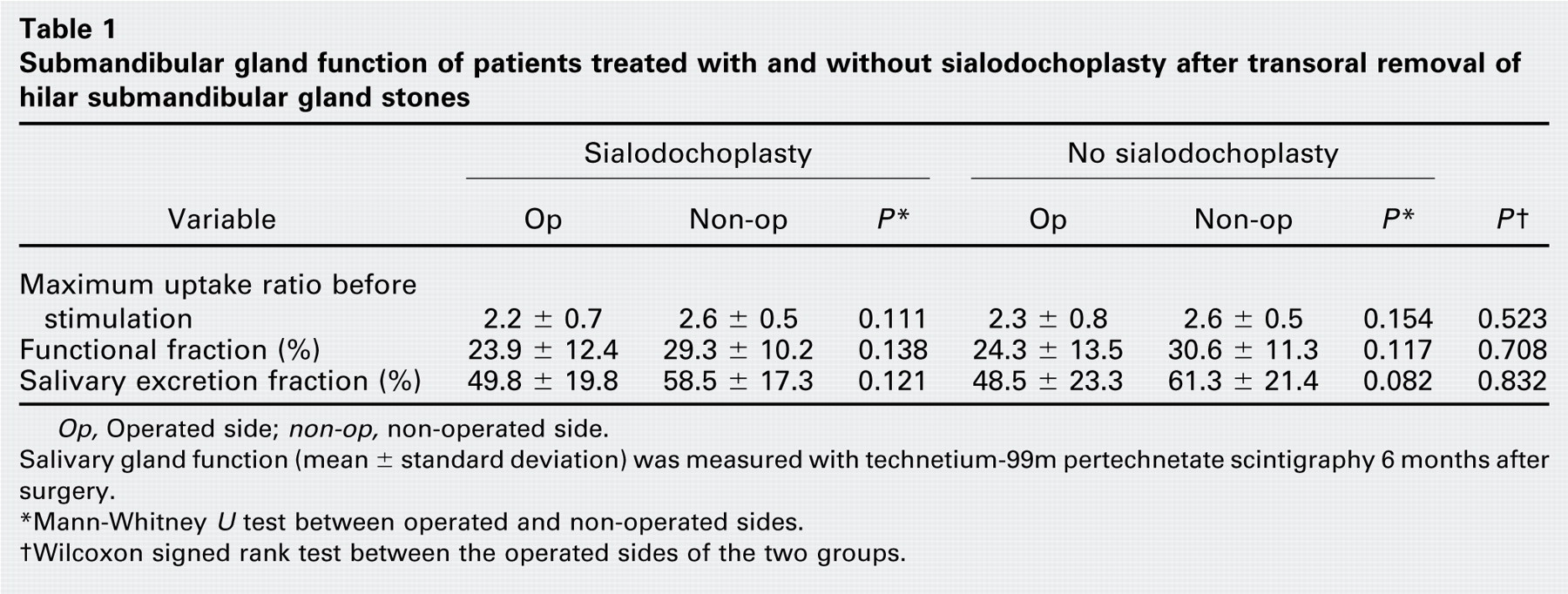
Op, Operated side; non-op, non-operated side.
Salivary gland function (mean ± standard deviation) was measured with technetium-99m pertechnetate scintigraphy 6 months after surgery.
Msup*Mann-Whitney U test between operated and non-operated sides.
Discussion
Treatment of salivary stones is changing from gland extirpation to gland-preserving surgery or minimally invasive techniques, including lithotripsy, interventional radiology, and sialoendoscopy. 6 – 8 These approaches are preferred because of mounting evidence that the secretory function of these glands can recover after the obstruction is removed. 5 , 9 , 10 This finding is supported by our results, which show that, although the affected submandibular gland had reduced function compared with the contralateral unaffected gland, many of the affected glands had improved function after stone removal. In our previous report, 9 salivary gland function was evaluated by direct measurement of salivary flow rate from a neo-ostium after stone removal and sialodochoplasty. Salivary flow rate, however, does not reflect actual submandibular gland function because of secretions from the sublingual gland and from the natural Wharton duct orifice. We therefore used salivary gland scintigraphy with technetium-99m pertechnetate, a method that reflects real flow rates from major salivary glands, 11 to quantitatively measure gland function. Preservation of gland function may prevent reduction of unstimulated salivary flow after excision of the submandibular gland. 12
We found that the success rate of transoral removal of a hilar submandibular stone was as high as 91.5 percent, similar to previously reported success rates. 1 , 9 , 10 , 13 – 15 For example, in a series of 102 patients with palpable perihilar stones who were treated by opening the duct up to the stones and creating a neo-ostium in the posterior mouth floor, the success rate was 91 percent, whereas the rate of stenosis of the neo-ostium was 2 percent. 1 Although our success rate was similar, our stenosis rate was higher (14.3%). However, symptom recurrence and recovery of salivary function after stone removal were unaffected by the presence or absence of a neo-ostium. In addition, we found that sialodochoplasty had no effect on postoperative outcomes, suggesting that the presence of the neo-ostium may have a minimal effect in preventing symptom recurrence after complete stone removal. In addition, the sialodochoplasty procedure itself may be ineffective in reducing symptoms when stones remain in the hilum after a failure of complete removal. Further, meticulous closure of the ductal incision may not be required to restore ductal patency or prevent recurrence. 13 , 14 Our findings and those of a previous study 15 suggest that wound healing and the recovery of gland function may be unaffected by ductal incision or by whether the mucosa is left open without any closure.
Transoral removal of stones in the hilum or gland is difficult and may be hazardous to the lingual nerve in some cases, especially for small impalpable stones. 1 , 15 All five patients who failed to show complete stone removal had impalpable stones in the hilum. Stone localization for transoral removal may be enhanced by probing the Wharton duct, 3 , 9 by making an incision in the duct by proceeding from the orifice, 1 or by dissecting the duct as an anatomical guide to reach the stone. 14 Further, ultrasound can be used to localize stones in the hilum or gland parenchyma during surgery, which may assist in removing impalpable hilar submandibular salivary stones. 15 The intraoperative use of ultrasound may also allow surgeons to ensure completeness of stone removal by checking remnant stones immediately after surgery. In patients in whom stones could not be easily palpated during surgery, the ductal orifice was probed and the incision was extended from the proximal duct to the hilum or parenchyma. These procedures provided successful removal in 14 of the 19 patients with impalpable hilar salivary stones; this success rate may increase with the intraoperative use of ultrasound. In addition, a sialoendoscope may be used to remove small stones in the hilum before transoral surgery, or it may be inserted through the incised opening of the proximal duct or hilum to facilitate intraoperative localization and removal.
Conclusion
We have shown here that stones in the hilum of the submandibular gland can be transorally removed with a high success rate and low-level risk. Previously described methods1,3,9,14,15 to facilitate stone localization may help find and remove the stones, even in patients with impalpable symptomatic stones in the submandibular hilum. Gland-preserving transoral surgery can restore gland function to normal after stone removal. Sialodochoplasty, however, had no effect in preventing symptom recurrence.
Author Information
Author Contributions
Financial Disclosure
None.