
Abstract
Epistaxis is a common problem in children, affecting 30 percent of children 0 to 5 years old, 56 percent of children 6 to 10 years old and 64 percent of children 11 to 15 years old. 1 Most bleeds are minor and self-limiting and no medical attention is sought. Most commonly, the bleeding comes from the anterior septum, and crusting, vestibulitis, and digital trauma have been suggested as causative factors. 2 , 3 Underlying bleeding disorders may also cause epistaxis and previous studies have shown that 5 percent to 10 percent of children with recurrent epistaxis may have mild von Willebrand's disease. 4 , 5
A previous study 6 from this department has shown that nasal colonization with Staphlococcus aureus is more common in children with epistaxis than controls, and postulated that S aureus colonisation causes inflammation and new vessel formation leading to epistaxis. This is the rationale for the use of antiseptic nasal cream in pediatric epistaxis.
Previous randomized controlled trials in this department have shown that Naseptin cream (0.5% neomycin and 0.1% chlorhexidine; Alliance Pharmaceuticals, Chippenham, Wiltshire, UK) is an effective treatment for pediatric epistaxis 7 but that petroleum jelly is no more effective than simple observation. 8 Trials from other units have compared silver nitrate cautery with antiseptic cream. These studies were small, nonblinded, and conducted in mixed adult and pediatric populations. They did not show any difference in resolution rates between the two groups. 9 , 10
A Cochrane review in 2004 concluded that optimal management of children with recurrent nosebleeds is unknown and recommended more research. 11 The hypothesis in this study was that cautery with silver nitrate would give an additional benefit to antiseptic cream alone where there were visible new blood vessels on the anterior nasal septum.
Methods
Participants
Approval was obtained from the hospital's Research Ethics Committee. All patients referred to our department with recurrent epistaxis were seen in a dedicated research clinic. Included in the study were any patients under 16 years of age with a history of nosebleeds in the 4 weeks before being seen in the clinic and with visible vessels on the nasal septum on the side of reported bleeding. Exclusion criteria were any known bleeding disorder or allergy to the ingredients of Naseptin cream (peanuts, neomycin, chlorhexidine, soya). Use of antiseptic nasal cream before referral was not considered a reason to exclude the child from the trial. Many children (the exact number was not recorded) had received antiseptic cream from their general practitioner before being seen in the clinic. The use of this was usually intermittent and inconsistent and in no cases had been used consistently for 4 weeks, as in this trial, and so was not considered an exclusion criterion.
All patients received standard care in the clinic including history, examination, and laboratory tests as appropriate. Information was recorded on frequency, duration and site of bleeding, medical history, and associated nasal symptoms. The examination was performed with a headlight and Thudicum's nasal speculum. The presence of visible vessels and crusting and any other findings were recorded. The recruitment period took 15 months and all the participants but 3 were seen by the principal researcher.
Objective
The objective of the study was to establish whether a treatment regimen of silver nitrate cautery and 4 weeks of antiseptic nasal cream is superior to antiseptic cream alone in the management of pediatric epistaxis where there are visible new vessels on the anterior nasal septum.
Sample Size
A power calculation was performed based on the results from previous trials in our department. 6 , 7 In these studies, the proportion of children treated with only antiseptic cream who achieved complete resolution of their epistaxis at week 8 was approximately 55 percent. We chose to define a minimum clinically important difference as an additional 25 percent resolution rate from the combined treatment, over and above the resolution rate in children treated with cream alone (number needed to treat = 4). Therefore, in order to demonstrate a significant effect of the combined treatment, 80 percent of patients in this group should have resolution of their epistaxis at week 8. To have a 75 percent power to detect such a difference at a significance level of 0.05, we calculated that we would need 54 patients in each arm of the study.
Randomization
Those who agreed to participate were randomly allocated with sequentially numbered, sealed, shuffled envelopes that contained the instructions “treatment” or “control.” The allocation was carried out by the principal investigator who opened the envelopes once the patient had agreed to participate.
Interventions
Once eligibility was confirmed on history and examination, both treatment and control groups had preparation of the nose by application of lignocaine solution either in spray form (2%) or soaked in a cotton wool pledget (4%). The treatment group underwent silver nitrate cautery with caustic applicators that contained 75 percent silver nitrate and 25 percent potassium nitrate (Bray Group Ltd, Faringdon, Oxfordshire, UK) to any visible vessels on the anterior nasal septum, whether on one or both sides of the septum followed by a course of antiseptic cream (Naseptin) topically twice daily for 4 weeks. If there were no visible vessels, cautery was not performed. The control group underwent sham cautery with the inactive end of the applicator followed by antiseptic cream topically twice daily for 4 weeks. The sham cautery was intended to blind the patients and their parents to their allocated treatment.
Blinding
The study was designed to be double-blind. Children and parents were blinded to treatment allocation by the use of sham cautery. Outcomes assessment was done in clinics held on different days and with different surgeons from the enrollment clinics, so that the assessor was blind to the original treatment allocation.
Outcomes
The patients were followed up in clinic 8 weeks later by a researcher who was not involved in randomization and the assessment of new patients and who was therefore blinded to the original treatment.
The primary outcome measure was no reported bleeding in the 4 weeks before follow-up. Any bleeding was defined as treatment failure. A secondary outcome measure of reduction in symptoms (reduced number of bleeds as judged by parents) was also recorded. This was subjectively reported by the patients or parents as a reduction in the number of bleeds. Any complications were also recorded. Results were analyzed on an intention-to-treat basis. We accepted that not all patients would be compliant with the full course of antiseptic cream and made no effort to objectively check compliance in this regard. All patients not attending follow-up were sent a further appointment and subsequent nonattenders were contacted by telephone.
Statistical Methods
Statistical comparison of the two groups was made with the χ2 test, calculation of the relative risk reduction (RRR), and number needed to treat (NNT).
Results
Study Population
The recruitment started in October 2006 and finished in February 2008. Follow-up was completed by April 2008. Over the 15 months of recruitment, 261 children were referred with epistaxis of whom 229 attended the clinic. The mean age was 7.4 years (range, 1 to 13 years). There were 145 boys and 84 girls. The demographics were similar in both groups. The duration of symptoms ranged from 1 month to 9 years; the majority had symptoms for at least a year (n = 145), and the frequency of bleeding ranged from 6 times per day to monthly. Most had no other nasal symptoms but 35 complained of blockage, 4 rhinorrhea, 6 both blockage and rhinorrhea, and 7 pain.
Of the 229 children who attended the clinic, 43 were ineligible for inclusion as they had not had a bleed in the last 4 weeks (n = 33), they were allergic to one of the constituents of Naseptin cream (n = 3), they had coagulation disorders (n = 4), or they refused examination (n = 3). This left 186 who met the entry criteria, of whom 155 had visible septal vessels; 109 agreed to participate and were randomized. Refusal to participate was due in every case to a strong parental preference for one of the treatments offered. Fifty-four were randomized to the treatment group (cautery plus antiseptic cream) and 55 to the control (antiseptic cream alone). Complete data were available for 46 in the treatment group (85%) and 47 in the control group (85%). (Fig 1).
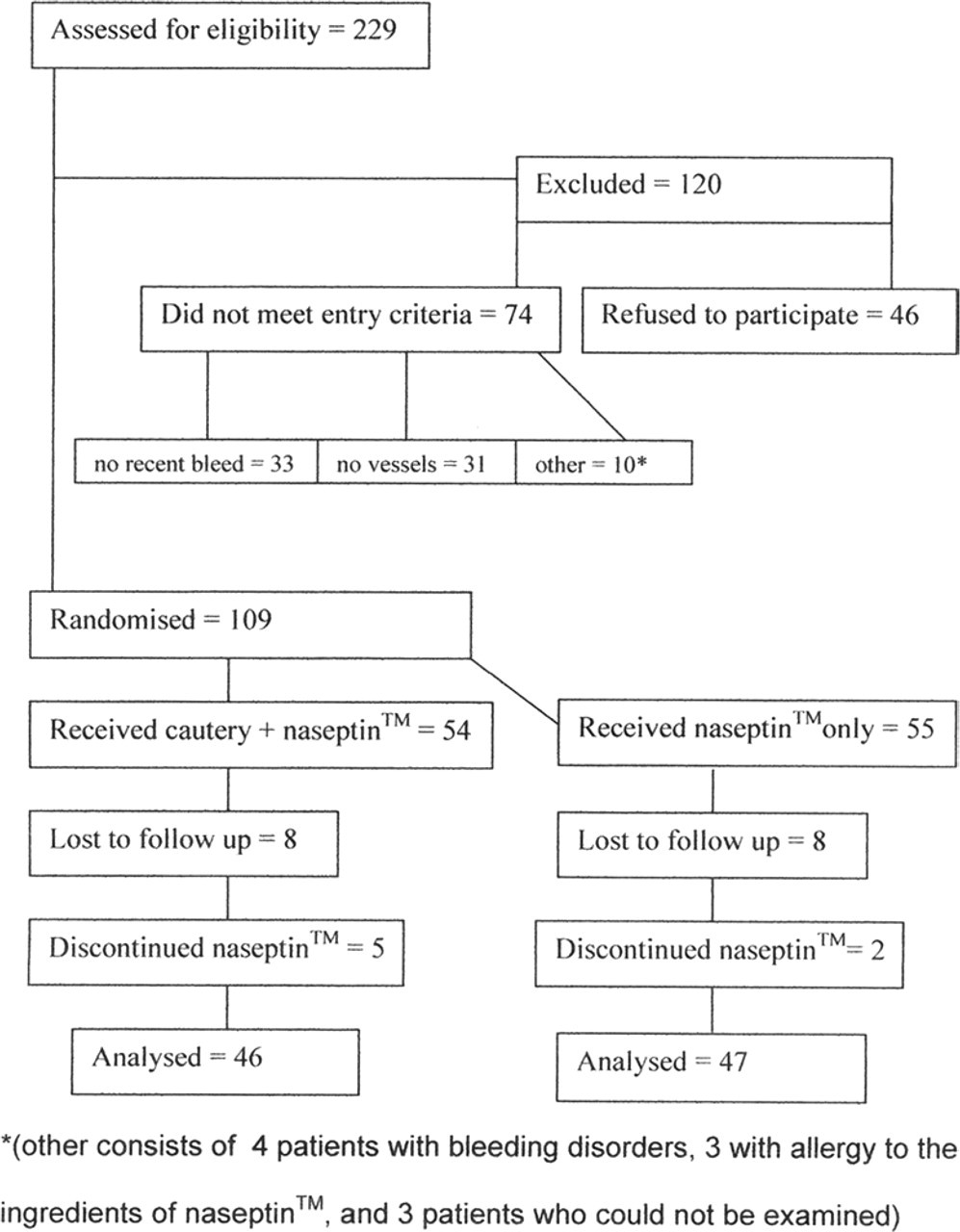
Consort flow chart.
Thirty-one children had no visible vessels on the septum and these children were not included in the randomized trial. They were simply given antiseptic cream and a follow-up appointment. Follow-up data are available on only 9 as there was a very high rate of nonattendance at the follow-up clinic.
An additional 4 patients were seen in clinic with epistaxis but were found to have suspicious nasal lesions on examination that required examination and biopsy under general anesthetic. They were excluded from the study and do not appear in the figures quoted above.
Cautery was well tolerated in children of all ages with only topical anesthesia. In the majority of cases, the cautery only took a few seconds and caused minimal discomfort. No child in the study required cautery under general anesthesia.
Outcomes
The analysis was done on an intention-to-treat basis, although cautery was completed in every case where it was attempted, so every child was actually treated as randomized. Parents admitted that 5 patients in the treatment group and 2 in the control group were not compliant with the full course of antiseptic cream.
The primary outcome measure used was no reported bleeding in the 4 weeks before follow-up. The difference in complete resolution rates between the treatment and control groups was not significant (21 of 46 [45.7%] treatment group vs 14 of 47 [29.8%] controls; χ2 = 2.49; P = 0.114). The secondary outcome measure was an improvement in symptoms (frequency and severity of bleeds) that for most children meant that no further treatment was required. Forty-two (91.3%) of 46 in the treatment group had an improvement in symptoms compared with 33 (70.2%) of 47 controls (χ2 = 6.626; P = 0.01; RRR = 71%; NNT = 4.7; 95% CI for NNT 3.2 to 19.3).
Many patients had crusting on the mucosa of the nasal septum that had to be removed before any vessels could be cauterized. Although those without crusting were more likely than those with crusting to have complete resolution of epistaxis within the active treatment group (16 of 27 vs 6 of 19), the difference was not statistically significant (P = 0.121).
Adequacy of Blinding
We attempted to blind patients to treatment allocation by performing sham cautery with the inactive end of the caustic applicator in the control group. This was successful in most cases although a small number (less than 15, although the exact number was not recorded) of older patients or parents spotted that “the wrong end” of the applicator had been used.
Outcomes assessment was done in clinics held on different days and with different surgeons from the enrolment clinics, so that the assessor was blind to the original treatment allocation. This blinding was compromised on 3 occasions: twice when the patient told the researcher which group they believed they were in and once when the code was broken because the patient was having problems with worsening bleeding.
Adverse Events
There was one reported minor adverse event, namely a patient who developed a rash and stopped taking the antiseptic nasal cream. There were no reported adverse events associated with cautery other than transient minor discomfort.
Discussion
In children with visible septal vessels, silver nitrate cautery gives a small additional benefit to antiseptic cream alone. Although some minor bleeding continued in both groups, the majority of patients whose symptoms improved (secondary outcome measure) had only one or two minor bleeds in the 4 weeks before follow-up and needed no further treatment. The number needed to treat was 4.7, which, we would argue, represents an effect that is clinically worthwhile, albeit only just.
The two previous trials 8 , 9 that compared antiseptic cream with nasal cautery showed no statistical difference between the two treatments. However, these two studies had smaller numbers of participants (48 in Ruddy et al 8 and 64 in Murthy et al 9 ), and only Ruddy et al 8 looked at an exclusively pediatric population. Both studies used nasal cautery regardless of the presence of visible vessels on the septum. Neither of these trials had a placebo control as in our study. We feel that our study adds to this existing small body of literature by having an improved design (double blinding, tighter inclusion criteria, bigger numbers, comparison with sham cautery) and by demonstrating for the first time a small but significant benefit from cautery.
It is impossible to draw any conclusions from this study as to the outcomes in patients without visible septal vessels as the follow-up rates were too low to make any meaningful statistical analysis. We excluded them from the randomized trial on the grounds that cautery, although logical for those with vessels, could be counterproductive in children where crusting is the main problem, as it could simply lead to more crusting. It has been our experience that these children respond well to antiseptic cream alone. We encountered fewer children without visible vessels (21%) than expected from previous studies: 50 percent in Kubba et al 6 and 53 percent in Loughran et al. 7 This may explain the lower response rate to antiseptic cream alone in the control group in this study compared with the previous ones, especially since the trials have all been conducted otherwise in very similar ways.
Most patients were followed up approximately 2 months after initial treatment, but as some did not attend or cancelled this appointment, the follow-up consultation (or telephone call) was more than 2 months later. This is a potential source of inaccuracy with the results as we accept that with prolonged periods of follow-up patients may have spontaneous resolution of their symptoms or indeed have recurrence after successful treatment. As has been shown in a previous study on long-term follow-up after treatment for epistaxis from this institution, 65 percent of patients were having nosebleeds again after treatment for epistaxis,12 so a prolonged period before follow-up may lead to a recurrence of symptoms. With the high rate of patients who did not attend appointments, this problem is difficult to combat. The nonattendance rates were the same in both the treatment and control group, and in both groups were lower than for patients not included in the study.
We also accept that there is a potential source of bias as some parents whose children had previously received antiseptic cream declined entry into the study because they wanted nasal cautery. Some patients who may have benefited from antiseptic cream alone were therefore excluded. This potential bias is balanced out by those parents who declined entry into the study because they definitely did not want nasal cautery.
The number of patients enrolled in the study was based on a power analysis with figures from two previous trials in our unit. Our estimates proved to be inaccurate, however, as the resolution rate in the cream-only (control) arm was much lower than in previous studies. A post hoc power analysis shows that with 46 and 47 patients in the arms and a resolution rate with cream of only 30 percent, the study has a 70 percent power to exclude a difference of 25 percent (ie, 55% resolution in treated group). This shows that this study was underpowered. In order to achieve more meaningful results, much larger numbers would be needed. This raises issues of practicality as it can be difficult to maintain recruitment over very long periods of time, or to raise the enthusiasm and funding required for large multicenter studies for unglamorous and non–life-threatening conditions such as epistaxis.
Conclusion
Most patients improve with either treatment modality (antiseptic cream alone or antiseptic cream with cautery), but less than half have complete resolution of symptoms at 8 weeks. Silver nitrate cautery with antiseptic cream twice daily for 4 weeks appears to give a small but clinically and statistically significant benefit when compared with antiseptic cream alone when measuring improvement in symptoms. This study provides some evidence in favor of the use of silver nitrate cautery in the management of recurrent pediatric epistaxis where there are visible septal vessels.
Author Contribution
Financial Disclosure
None.
Footnotes
Acknowledgements
The authors thank Sarah Casey, Department of Pharmacy, Royal Hospital for Sick Children, for preparation of the Naseptin prescriptions and Muhammad Shakeel, MRCS, for assistance in data collection.