
Abstract
Several rehabilitative maneuvers have been applied in the management of patients with swallowing disorders. 1 - 5 A tongue-holding maneuver (THM) was reported by Fujiu et al 6 to have a potential for compensatory anterior movement of the posterior pharyngeal wall (PPW) during swallowing, and they recommended it as a good maneuver for the rehabilitation of patients with dysphagia. To the best of our knowledge, however, there has been only one preliminary report examining the effect of the THM by comparatively measuring the pharyngeal pressure using a manometer with only two channels, and the study was performed on only three patients with head and neck cancer. 7
The advent of high-resolution manometry (HRM) came with the development of micromanometric water-perfused assemblies with 36 sensors in 2006. 8 At the same time, advances in computer technology allowed the large volume of data acquired by HRM to be presented in real time not only as conventional ‘line plots” but also as “spatiotemporal plots” (sometimes referred to as “contour” or “topographic” plots) that display the direction and force of esophageal pressure activity. Esophageal HRM is now being used not only for research but also in clinical practice. 9
This study aimed to investigate the effects of the THM during swallowing along the velopharynx and upper esophagus of normal Japanese adult subjects using this system.
Subjects and Methods
Subjects
We evaluated consecutively 33 healthy Japanese volunteers (19 men and 14 women) without history of dysphagia, gastrointestinal symptoms, upper gastrointestinal tract surgery, or any other significant medical condition. Their ages ranged from 22 to 46 years with the average of 26 ± 5.0 (mean ± standard deviation). The study protocol was approved by the Institutional Review Board committee of Nagasaki University Medical Dental Hospital, and written informed consent was obtained from each participant.
HRM
A solid-state manometric assembly with a 4.2-mm outer diameter having 36 circumferential sensors spaced at 1-cm intervals was used (Sierra Scientific Instruments Inc, Los Angeles, CA). This HRM device uses proprietary pressure transduction technology (TactArray, Pressure Profile Systems, Inc. Los Angeles, CA) that allows each of the 36 pressure sensing elements to detect pressure over a length of 2.5 mm in each of 12 circumferentially dispersed sectors. The sector pressures are then averaged to obtain a mean pressure measurement, making each of the 36 sensors a circumferential pressure detector with the extended frequency response characteristic of solid-state manometric systems. Before recording, the transducers were calibrated at 0 and 100 mm Hg using externally applied pressure. The response characteristics of each sensing element were such that they could record pressure transients in excess of 6,000 mm Hg/s and were accurate to within 1 mm Hg of atmospheric pressure after thermal calibration correction. The data-acquisition frequency was 35 Hz for each sensor. All pressure measurements were referenced to atmospheric pressure. Time is on the x-axis, and distance from nostril is on the y-axis. Strength of the pressure is expressed by a series of colors from blue to purple as indicated on the left side color bar. When an examinee vocalizes “kakaka,” we can identify the location of the velopharyngeal muscle zone, mesohypopharyngeal muscle zone, and upper esophageal sphincter (UES) muscle (Fig 1). 10
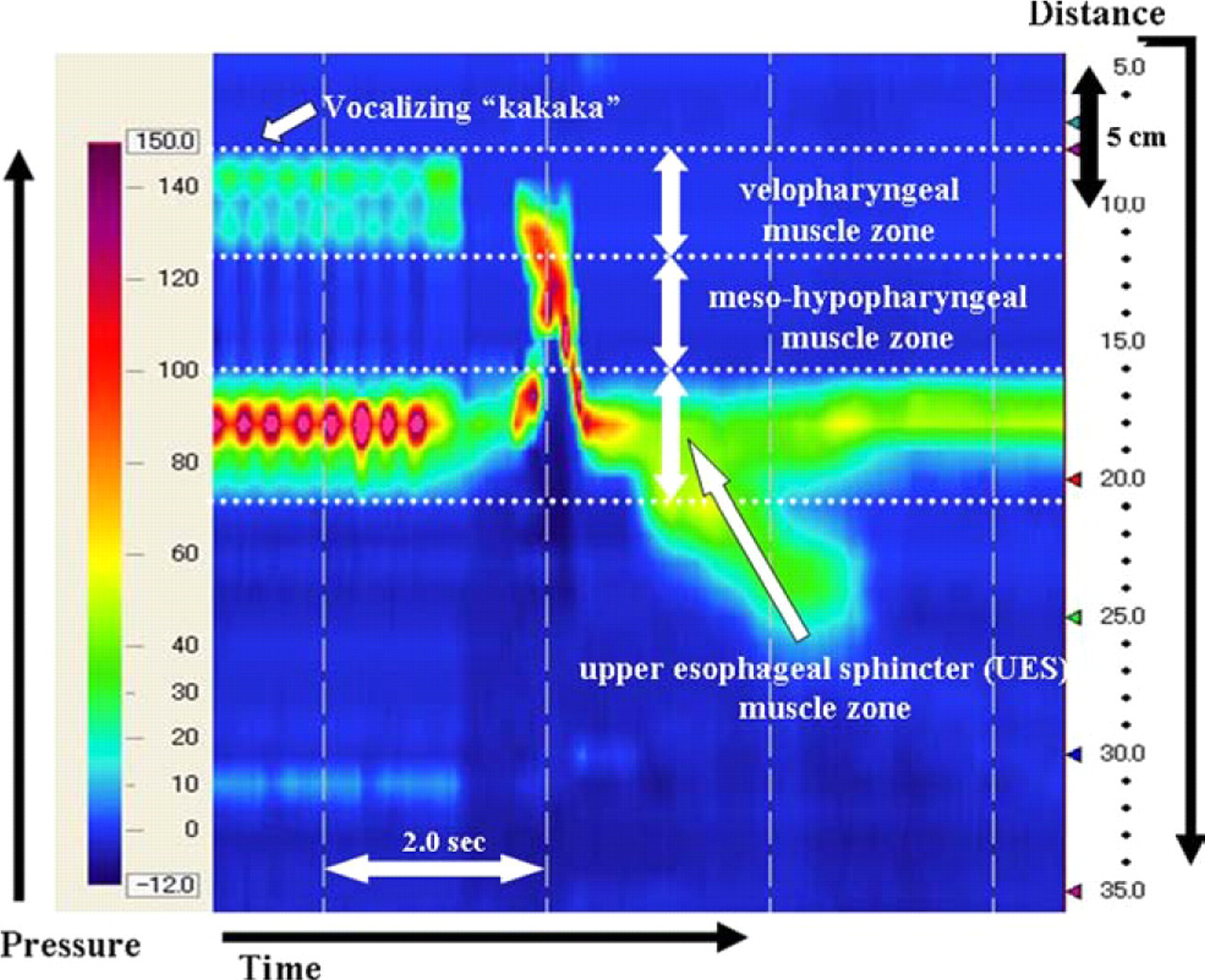
HRM depicts swallowing pressure activity from the velopharynx to the upper esophagus in the spatiotemporal plot.
Protocol and Analysis
After a brief interview and examination to ensure the absence of gastrointestinal symptoms, participants underwent transnasal placement of the manometric assembly in a natural supine position. Real-time pressure imaging during catheter intubation enabled accurate placement. The catheter was fixed in place by taping it at the nostril. For the THM, the examinees were asked to protrude their tongue anteriorly and hold it between the central incisors (Fig 2). Examinees were asked to swallow their saliva (dry swallowing) three times each with and without the THM, and the mean values were adopted.
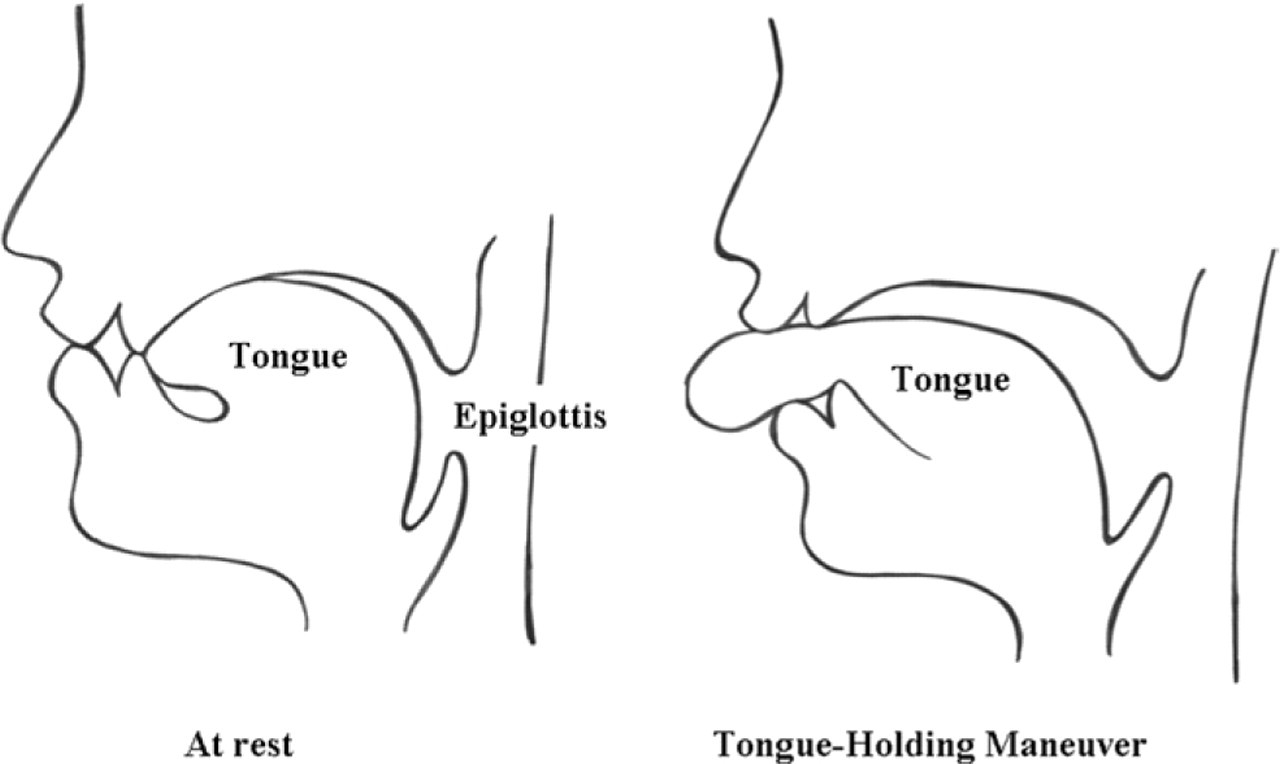
A schematic showing the tongue position and space of the pharynx at rest and during the THM.
Manometric data were initially analyzed by using ManoView analysis software (Sierra Scientific Instruments Inc, Los Angeles, CA). Using ManoView analysis software, we could easily obtain digital data of the pressure in millimeters of mercury and the distance in centimeters anywhere along the manometer. The maximum value of the swallowing pressure in any arbitrarily selected area (white square, the velopharyngeal muscle zone in Fig 3) and the distance from the nostril to the upper and lower margins of the area are shown in millimeters of mercury and centimeters, respectively.
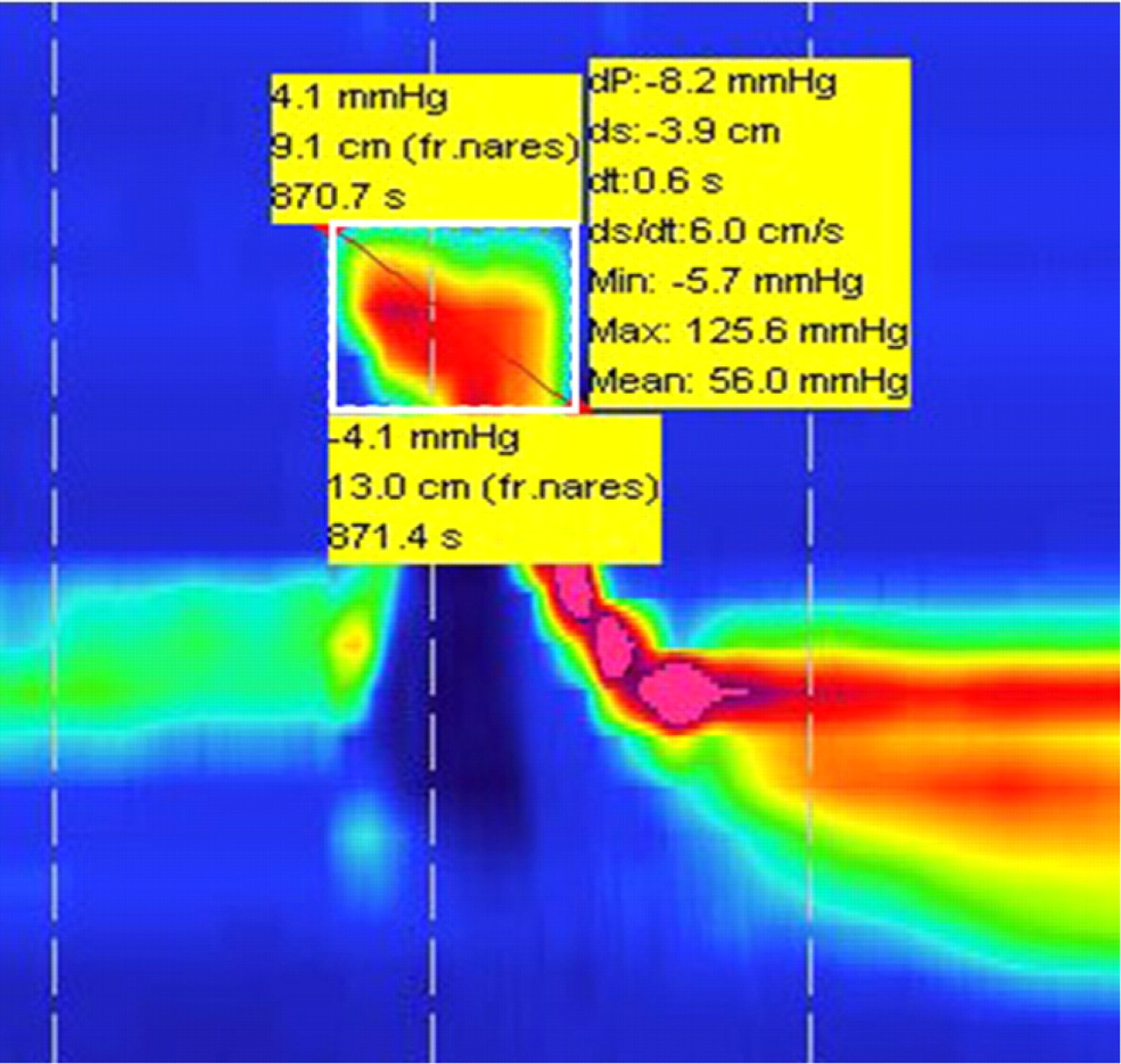
Using ManoView, the maximum value and the distance in any arbitrarily selected area (white square in this figure) are shown.
We used a repeated-measures analysis of variance to evaluate global differences of the maximum values of the swallowing pressures with and without the THM at the velopharynx, mesohypopharynx, and UES and a paired t test to evaluate the maximum values of the swallowing pressures and the distance from the nostril to each point of maximum values between groups with and without the THM. P values below 0.01 were regarded as significant.
Results
All results measured in the present study are summarized in Tables 1 and 2. The maximum values of the swallowing pressures with and without the THM were significantly different between at the velopharynx and at meso-hypopharynx and between the velopharynx and UES, respectively (P < 0.001).
Distances from nostril to maximum pressure point and P value of velopharyngeal, mesohypopharyngeal, and UES (cm) with and without the THM
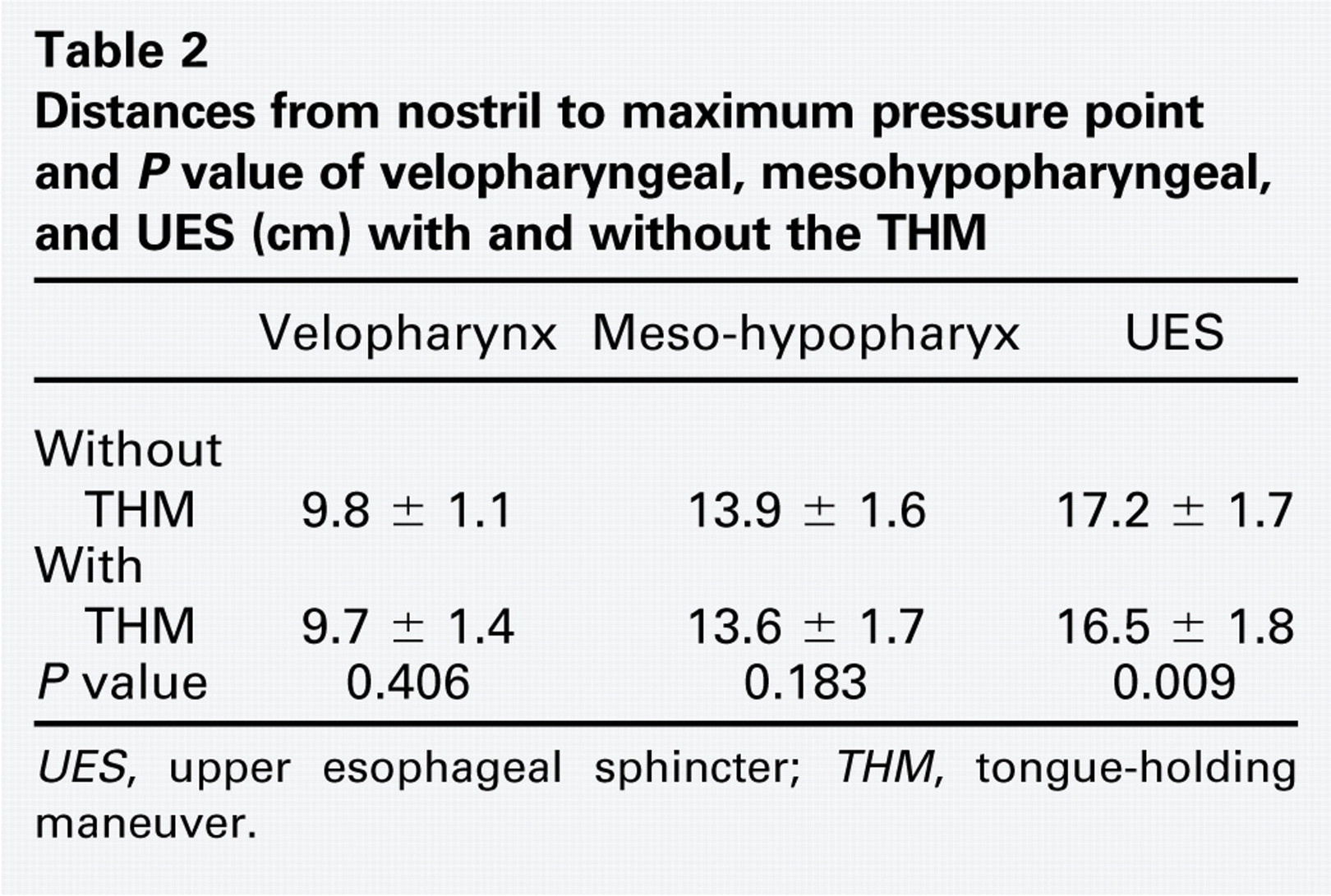
UES, upper esophageal sphincter; THM, tongue-holding maneuver.
Maximum values and P value of the velopharyngeal, mesohypopharyngeal, and UES pressures (mm Hg) with and without the THM
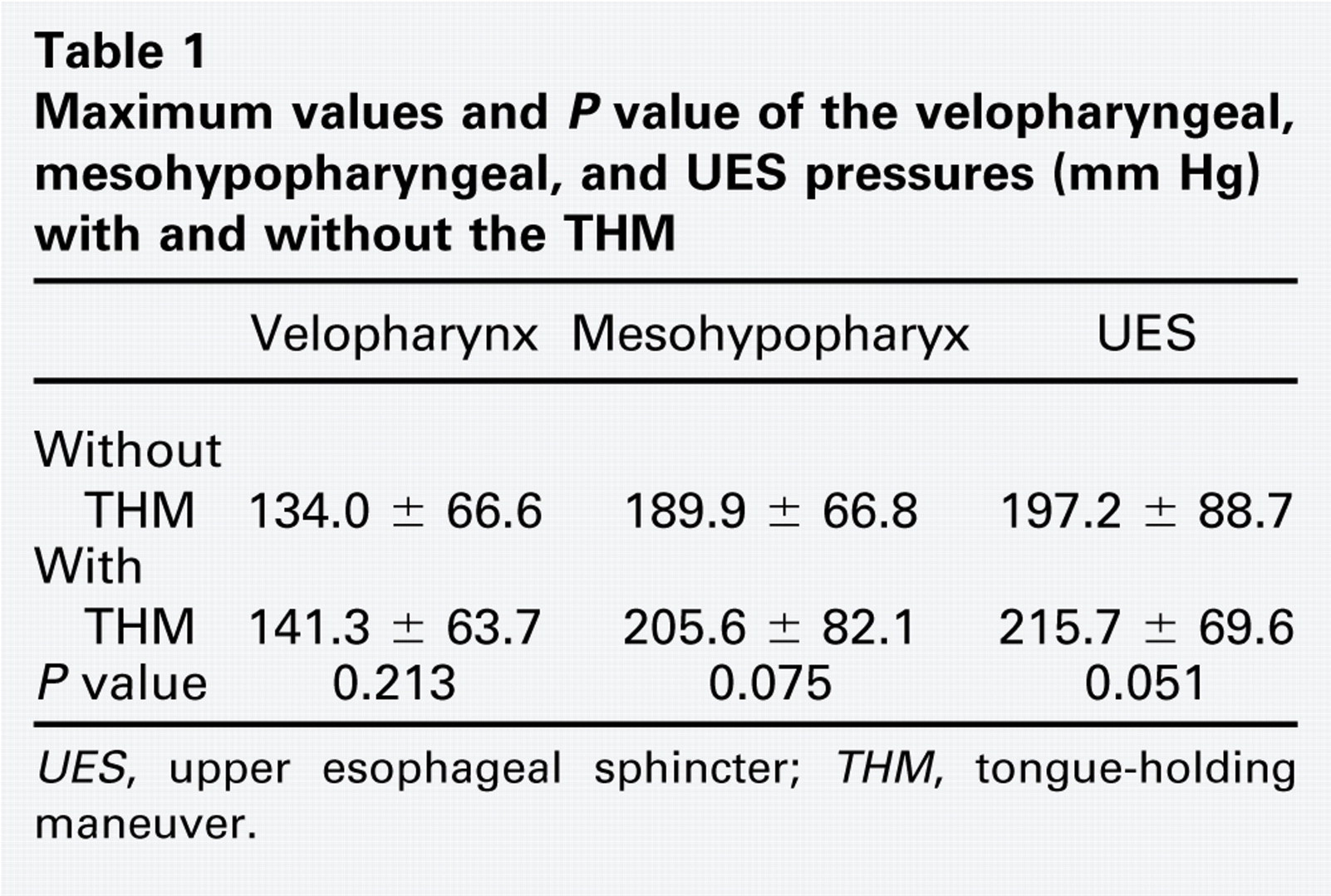
UES, upper esophageal sphincter; THM, tongue-holding maneuver.
The distance from the nostril to the UES was significantly shorter when swallowing with the THM than without the THM (P = 0.009). The maximum pressures at the mesohypopharynx (P = 0.075) and UES (P = 0.051) were greater when swallowing with the THM than without the THM, respectively. There was no difference in the pressures and the distance between swallowing with or without the THM at any other site.
Discussion
A THM is one of the maneuvers applied in the management of patients with dysphagia. 6 It was known that an increase in anterior bulging of the PPW has been observed videofluorographically in some surgically treated oral cancer patients during their postoperative course. 11 , 12 Fujiu and Logemann 6 reported that the anterior bulge of PPW during swallowing was significantly greater with the THM than without the maneuver at the level of the second cervical vertebrae (C2) or slightly lower level, which was the level of the mesopharynx.
The present study revealed different results from those of Lazarus et al. 7 The maximum swallowing pressure at mesohypopharyx did not show any significant difference with or without the THM, although the anterior bulge of PPW during swallowing with the THM is sometimes observed. This finding suggests that the anterior movement of PPW and the anterior movement of the tongue base with the THM may offset each other with the increase in swallowing pressure in the pharynx. We also found that the distance from the nostril to the UES, which was located at the level of the forth cervical vertebrae (C4) or slightly lower level, was shorter when swallowing with the THM than without the THM. The maximum value of swallowing pressure at UES was marginally higher with the THM (P = 0.051). These effects of the THM might be caused by a possible stronger influence of the THM on the lower pharyngeal constrictor muscle forming the UES than on the middle pharyngeal constrictor muscle. The elevated pressure at the UES might make bolus transit through this region more difficult. However, the present study provides clinicians with the possibility of actively changing the degree of muscular contraction of the UES, which has not previously been thought to respond to treatment for dyspharyngeal patients. Further study is required to clarify it.
The pressure changes in the pharynx during swallowing are more rapid than those of peristalsis within the esophagus because the muscles related to swallowing in the pharynx and upper esophagus are striated muscles. Thus, the pressure-measurement equipment for the pharynx and upper esophagus must have a very short response time. Some authors applied several maneuvers for the assessment and diagnosis of patients with swallowing disorders 2 - 5 using a conventional manometer with three or four sensors and/or videofluorometry. However, one of the possible problems that may take place when pharyngeal swallowing pressure is measured with a single-point sensor is that the elevation of the larynx during swallowing sometimes causes an unnatural spike-like increase of the pressure as a movement artifacts. To date, this has been one of the reasons that makes it difficult to study the characteristics and detailed mechanisms of swallowing along the velopharynx and upper esophagus using a conventional manometer. This may be one of the reasons why the present results were different from those of Lazarus et al 7 using a conventional manometer.
HRM has a high population and density of pressure sensors with circumferential sensing ability and is now being used not only for research but also in clinical practice in the esophageal region. 9 Using this device, we have already reported the maximum value of dry and water swallowing pressures at the velopharynx, mesohypopharynx, UES, and the distances from the nostril to each point and obtained important anatomic and physiologic information about normal swallowing along the velopharynx and upper esophagus. 10 However, there are few reports to observe the swallowing pattern with some rehabilitative maneuvers for patients with swallowing disorders in order to digitalize the effect of such maneuvers in normal individuals using this device. The present study revealed that the maximal pressure increased not at the mesohypopharynx as shown in the previous study 7 but at the UES. This may indicate a higher ability of HRM to collect more precise and detailed data than the conventional manometer. Thus, we may expect to obtain much important information about the swallowing physiology and pathophysiology along the velopharynx and upper esophagus using HRM in the future.
The present study was performed on a young cohort with a mean age of 26, and, therefore, these findings may not be generalizable to older persons. The THM may have a different effect on the elderly as they experience decreased pharyngeal pressures with aging. 13 Because most swallowing problems are more common in the elderly, we think that these results should be re-evaluated in an elderly cohort.
Conclusion
These findings suggest that the THM may not have a potential to facilitate compensatory swallowing power when swallowing. HRM will provide us with important information about the swallowing physiology and pathophysiology along the velopharynx and upper esophagus.
Author Contributions
Disclosures