
Abstract
Background
We have noticed a protrusion on the pharyngeal wall in patients with Zenker's diverticulum (ZD). The protrusion gives the appearance of a neo-pharyngoesophageal segment (faux-PES) and may represent an adaptation to protect the airway.
Study Design
A case-control study.
Methodology
The fluoroscopic swallow studies of patients with ZD were compared with matched controls. Information regarding the presence and location of a faux-PES, true PES opening, pharyngeal constriction, and laryngohyoid elevation was compared.
Results
The fluoroscopic swallow studies of 31 patients with ZD were compared with 31 controls. A faux-PES was found in 100 percent of ZD patients and in 0 percent of controls. The mean maximum opening of the faux-PES was 1.5 (±0.27) cm. The faux-PES was located 1 cm above the true PES below the entrance to the supraglottic airway. This is the optimal location for airway defense.
Conclusions
The faux-PES was identified in 100 percent of patients with ZD. The faux-PES may represent a physiologic adaptation to protect the airway from regurgitation out of a ZD.
Participation of the pharynx in speech and swallowing has long been recognized. In the 1800s, Passavant described a ridge on the posterior pharyngeal wall that developed during speech in an individual with an unrepaired cleft palate.1 Subsequent investigation revealed variability in the exact location and configuration of the pad and identified it in both normal speakers and those with cleft palate.2–4 It is generally accepted that Passavant's ridge represents a compensatory behavior facilitating velopharyngeal closure for speech in some speakers. Other examples of pharyngeal adaptation are noted in swallowing. For example, restricted tongue movement increases compensatory anterior displacement of the pharynx. We have noticed a pharyngeal adaptation that occurs in association with Zenker's diverticulum (ZD).
ZD is a mucosal herniation in the hypopharynx at the posterior intersection of the upper border of the cricopharyngeus and inferior pharyngeal constrictor muscle fibers, an area referred to as Killian's dehiscence.5 At this site, the oblique fibers of the inferior constrictor meet the transversely oriented fibers of the cricopharyngeus muscle (CPM) to produce an area vulnerable to hernia formation. The exact cause of diverticula at this location has been debated. Zenker and von Ziemessen6 attributed it to a lack of coordination between bolus arrival at the upper-esophageal sphincter and opening of the upper-esophageal sphincter to accommodate the bolus. Over time, elevated hypopharyngeal pressures caused by this incoordination presumably produce herniation at the site of tissue vulnerability. Contemporary investigators have generally attributed the etiology of ZD to pharyngeal weakness or to a structural or functional abnormality of the pharyngoesophageal segment (PES) (eg, spasm, incomplete relaxation, myopathy, or atrophy of the CPM).7,8
A number of investigators have speculated that ZD may result from chronic extraesophageal reflux.9–11 Reflux (the regurgitation of stomach acid and pepsin, a proteolytic enzyme) is thought to result in dysfunction and hypertrophy of the CPM that, over time, produces excessive pressures in the hypopharynx and, eventually, herniation. Support for this idea comes from studies of the CPM in ZD showing histologic and biochemical changes consistent with fibrosis and loss or other alteration of muscle fibers as compared with normal,12,13 manometric studies showing abnormally high intrabolus pressures in ZD14 and, recently, evidence of excessive extraesophageal reflux in ZD patients on 24-hour pH monitoring.9 Symptoms in patients with ZD range from mild to extreme and include difficulty swallowing, bad breath, frequent expectoration or regurgitation, cough, aspiration, and weight loss. We have noticed that the body attempts to compensate for regurgitation out of the ZD with hypertrophy of the inferior pharyngeal constrictor. We have called this physical adaptation a PES or “faux-PES.” The purpose of this investigation is to describe pharyngeal adaptation in patients with ZD.
Methodology
Approval to conduct this study was obtained from the Institutional Review Board of the University of California, Davis. The records of all persons diagnosed with ZD at the Center for Voice and Swallowing between January 1, 2006, and December 31, 2008, were abstracted. Patients who had undergone previous surgical intervention for ZD were excluded. Each patient with ZD was age- and sex-matched to a fluoroscopic swallow study taken from a large group of normal control subjects.
All radiographic studies were conducted at UC Davis in accordance with the routine radiographic protocols approved by the institution. The equipment used included a properly collimated OEC Medical Systems 9800 Radiographic/Fluoroscopic unit (Salt Lake City, UT) that provided a 63-kV, 1.2-mA type output for the full field of view mode (12-inch input phosphor diameter). In accordance with our protocol, subjects swallowed a 1-mL, 3-mL, and 20-mL liquid bolus (EZ-PAQUE Barium Sulfate Suspension, 60%w/v, 41%w/w; E-Z-EM, Inc, Westbury, NY) from a spoon or cup. The bolus size was carefully measured with a syringe or graduated medicine cup. Timing information to hundredths of a second was superimposed on recordings by using a Video Stopwatch (Horita, Mission Vijeo, CA). A radiopaque disk of known diameter was placed on each subject's mid-chin so that displacements of structures could be calculated in the lateral view. When the protocol in lateral view was complete, the disk was moved to a position over the anterior edge of the posterior pharyngeal wall at the level of the UES for filming in the anterior-posterior view.
Fluoroscopy studies were recorded on a high-quality videotape or DVD recorder for later playback and analysis using a Sony Model SVO-9500 MD Videocassette S-VHS Recorder/Player or Sony Model DVD-1000 MD digital recorder (Sony Corp of America, New York, NY). For purposes of this study, only data for the 20-mL bolus size or largest bolus swallowed will be reported. Timing and displacement measures were obtained by using techniques previously described at length.15,16 All fluoroscopic studies were evaluated for the following: (1) the presence and location of a faux-PES; (2) the maximum opening of the true PES, defined as the narrowest point in the aerodigestive tract between vertebrae 3 and 6 (in lateral view) during this area's maximum distension on the largest bolus swallowed (PESmax); (3) the maximum displacement of hyoid during largest bolus swallowed (Hmax); (4) the pharyngeal constriction ratio (PCR), defined as the ratio of the pharyngeal area measured in the lateral view at the point of maximum pharyngeal constriction (PAmax) to the area measured with a 1-mL bolus held in the oral cavity (PAhold); and (5) the distance of the PES (as defined earlier) from the top of the tracheal air column at the point of the PES maximum distention during the swallow.
In addition to standard measures obtained for all patients, measures unique to swallowing in ZD patients were also extracted from the patient studies. These included the length and area of the diverticulum, the distance from the top of the tracheal air column to the faux-PES, and the maximum opening of the faux-PES during the swallow (Figure 1). Pearson correlations were used to assess relationships between the PES opening and the size of the diverticulum in the ZD group.

The measurements made for ZD patients include (a) the maximum extent of faux-PES opening (in cm) during swallow, (b) the maximum extent of PES opening (in cm) during swallow, (c) the depth (in cm) of ZD (from the top of the neck to the base, shown by white lines), and (d) the distance of the faux-PES from the top of the tracheal air column (in cm). In the anterior-posterior view (e), the area of diverticulum (in cm2) was calculated.
Data for the 2 groups were compared by using independent sample t tests, with the alpha adjusted for multiple tests (P = 0.05/5=0.01). All measures included were completed by two clinicians, with a portion of the data (20%) also measured by a third examiner. The reliability of displacement events across measurers has been previously reported as generally greater than 0.90, which was considered acceptable for study objectives.16
Results
Thirty-one patients with a ZD were age- and sex-matched to 31 control subjects. Each group was 68% male (21/21). The mean age was 66 years for the control group and 64 years for ZD patients.
The Prevalence of a Faux-PES
The faux-PES was present in 100 percent (31/31) of patients with ZD and in 0 percent (0/31) of normal control subjects. Examples of what we have termed the faux-PES are presented in Figures 2A-F. As seen in these illustrations, the faux-PES is a protrusion on the posterior hypopharyngeal wall that is present during the swallow and at rest in patients with a ZD. The true PES opening was 0.35 (±0.18) cm in patients with a ZD in comparison to 0.82 (±0.22) cm in control subjects (P < 0.01).
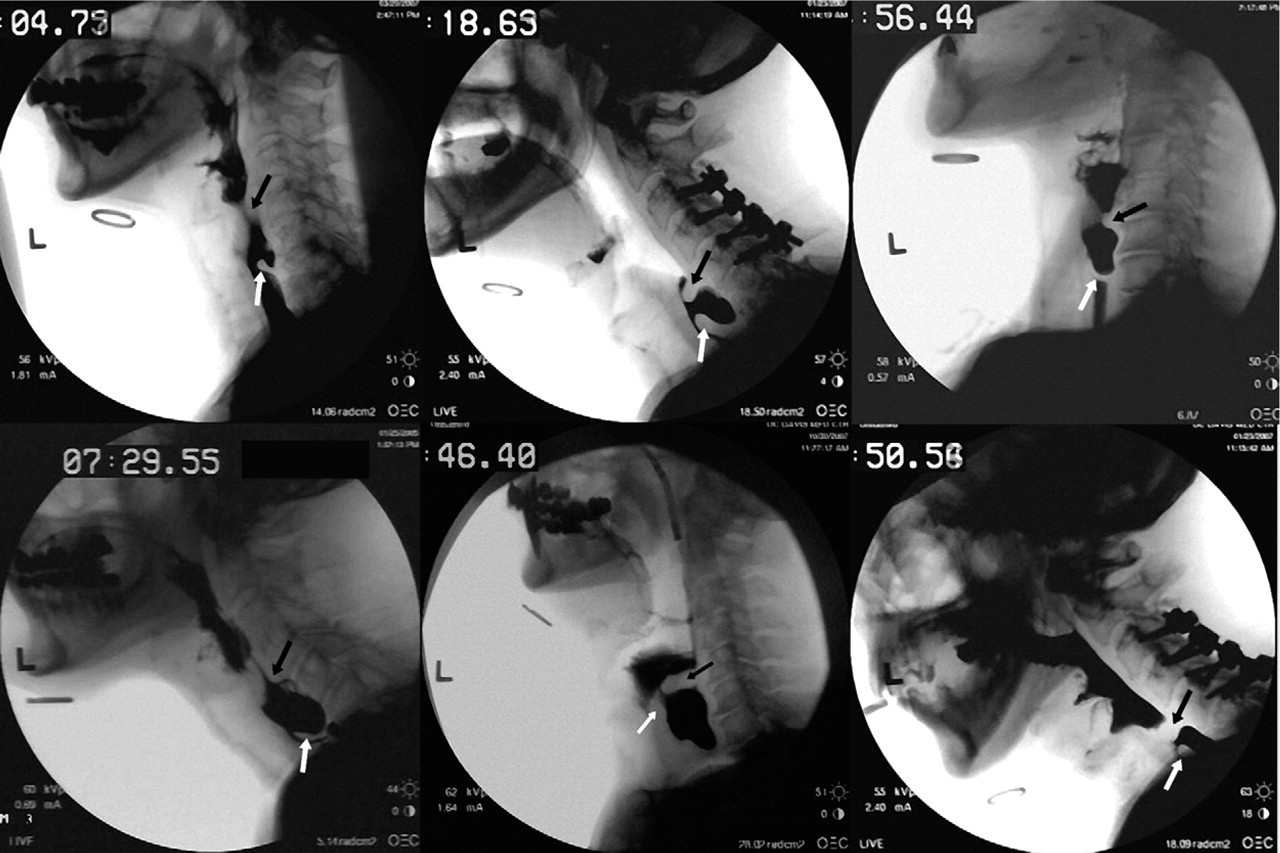
Examples of faux-PES in patients with ZD. Black arrows indicate faux-PES; white arrows denote true PES. The faux-PES is above the true PES, often substantially, and most likely develops in an attempt to protect the airway from material refluxed from the diverticulum or esophagus into the pharynx.
Characteristics of ZD and Faux-PES
The mean location of the faux-PES measured during bolus transit was 0.51 (±0.70) cm from the top of the tracheal air column. This was higher than the mean location of the true PES during the swallow in normal subjects (1.5 [±0.5] cm from the top of the tracheal air column). The mean maximum opening of the faux-PES in ZD patients was 1.5 (±0.27) cm. In all cases, the faux-PES was above the PES and below the entrance of the supraglottic airway, the optimal location for defending the airway from refluxate and not interfering with respiration.
An additional measure obtained in the ZD patients was the length from the top of the neck of the ZD, or the true PES, to the ZD base. The mean length was 1.62 (±0.61) cm. A measure of the area of the diverticulum, including both bolus material and air space that could be visualized, was extracted from the anterior-posterior view. Filming in the anterior-posterior view was completed after swallows in the lateral view and when bolus material had accumulated in the diverticulum. The range of values for this measure was from less than 2 to over 14 cm2, with a mean of 4.82 (±3.45) cm2.
Pearson correlations on these data revealed a modest correlation between neck length and the diverticulum area (0.53), and neither of these measures was significantly correlated with the maximum extent of the PES opening.
Characteristics of Swallowing in Normal Subjects and ZD Patients
Fluoroscopic measures from the 20-mL bolus swallow (or largest bolus swallowed) for both groups of subjects are presented in Table 1. The mean maximum opening of the true PES was markedly reduced in the ZD population (P < 0.01). The ZD and control groups did not differ significantly in maximum hyoid displacement during the swallow (P > 0.05). The true PES of patients with ZD was 2 to 3 cm below the top of the tracheal air column, substantially lower than the typical position of the PES in normal subjects (1.5 cm). This suggests that the PES migrates or is displaced inferiorly in ZD, with the faux-PES developing at a site proximal to the usual PES location.
Fluoroscopic findings in ZD patients and age- and sex-matched control subjects
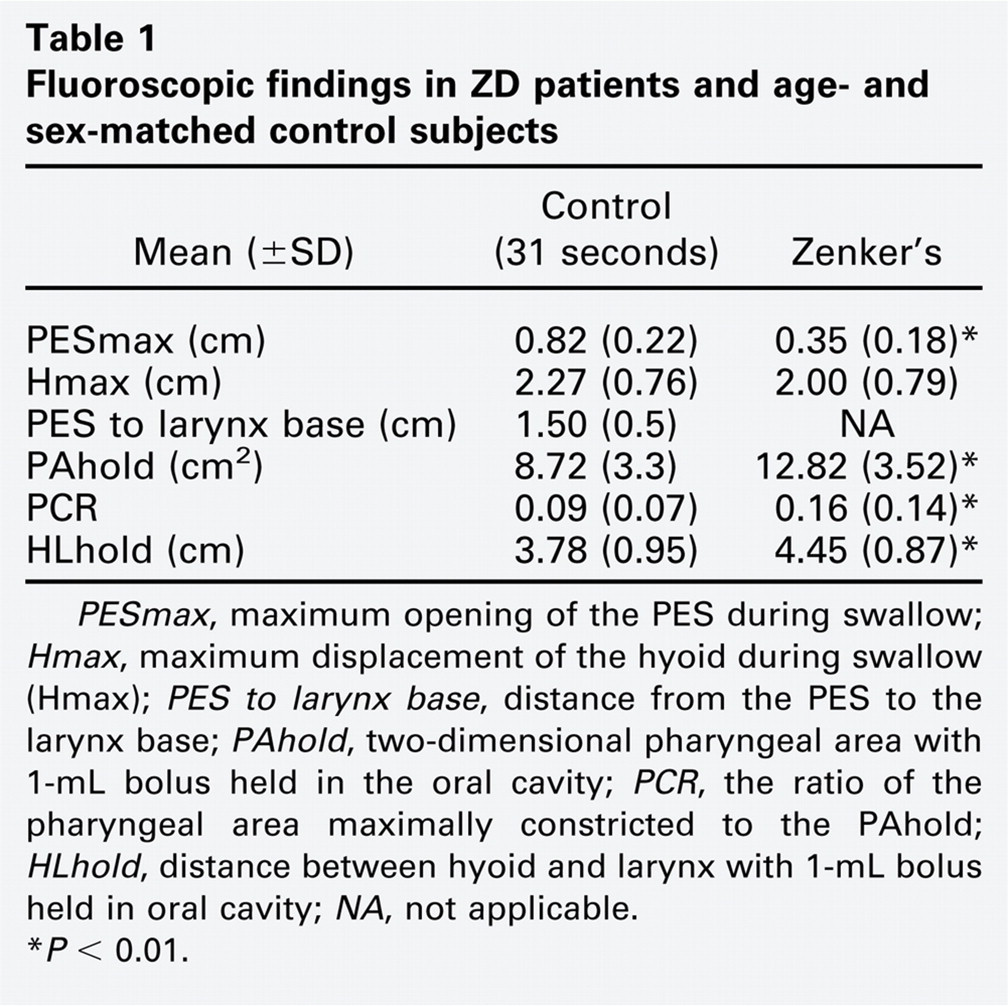
∗P < 0.01.
PCR, a measure of pharyngeal constriction during swallowing, was also compared in the control and ZD groups. PCR is a ratio of the pharyngeal area (lateral view) at the point of maximum constriction during the swallow (PAmax) to the area with a 1-mL bolus held in the oral cavity (PAhold). The mean PAhold (not including the area of the ZD) was significantly greater in the ZD patients (12.82 [±3.52] cm2) than in the sex- and age-matched normal subjects (8.72 [±3.30] cm2; P < 0.01). The PCR, a validated surrogate measure of pharyngeal strength, was significantly elevated in the ZD group (Table 1; P < 0.01). An elevated PCR suggests a weakened pharynx. The distance between the hyoid and larynx with a 1-mL bolus held in the oral cavity (HLhold) was also significantly greater in the ZD group (Table 1; P < 0.01). These findings suggest that the pharynx becomes larger and weaker in ZD patients as compared with normal subjects.
Discussion
The pharyngeal adaptation we have termed the faux-PES was identified in all 31 patients with ZD and in none of the control subjects. The faux-PES may represent a physiologic compensation to bolus material in the diverticulum and may function to help prevent regurgitation out of the ZD into the airway. This notion is supported by evidence that the faux-PES is present not only during swallowing, when it opens, but also before and after the swallow, when the airway is in a respiratory state. In addition, the faux-PES was always identified below the entrance to the supraglottic airway, a site that permits continuous airway defense from refluxate without interfering with respiration.
Based on our observation that the location of the faux-PES is above the area of Killian's dehiscence just above the CPM, we hypothesize that the faux-PES is primarily composed of fibers of the inferior pharyngeal constrictor muscle. The CPM is comprised of upper oblique fibers (pars oblique) and a lower band of horizontal fibers (pars fundiformis), both of which attach to the cricoid cartilage.17,18 These two compartments are both structurally and physiologically different. Mu and Sanders19 reported a greater proportion of type I, slow-twitch fibers in the horizontal portion, best suited to sustained activity, and a preponderance of fast-twitch type II fibers in the oblique portion of the cricopharyngeus, more appropriate for rapid, phasic movements. If the oblique compartment of the cricopharyngeus is a part of Killian's triangle, then the faux-PES may arise from the inferior hypopharynx, above the horizontal fibers of the CPM. Otherwise, it develops above both the oblique and horizontal compartments of the CPM. The true PES in ZD is composed of the horizontal fibers of the CPM.
If the faux-PES develops in response to an airway threat, it may parallel a PES response to chronic reflux. A number of patients in the current study aspirated material from the ZD, suggesting that faux-PES is not always effective in preventing reflux and protecting the airway. In the patients described, the faux-PES opened completely during the swallow. How or whether this might change over time, in the presence of a constant reflux threat, is not clear. This question is particularly interesting given possible differences in muscle fiber types in the true PES and faux-PES. Other features of swallowing in the ZD patients included a marked lowering of the PES and measures of two-dimensional pharyngeal area and length significantly greater than in control subjects. From a clinical perspective, the lower position of the PES and presence of the faux-PES in ZD may have implications for manometry or other pharyngeal instrumentation (ie, unless catheter placement can be visualized, it could be extremely difficult to differentiate the PES from the faux-PES and to interpret findings with accuracy).
Other findings in the current study appear to support the possibility that ZD is related to chronic reflux, as has been suggested by a number of investigators. First, the size of the PES maximally open during the swallow was significantly reduced in the ZD patients as compared with control subjects. This finding is consistent with a process that produces impaired opening of the PES, either structural or functional. In addition, hyoid displacement did not differ between the two groups, evidence that this component of PES opening was working appropriately.
Two measures of the size of the pharynx revealed the pharynx to be larger in the ZD patients as compared with the age- and sex-matched control subjects. If pressures in the hypopharynx are typically larger when the PES is obstructed and if these pressures are present over a long period of time, some general dilation of the pharynx may not be surprising. Chronic reflux that affects PES opening, related to either structural or functional changes, could be a contributing factor in this situation. Other possibilities for the greater pharyngeal length in the ZD patients may be related to a mechanical effect of the ZD. The PCR was significantly elevated in the ZD group, suggesting pharyngeal weakness.
Conclusion
Pharyngeal adaptation we have termed the faux-PES was present in 100 percent (31/31) of patients with ZD. The faux-PES may represent a physiologic compensation to bolus material in the diverticulum and functions to help prevent regurgitation out of the ZD into the airway.
Author Contributions
Financial Disclosures