
Abstract
The term adenoids describes lymphoid tissue on the superior and posterior walls of the nasopharynx, and their hypertrophy is a common condition of childhood. When enlarged, adenoids can obstruct the nasopharyngeal airway and cause mouth-breathing, hyponasal voice, and snoring. 1 , 2 In more severe cases, obstructive sleep apnea (OSA) may result, which carries potential risk of neurocognitive disturbance, growth failure, and cor pulmonale. 3 - 5 Adenoid hypertrophy can also be associated with otitis media with effusion, possibly through eustachian tube dysfunction or chronic adenoidal infection. 1 , 6
When children present with nasal airway obstruction, other potential diagnoses in addition to adenoid hypertrophy include rhinitis, nasal polyps, and septal deviation. Methods for identification of adenoid hypertrophy include the clinical history, examination (eg, with transoral mirror), imaging (eg, plain lateral x-ray), 7 or by direct palpation, usually with the patient under general anesthesia at the time of surgery for middle ear effusion. The gold-standard for diagnosis of adenoid-related nasal obstruction is considered to be fiber-optic nasendoscopy, which allows direct visualization of the nasal cavity with dynamic evaluation of any nasal airway obstruction. 8 , 9 It appears that the ratio of adenoid size to nasopharyngeal cavity dimensions, and not the absolute adenoid size, is primarily responsible for the nasal obstruction caused by adenoidal hypertrophy. 8
The management of adenoid hypertrophy that causes nasal obstruction in children is dependent on the clinical manifestations and any associated morbidity. In the presence of OSA, adenoid and tonsil hypertrophy are usually implicated, and tonsillectomy with adenoidectomy is generally indicated. Of note, the efficacy of adenoidectomy for children with OSA has not yet been formally investigated by randomized controlled trials. 10 In the absence of OSA, the risk-benefit ratio of surgical intervention for the individual child needs to be carefully assessed in light of potential anesthetic and postoperative complications (eg, hemorrhage, airway obstruction as a result of edema, and palatopharyngeal insufficiency). In mild cases, nonsurgical interventions may be considered, but few medical alternatives are available. Nonsurgical management is therefore commonly limited to treatment of any concurrent infection or specific complications of adenoid enlargement. 11
Interest has increased in the potential benefit of treating children with adenoid hypertrophy with intranasal corticosteroids. The mechanism by which steroids could reduce nasal airway obstruction is unclear, but several possibilities have been proposed: a lympholytic action of steroids on adenoids that can cause a direct reduction in size; a reduction in adenoidal and nasopharyngeal inflammation through the anti-inflammatory effect of steroids; or a reduction in the role of the adenoids as a reservoir for infection. 12 Despite the uncertainty over the precise mechanism, establishment of a therapeutic role for intranasal corticosteroids in children with adenoidal hypertrophy would have significant clinical implications. This modality may provide an effective nonsurgical alternative treatment for children with symptomatic adenoidal hypertrophy. Nasal steroids are widely considered safe in the pediatric population, although uncommonly reported potential adverse effects have included epistaxis, nasal mucosal irritation, septal perforation, adrenal suppression, and growth retardation. 13 - 15
The aim of this review is to systematically identify and appraise the available evidence for nasal steroids in the treatment of nasal obstruction associated with adenoid hypertrophy in children. This review is based on a Cochrane Review by the same authors, 16 and updates and widens the evidence-base to consider nonrandomized controlled trials in addition to randomized controlled trials.
Methods
Search Strategy
Original published studies on adenoid hypertrophy and nasal steroids were identified with a comprehensive search strategy in MEDLINE (from 1966 to April 2008), EMBASE (from 1974 to April 2008), and the Cochrane Central Register of Controlled Trials (CENTRAL) in Issue 3, 2008 of the Cochrane Library. The search terms used for adenoid hypertrophy were “adenoids [MeSH],” “adenoid*,” “adenotonsil*,” “hypertrophy*,” and “enlarge*.” The search terms used for steroids included: “anti-inflammatory agents [MeSH],” “steroids [MeSH],” “steroid*,” “corticosteroid*,” “glucocorticoid*,” “beclomethasone,” “mometasone,” and “fluticasone.” These terms were combined with Boolean operators. Reference lists from relevant articles, including other reviews, were searched. All searches were initially performed as part of a Cochrane review 16 but were updated in August 2008 to include newer and nonrandomized evidence.
Inclusion Criteria
The included studies comprised peer-reviewed randomized controlled trials (RCTs), comparative studies (historical and/or nonrandomized), observational studies, case series, and case reports. Only studies on human patients diagnosed with adenoid hypertrophy and symptoms of nasal obstruction who used nasal steroids as sole or adjuvant treatment, were included. The primary outcome measure of interest was improvement in symptoms of nasal obstruction, and secondary outcomes of interest included reduction in adenoid size and adverse events. Two authors independently assessed the titles and abstracts of all studies identified by the searches. The full articles were obtained where they appeared to meet the inclusion criteria. Studies not available in English were excluded.
Assessment of Quality
The evidence presented in the selected studies was categorized by level of evidence as defined by the Oxford Centre for Evidence-Based Medicine. Methodological quality of included trials was assessed using the five-point scoring system proposed by Jadad. 17
Data Extraction and Analysis
Data were extracted from the included articles independently by two authors, with a standardized data extraction form developed a priori. Descriptive statistics were extracted or calculated for outcomes (where possible), and a qualitative synthesis of the results undertaken. Where significant heterogeneity existed between outcome measures across the included trials, we planned to perform a meta-analysis with standardized mean differences. Unfortunately after contacting the corresponding authors, we were unable to obtain adequate original data from the studies to perform a formal meta-analysis, and data were therefore summarized in a narrative format.
Results
Study Selection
The search strategy identified 206 potential studies. After a review of the titles and abstracts, appropriate articles were retrieved and assessed independently by at least two authors for possible inclusion. Seven trials met the criteria for inclusion (Fig 1, trial flow). Studies that did not meet the inclusion criteria were also retrieved and reviewed if it was considered that they might contribute to the evidence-base on the subject.
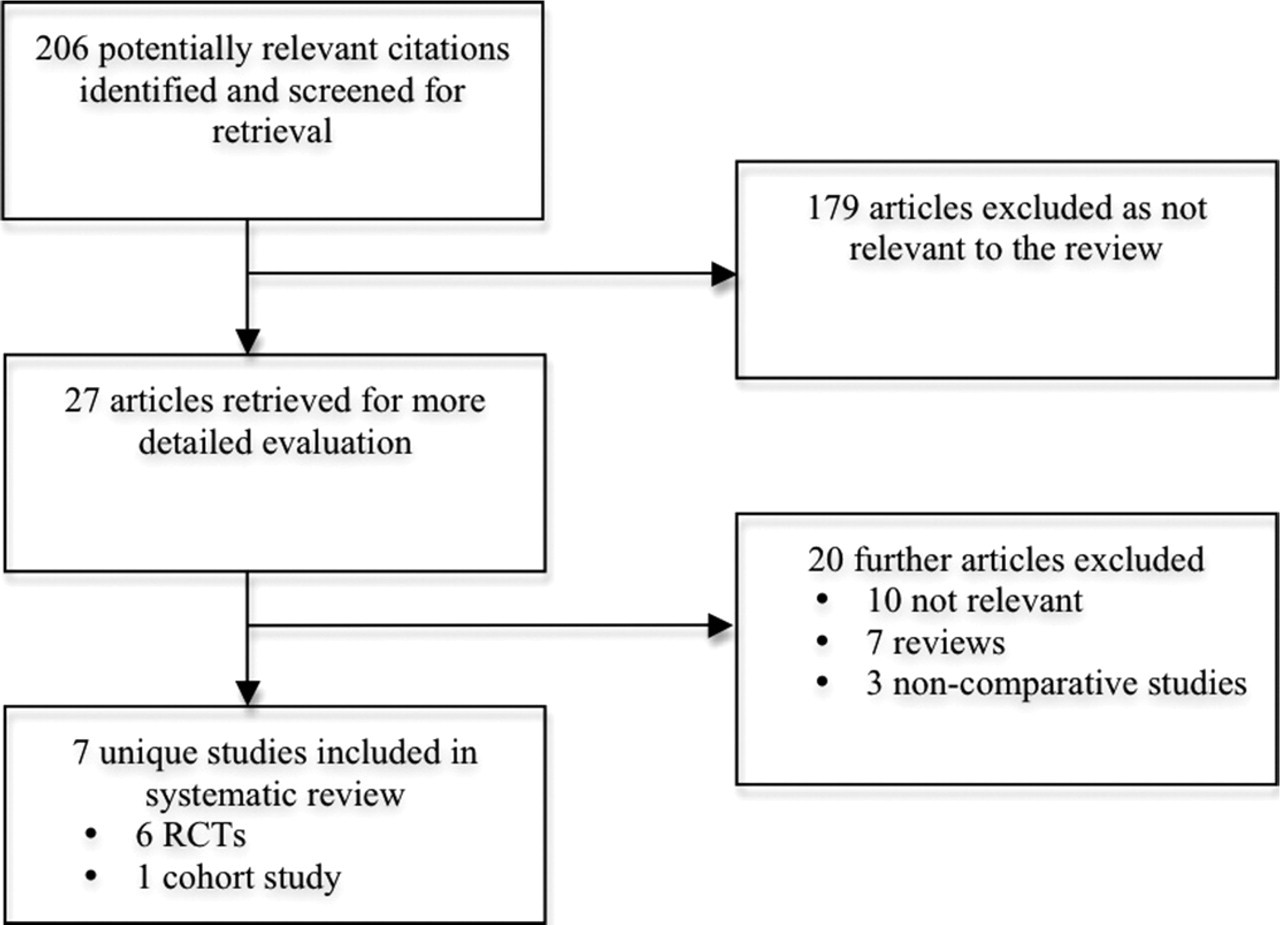
Flow chart summarizes trial flow in systematic review.
Included Study Characteristics
The included studies consisted of six randomized controlled trials (RCTs), and 1 cohort study. The characteristics of these studies are detailed in Table 1. Three of the studies excluded children with a history of allergic rhinitis, 18 - 21 and, in the remaining studies, the proportion of participants with allergic rhinitis were 9 percent, 22 15 percent, 23 and 53 percent 12 in the treatment groups and 9 percent, 19 percent, and 53 percent in the control groups, respectively.
Characteristics of the included studies
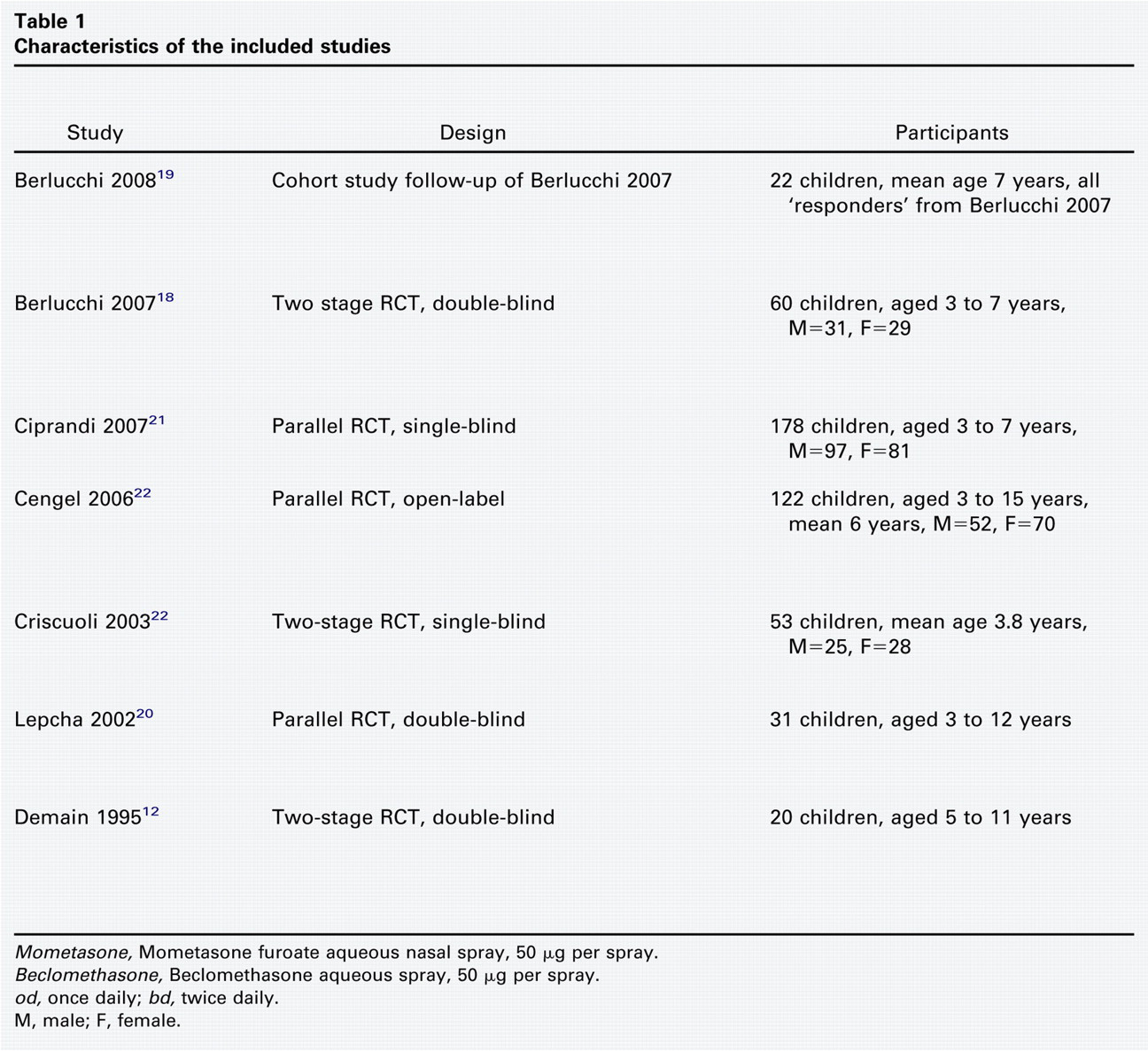
Mometasone, Mometasone furoate aqueous nasal spray, 50 μg per spray.
Beclomethasone, Beclomethasone aqueous spray, 50 μg per spray.
od, once daily; bd, twice daily.
M, male; F, female.
Effects of Interventions
A total of 471 children were enrolled in the five RCTs and 443 completed the trials. Nasal obstruction symptoms were improved with the nasal steroid intervention in five trials. 12 , 18 , 21 - 23 A reduction in adenoid size was demonstrated in four of these studies. 12 , 18 , 21 , 22 The cohort study 19 provided long-term follow-up data on the 22 patients who had demonstrated an improvement in an earlier study. 18 This study showed that those children who had continued treatment past the initial four months had further reduction in nasal obstruction and adenoid size. In contrast, one study 20 demonstrated no significant difference between the nasal steroid group and the placebo group in terms of symptoms of nasal obstruction or adenoid size.
Adverse Events
Adverse events occurred in two of the included studies. These studies reported epistaxis in a total of three participants in the treatment arms and one participant in the placebo arms, 12 , 18 and one of these studies reported stinging in six participants in the treatment arm and one participant in the placebo arm. 12 None of these complications resulted in a withdrawal from the trials.
Risk of Bias in Randomized Controlled Trials
The Jadad score 17 was four in three studies, 12 , 18 , 20 two in one study, 21 and one in two studies. 22 , 23 Five studies did not explicitly describe their methods of randomization, and the other study 22 used an inadequate method of randomization (allocating alternate patients). Allocation concealment was adequate in only one trial 12 and unclear in the remaining five trials. The methods used for double-blinding and description of dropouts were adequate in three trials. 12 , 18 , 20 Drug administration compliance was only adequately assessed in one study. 12
Discussion
Why Should Nasal Steroids Have Any Effect?
It has recently been demonstrated that adenoid tissue from children with adenoid hypertrophy (from obstructive sleep apnea or recurrent tonsillitis) had abundant glucocorticoid receptors and mRNA. 24 This suggests that these children may respond favorably to therapy with topical steroids. Potential mechanisms for the efficacy of steroids on the reduction of nasal airway obstruction include lympholytic action through the glucocorticoid receptors that causes a direct reduction in adenoid size; a reduction of adenoid inflammation through the anti-inflammatory effect of steroids; or steroid modulation of recurrent infection within the adenoids.
Evidence for Nasal Steroids Reducing Adenoid Size
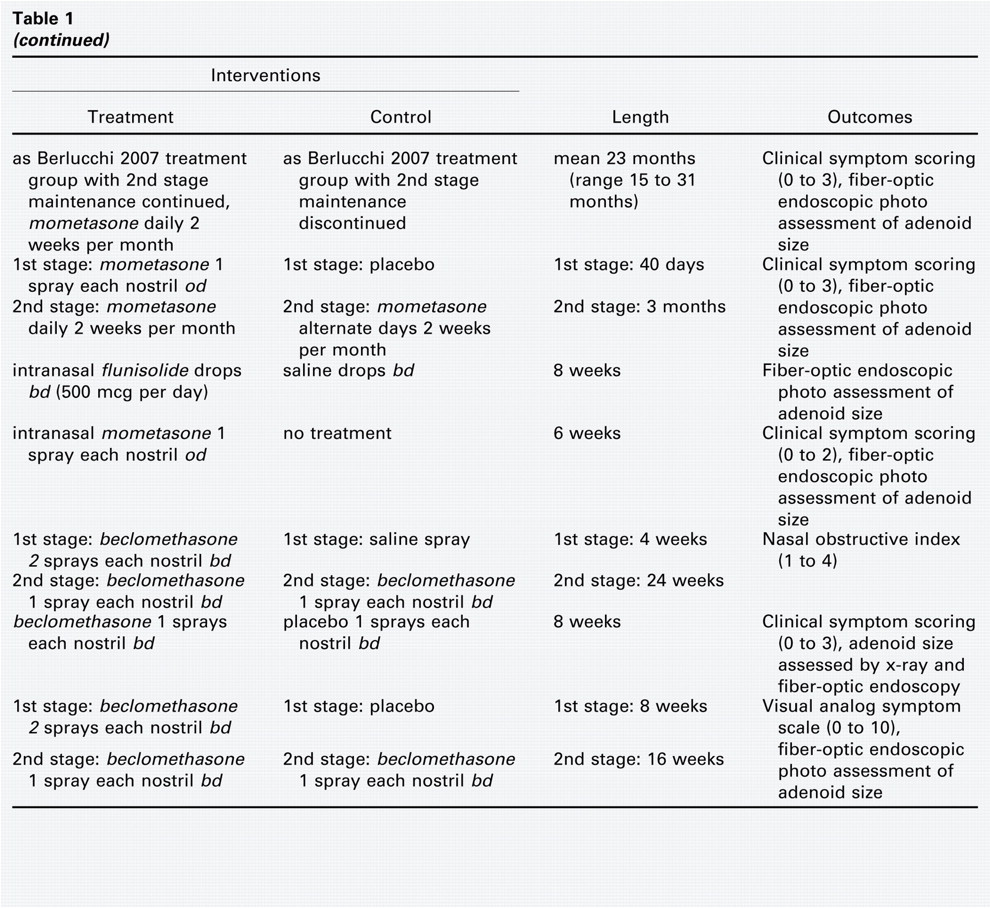
All of the six RCTs included in this review measured adenoid size after treatment with nasal steroids, and all but one demonstrated a statistically significant reduction compared with the placebo group (Table 2). The study, which did not demonstrate a statistically significant difference between the groups, 20 did suggest a trend toward a difference with a reduction in the obstruction grade of 0.39 in the treatment arm compared with 0.08 in the controls (P = 0.067).
Effect of nasal steroids on adenoid size
Methods used to assess adenoid size varied between the studies. Five studies assessed size with fiber-optic endoscopy examination of the nasopharynx. 12 , 18 , 20 - 22 In three of these studies, the two-dimensional area of the adenoid was measured relative to the area of the posterior choana, to determine an adenoid-to-choana ratio. 12 , 18 , 22 Another study used a grading system based on the magnitude of adenoid obstruction: first degree where adenoids occupied only the upper segment in the nasopharyngeal cavity with free choanal openings; second degree where adenoids were confined to the upper half of the nasopharyngeal cavity; third degree where the adenoids obstructed the choana with partial closure of eustachian tube orifice; and fourth degree where the obstruction was almost total and both the eustachian tube orifice and lower choanal border could not be observed. A further study used the distance from the adenoids to the vomer and scored this as grade 1 (>1 cm), grade 2 (0.5 to 1 cm), or grade 3 (<0.5 cm). 20 In addition, this study included lateral neck x-rays and reported the narrowest distance between the nasopharyngeal soft tissues and the soft palate (grade 1, >6 mm; grade 2, 4 to 6 mm; or grade 3, 0 to 3 mm).
In the cohort study that provided long-term follow-up from patients who had responded to nasal steroids in the initial RCT, further reduction of 20 percent in the adenoid-to-choana ratio was seen in the subgroup that continued with maintenance mometasone treatment as assessed by fiber-optic endoscopy. 19 In contrast, an increase of 15 percent was seen in the subgroup that discontinued nasal steroid therapy early (P = 0.01), and these children ended-up undergoing adenoidectomy.
Recent work has confirmed that fiber-optic endoscopy is a highly accurate method for diagnosis of adenoid hypertrophy, 25 and it has become accepted as the gold-standard. This technique can be safely and easily performed in co-operative children by skilled operators; and it provides an objective and dynamic view of the relationship between adenoid size and nasopharyngeal airway. A new grading system for fiber-optic evaluation has recently been proposed and validated 26 that may provide future studies with a more reliable measure than estimation of ratios. The use of a consistent measure would also facilitate meta-analysis and comparisons between studies. Other recent work has demonstrated that video fluoroscopy can be a safe and reliable alternative that correlates well with fiber-optic endoscopy findings. 27 This may in particular have a role in those children in whom fiber-optic examination cannot be tolerated.
Evidence for Nasal Steroids that Reduce Symptoms of Obstruction
Five of the included RCTs measured symptoms of nasal obstruction as an outcome measure, 12 , 18 , 20 , 22 , 23 with different symptom scores used. Four studies showed statistically significant decreases in the symptom score, and one study showed no significant difference. The symptom scoring systems used and differences between the studies are detailed in Table 3.
Effect of nasal steroids on symptoms of nasal obstruction
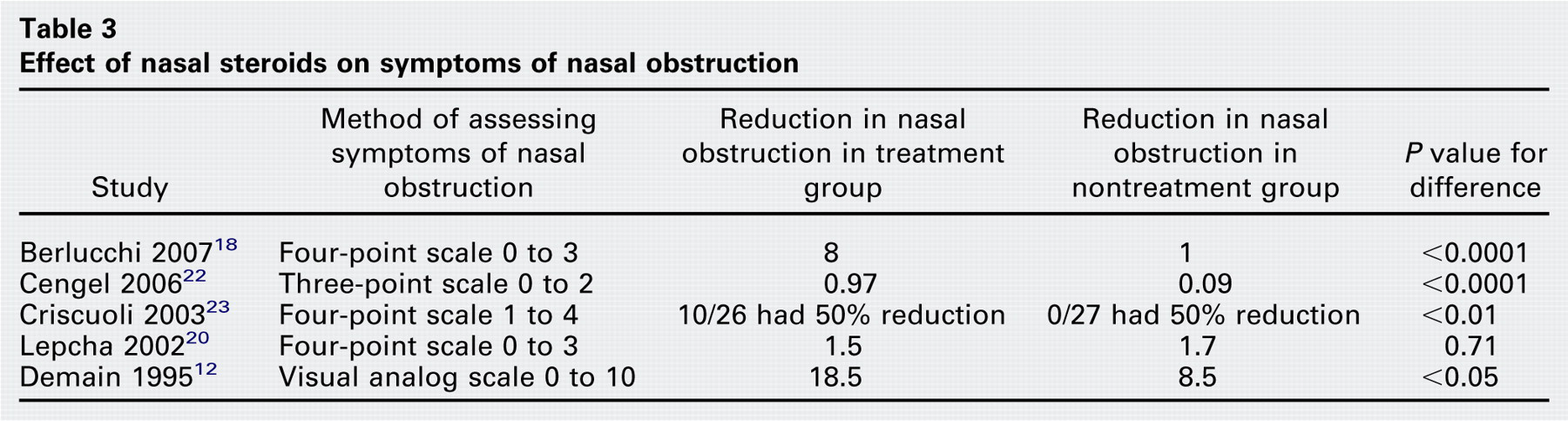
In the cohort study that provided long-term follow-up from patients who had responded to nasal steroids in the initial RCT, the mean symptom score was reduced from 2.0 (at the end of the initial trial period) to 0.0 in the subgroup that continued with maintenance mometasone treatment, but increased from 1.5 to 8.0 in the subgroup that discontinued nasal steroid therapy early (P < 0.001).
A good correlation between nasal symptom score and adenoid-to-choana ratio was found in the two studies 12 , 22 in which it was reported. This finding together with the findings of both nasal obstruction and adenoid size being reduced in five of the six RCTs leads to the logical presumption that the improvement in nasal obstruction symptoms may be as a result of nasal steroids reducing adenoid size.
A variety of symptom scoring systems have been used in the included studies. Future work would benefit from consistency in the measures used to allow comparison and pooling between studies. The longest established scoring method for nasal obstruction in children with adenoid hypertrophy is the Nasal Obstructive Index in which the degree of patients' mouth breathing and speech hyponasality were rated on a 4-point scale (none = 1; mild = 2; moderate = 3; marked = 4). 2 This measure showed good interobserver agreement and correlated well with roentgenographic assessment. Further work to validate the Nasal Obstructive Index against the gold standard (fiber-optic endoscopy) would be beneficial.
Which Steroids and at What Dose?
The questions of which steroid and what dose were not specifically addressed in the identified studies. As different studies used different treatment regimens, some information can be inferred from comparisons between them. Three trials used nasal beclomethasone, and two of these showed significant improvement in nasal obstruction and reduction in adenoid size after a two-week treatment period, with initial daily doses of 336 and 400 μg. 12 , 23 These studies then moved patients onto a maintenance lower dosage (168 and 200 μg/day), and benefits persisted. In the contrasting study that demonstrated no statistical benefit, beclomethasone was administered at a lower dosage (200 μg/day) for an eight-week period. 20 This suggests that a higher initial dose of nasal beclomethasone may be needed to effectively treat the adenoidal hypertrophy, which can then be followed by a lower dose in maintenance therapy.
In the two randomized controlled studies that administered mometasone, doses of 50 μg/day for 40 days and 100 μg/day for 42 days were used. 18 , 22 The study that used the lower dose then changed the patients to a three-month maintenance second stage with 50 μg on alternate days or daily for the first 2 weeks per month. Both studies showed significant improvement in symptoms and adenoid size after the regimens. The follow-up cohort study from the group with the maintenance period showed further improvement in symptoms in children who continued on the low dose maintenance (25 to 50 μg/day for 2 weeks per month) for a further 15 to 31 months (mean, 23 months). 19 These three studies suggest that mometasone at an initial dose of 50 to 100 μg/day will be initially effective, and this can be followed by maintenance on a lower dose (25 to 50 μg/day for 2 weeks per month) to give long-term efficacy.
Long-term follow-up with beclomethasone was limited to one study that included a follow-up period of 100 weeks. 23 Of 24 patients who had responded to the initial two-week therapy with beclomethasone (400 μg/day) and then had an additional 24-week treatment at the lower dosage (200 μg/day), an adenotonsillectomy was still warranted in 13 (54%) patients at 100-week follow-up. This suggested that the nasal obstruction reappeared or worsened in over half of the patients two years after the clinical improvement obtained by a 26-week treatment with intranasal steroids. These results suggest that in the case of beclomethasone, discontinuing treatment after 6 months will confer a longer-term (two year) benefit in about half of patients, but as in the case of the mometasone, continuing the beclomethasone at a low maintenance dose may be necessary for prolonged benefits in many other patients. Further studies are needed to define the long-term outcome in patients who initially respond to the steroid therapy.
Were Nasal Steroids Safe?
The use of nasal steroids in children is well-established, particularly for allergic rhinitis, and safety is widely recognized. 28 , 29 Rare adverse events occurred in two of the included studies. Two studies reported epistaxis 12 , 18 and one study reported stinging and sneezing. 12 None of these complications resulted in a withdrawal and they were recognized as infrequent. However, even when combined, the included studies incorporated a relatively small number of patients (493) and their design was not appropriate for drawing strong conclusions on the risk of adverse effects from nasal steroids, particularly the potential systemic effects such as adrenal suppression and growth retardation. As it appears from the above discussion that long-term maintenance may be necessary for long-term efficacy in some patients, the safety of long-term use of nasal steroids in children needs to be considered. Several prospective and retrospective studies have been performed to explore the possibility of hypothalamic–pituitary–adrenal axis suppression, bone density effects, growth retardation, cataract formation, and glaucoma in children. 28 - 31 The available information suggests there is no concern about any of these adverse effects with currently available nasal steroids with lower bioavailability (eg, mometasone and fluticasone), but there is some limited evidence that a possible growth-suppressive effect might be associated with those of higher bioavailability (eg, beclomethasone). 32
Study Limitations
This review has expanded on a Cochrane review on this subject, having a wider remit of the available evidence available for consideration. 16 The included studies had a number of methodologic weaknesses that may be detrimental to the evidence available to this review. In particular, none of the studies used a sample size calculation or analyzed patients on an intention-to-treat basis. The methods used for randomization were not adequately described in six of the studies; in the seventh, alternate patient allocation was used that is a method subject to potential bias. 22 Double-blinding was not used in all the studies, which creates potential bias, and one study did not use a placebo preparation. 22 In addition, the symptom scores used, methods of assessment of adenoid size, and reports of results were not standardized which precludes extraction of sufficient data on effect size for meta-analysis.
Another potential concern is a confounding effect of nasal obstruction caused by allergic rhinitis, which could also benefit from nasal steroid treatment. All the included studies only included children with a primary diagnosis of adenoid hypertrophy as their cause of nasal obstruction, excluding other causes such as nasal anatomic anomalies (eg, nasal septum deviation) or sinonasal disease (eg, hypertrophy of inferior turbinates, nasal polyposis, and craniofacial malformations). The studies also either excluded children with a history of atopy or allergic rhinitis, or identified atopy (through clinical history and skin prick testing) and excluded subgroup differences. Although there was no clear influence of any direct nasal response on the perceived efficacy of nasal steroids in adenoid hypertrophy, it is impossible to completely rule out a combined effect of the treatment on the adenoids and nasal lining in some or all of the studied children. It is important to note, however, that as well as adenoid hypertrophy, atopy and allergic rhinitis are common conditions of childhood, and if the efficacy of nasal steroids in treating nasal obstruction is through a multi-factorial effect, then this does not detract from it as a potentially powerful nonmedical option.
Evidence from Other Excluded Studies
Useful information can be gained from consideration of a number of other studies that did not meet the criteria for inclusion in this review. In particular, several researchers have explored the potential for efficacy in the use of nasal steroids to treat obstructive sleep apnea (OSA) associated with adenoid hypertrophy. In a pilot study, one group tried systemic prednisolone to look for an effect. 33 They found that adenoid size may have been slightly reduced after a short five-day course, but this treatment was otherwise ineffective. A randomized controlled trial used fluticasone 200 μg/day for one week and then 100 μg/day for five weeks in children with OSA and adenoid hypertrophy. 34 They found a decrease in apneas and hypopneas on polysomnography but were unable to demonstrate a change in adenoid size on lateral neck x-rays. An improvement in OSA that persisted for nine months after a four-week course of nasal budesonide 200 μg/day was found in another RCT on OSA children with adenoid hypertrophy, but unfortunately post-treatment lateral x-rays were not performed so the effect on adenoid size was not known. 35
A more recent crossover RCT in children with mild OSA used nasal budesonide (62 μg/day) or placebo for six weeks, and then after a two-week washout period swapped the groups for a further six-week period. 36 After six weeks of treatment, a significant decrease was found in adenoid size, measured by lateral x-ray adenoid-to-choana ratio (from 0.71 to 0.57, P < 0.0001). Signs of OSA on polysomnography were also improved, and these improvements persisted for at least eight weeks after cessation of treatment.
Conclusion
The available evidence suggests that nasal steroids may significantly improve symptoms of nasal obstruction in children with adenoid hypertrophy. The likely mechanism is through a reduction in adenoid size, and this has been shown to occur concurrently. The effect of nasal steroids on adenoid hypertrophy appears to be a group effect, not specific to any particular steroid, as the included studies used three different agents (mometasone, beclomethasone, and flunisolide). This is consistent with recent work that has demonstrated high levels of steroid receptors and mRNA in adenoid tissue. Nasal steroids appear to be safe and well-tolerated in children, and this makes the prospect of this nonsurgical management option attractive. However, although the available evidence is compelling, before nasal steroids can be recommended as a first-line therapy in these children, more robust high-quality randomized controlled studies are needed to confirm the results of the seven included studies. In particular, future work should focus on the optimal duration of treatment, minimum effective dosage, long-term efficacy, and the safety of long-term maintenance therapy.