
Abstract
With the incidence of obstructive sleep apnea (OSA) in infants and children approaching 0.69 to 2.9 percent, adenotonsillectomy has become one of the most common surgical procedures performed on children today. 1 - 3 Sleep apnea has been implicated in a number of sequelae including failure to thrive, chronic respiratory failure, cardiomegaly, developmental delay, and possibly sudden infant death syndrome. 4 - 6 Ample literature supports adenotonsillectomy as an accepted treatment for OSA in children. However, the surgical management of OSA in infants and children younger than 2 years has been controversial, likely owing to the belief that there is an increased incidence of complications. Although some authors have noted an increase in complications for children younger than 3 years, others have suggested that there is no increase in adverse outcomes with respect to otherwise healthy children younger than 2 years. 7 , 8 In contrast to the older pediatric population in whom adenotonsillar hypertrophy is the main cause of OSA, other etiologies such as craniofacial anomalies and neurological impairments are implicated at the infant and toddler ages. 9 Furthermore, it has been suggested by McNamara and Sullivan 3 that continuous positive airway pressure (CPAP) is an effective therapy for the management of OSA in infants, regardless of the site or mechanism of obstruction. Their study noted that most healthy infants eventually outgrow their need for CPAP. Infants with upper airway and craniofacial abnormalities require increasing amounts of pressure for treatment.
Adenotonsillectomy in infants and young toddlers is performed with increasing frequency. Objective data supporting improvement in OSA with this procedure is emerging. 10 Greenfeld et al 9 demonstrated clinical and symptomatic improvement in surgically treated infant OSA with respect to weight percentiles, parental questionnaires, and developmental delay. In a similar study, Shatz 11 concluded that failure to thrive and gastroesophageal reflux disease (GERD) improve considerably after adenoidectomy among infants. Selecting patients for surgical treatment may be difficult. Recent evidence shows that history and physical examination are poor predictors of OSA compared with polysomnography (PSG). 11 - 13 At our center, increasing numbers of infants and young toddlers undergo PSGs and thus are often diagnosed with OSA. Traditionally, adenotonsillectomy was reserved for patients 2 to 3 years old and older. Successful treatment in the infant and toddler age group measured by objective data is still evolving. In this era of evidence-based medicine and scrutiny by third-party payers, data for OSA treatment and complications in the infant and toddler age group is desirable. We wish to review our outcomes by analyzing pretreatment and posttreatment AHIs in both surgically treated patients and a medically treated control group. Safety and complication data will also be discussed.
Methods
This study was approved by the Institutional Review Board of the Indiana University School of Medicine. Our study was a case series with chart review of every pediatric patient younger than 24 months treated for OSA between 2000 and 2005 by two pediatric otolaryngology faculty members at James Whitcomb Riley Hospital for Children. Patients were identified by searching a departmental database for subjects with diagnoses of OSA, sleep disordered breathing, and adenotonsillar hypertrophy (International Classification of Diseases, Ninth Revision codes 780.50, 780.56, 780.57, 474.10, 474.11, 474.12). A search for all patients younger than 24 months treated by adenotonsillectomy, adenoidectomy, and tonsillectomy was also performed by using Current Procedural Terminology codes 42820, 42830, 42825, and 42835. It is routine practice at our institution that patients younger than 2 years undergo PSG for evaluation of OSA. All patients in the study were required to have a minimum of two PSGs (pretreatment and posttreatment for either medical or surgical treatment). Seventy-three patients who met inclusion criteria were identified. Patients were excluded if they had other concurrent airway procedures such as supraglottoplasty. Patients were also excluded if their postoperative PSG was less than 14 days post-procedure or greater than 20 months after surgery to minimize the influence of natural processes on the dynamics of PSG results. For patients who had multiple preoperative and postoperative PSGs, the studies performed closest to the date of surgery (outside of the 14 days) were used for comparison. Bovie electric cautery was used for tonsillectomy during the first half of the study. By the second half of the study, the faculty transitioned to Coblation tonsillectomy. Adenoidectomy was performed with either cold curettes or electric adenotome throughout the entire study.
The data collected included patient comorbidities, all available PSGs, and any major complications. Standard pediatric PSG parameters are measured at our institution including AHI, mean oxygen saturations, lowest desaturation, and mean and maximum end-tidal carbon dioxide (ETCO2). 14 - 16 OSA is defined as AHI greater than 1.0 in our center. Obstructive apneas are scored by noting continued chest or abdominal movement of at least two efforts without flow on the air flow and ETCO2 sensors. Hypopneas are scored by noting a decrease in airflow of 50 percent or more followed by either a drop in saturation of peripheral oxygen by 3 percent or greater, or an arousal. Obstructive hypopneas are characterized by paradoxical movement of the chest and abdomen. Central hypopneas are characterized by synchronous movement of the chest and abdomen. Events are not scored if they start during an arousal or awakening. At least one breath must separate an arousal from any subsequent events. OSA severity is generally classified as mild if AHI is less than 5 with absence of desaturation or hypoventilation; moderate if AHI is 5 to 10 with desaturation or hypoventilation present but not repetitive; severe if AHI is greater than 10 and presence of prolonged apnea with desaturation and hypoventilation. Major complications included respiratory distress (requiring intervention such as significant supplemental oxygen, nasopharyngeal airway, endotracheal intubation) and postoperative hemorrhage.
Changes in pretreatment and posttreatment AHI were analyzed. An AHI change score (defined as the initial AHI minus the follow-up AHI) was calculated for all patients in the surgical and medical groups. These values are presented with 95 percent confidence intervals (CIs). An independent t test compared the AHI change scores for the surgical group with those in the medical group. The mean difference between groups was calculated with a 95 percent CI. Comorbidities and complications of treatment were reviewed. Logistic regression analysis reviewed the effects of age, OSA severity (mild, moderate, severe), and comorbidities on complications. SPSS version 12.0 software for Windows (SPSS Inc, Chicago, IL) was utilized.
Results
Seventy-three children younger than 2 years met inclusion criteria. A total of 61 were surgically treated. Twelve patients were treated medically. The surgical modalities of treatment included adenotonsillectomy (n = 55), adenoidectomy (n = 5), and tonsillectomy in one patient with a prior adenoidectomy. Medical treatment included observation, oxygen, or CPAP (n = 12). The average age of the first PSG for all children was 336 days (11.2 months). The average age at surgical treatment was 507 days (16.9 months). The age range of surgically treated patients was 247 days (8.2 months) to 729 days (24 months). The mean interval of time between the preoperative and postoperative PSG was 222 days (7.4 months), whereas the mean interval between PSGs in the medically treated group was 186 days (6.2 months). For purposes of calculation, all months were given a standard value of 30 days.
The mean pretreatment AHI for the surgical group was 17.73, improving to a mean posttreatment AHI of 8.17. The medical groups mean pre- and posttreatment AHI values were 18.26 and 21.26 respectively. The mean AHI change score (initial AHI minus follow-up AHI) of the surgical group was 9.6 (95% CI, 5.8-13.4); the mean AHI change score of the medical group was −3.0 (95% CI, −15.1 to 9.1) (Fig 1). The mean difference in AHI change scores between the surgical and medical groups was 12.56 (95% CI, 2.7-22.4). An independent t test found this difference reached statistical significance (P = 0.013).
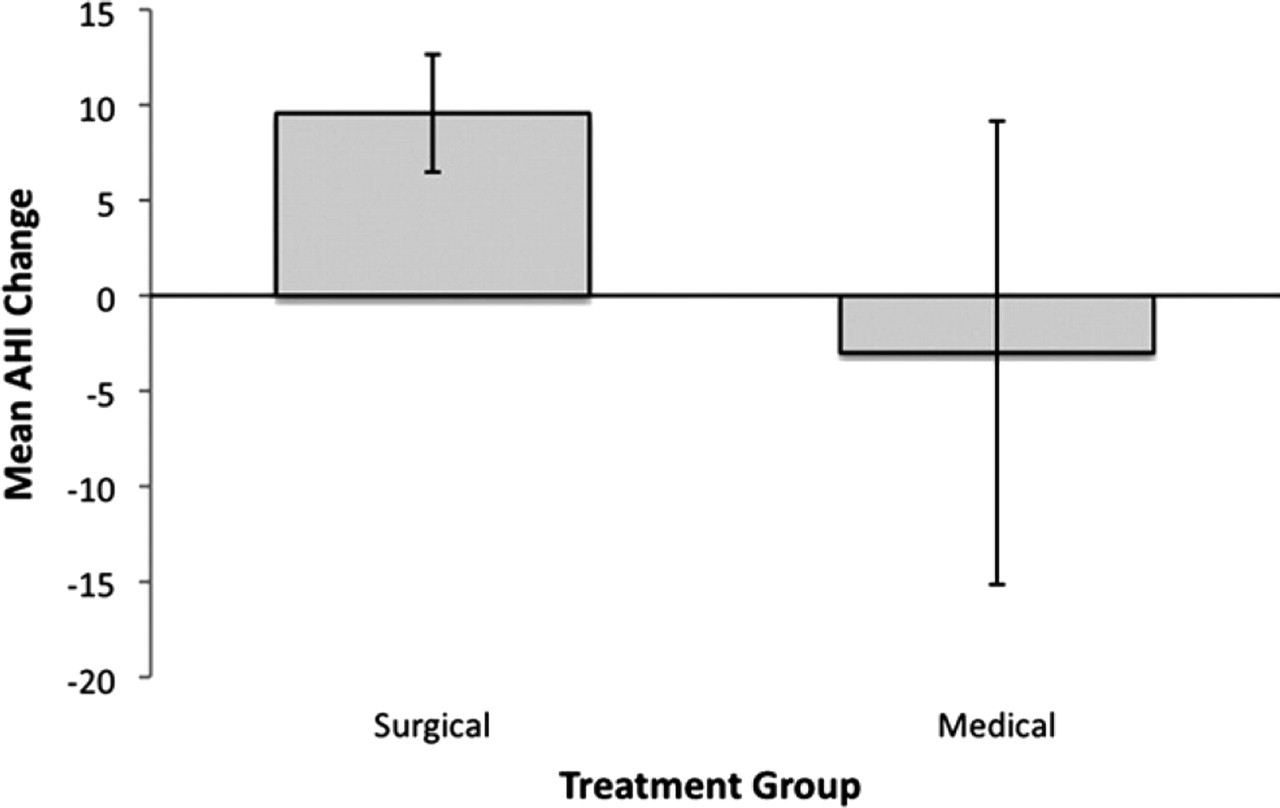
Mean AHI change (with 95% CI) for the medical and surgical groups posttreatment.
The number of patients with mild OSA, moderate OSA, and severe OSA (as defined earlier) after surgical treatment was 21(34%), 23 (38%), and 17 (28%), respectively. The number of postoperative patients with AHI < 1 and AHI < 3 was 0 and 7 (11%), respectively. The number of surgically treated patients with 50 percent reduction in AHI was 28 (46%), whereas those treated medically was 2 (17%).
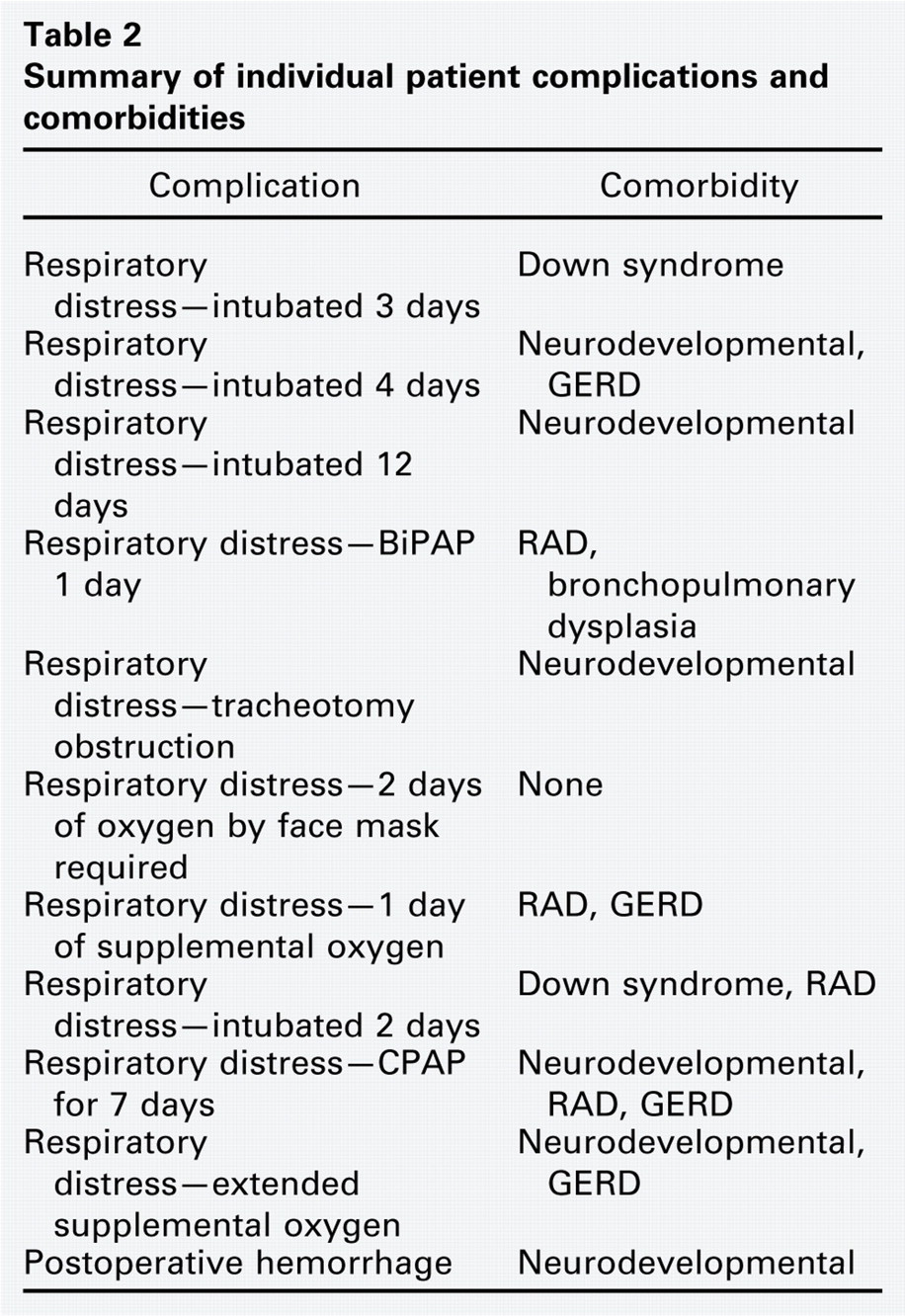
Eleven (18%) patients suffered significant postoperative surgical complications. These included postoperative respiratory distress (n = 10) and delayed postoperative hemorrhage (n = 1). Patients had varying degrees of respiratory distress: four requiring intubation for a period of 2, 3, 4, or 12 days; three requiring oxygen for up to 2 days; one patient requiring bi-level positive airway pressure (BiPAP) for 1 day, and one requiring CPAP for 7 days. One patient required replacement of a tracheotomy tube because of crusting in the tube lumen, which caused airway obstruction. This particular patient had a very small indwelling tracheotomy tube initially placed for severe OSA and received tonsillectomy and adenoidectomy to facilitate future decannulation. Nine of the 10 patients with postoperative respiratory distress had a preoperative AHI > 10 on their PSGs, with a mean of 27.5 and a range of 8.7 to 56.8. The single patient with delayed postoperative hemorrhage had mild bleeding controlled with cautery in the operating room but did not require blood transfusion. One additional patient had prolonged hospitalization attributable to poor oral intake.
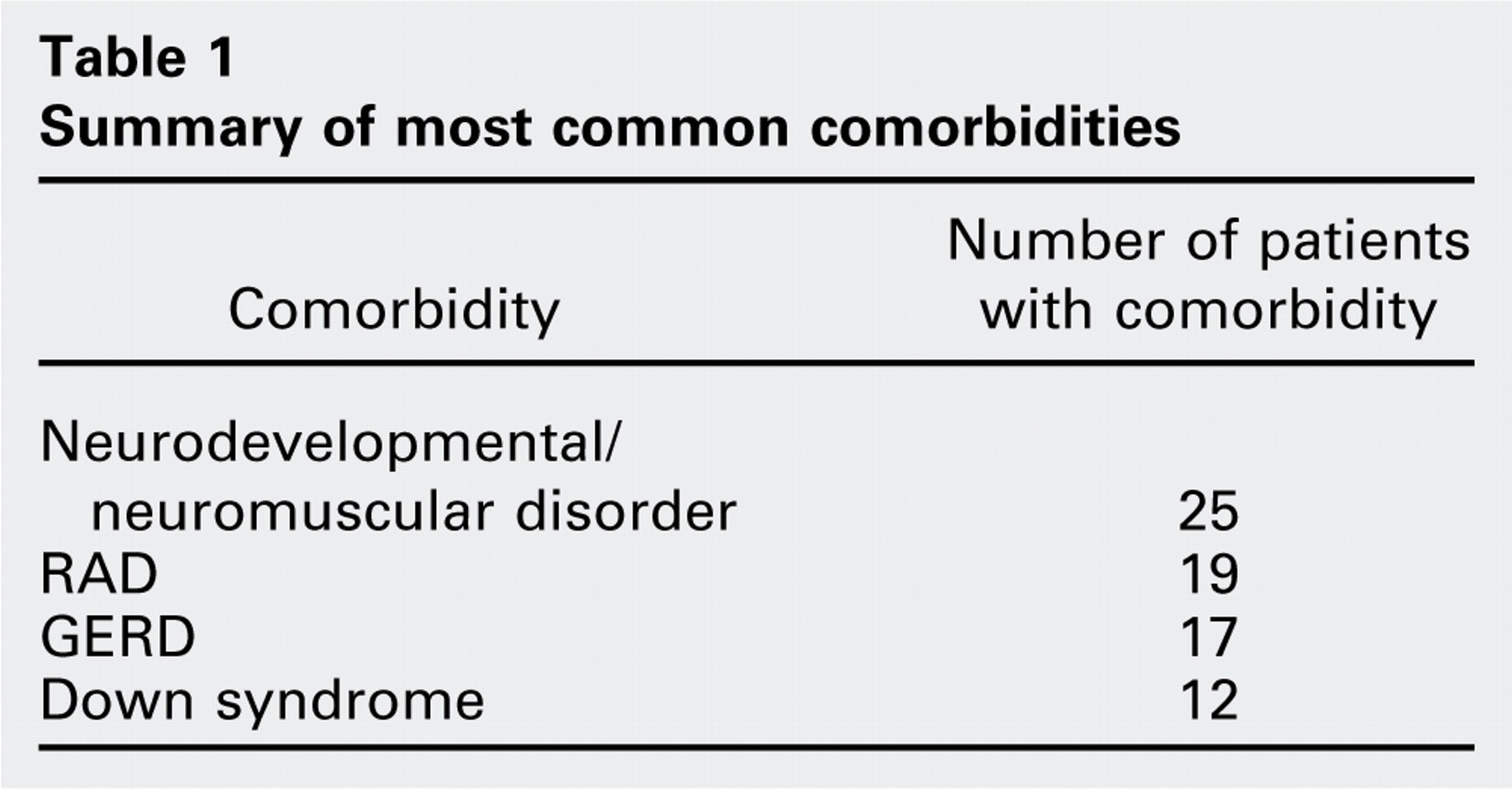
Sixty-three patients had comorbidities: 55 of the 61 patients treated surgically and 8 of the 12 patients treated medically. Ten (18%) of the 55 surgically treated patients with comorbidities had a postoperative complication, whereas one (17%) of the six patients without comorbidities had a postoperative complication. The most common diagnoses were reactive airway disease (RAD), GERD, Down syndrome, and other neurodevelopmental/neuromuscular disorders. Nineteen patients had multiple comorbidities. Down syndrome patients were considered a separate category of comorbidity. For the purpose of this analysis, the neurodevelopmental, cardiac, and other comorbidities of our Down syndrome patients were not counted individually under the other categories. The most common comorbidities and complications are listed in Table 1. The single postoperative bleeding complication mentioned previously was in a patient without comorbidity. To assess whether the likelihood of postoperative complications was due to age, severity of preoperative OSA, or comorbidities, we performed a binary multiple logistic regression analysis (SPSS version 16) using postoperative complication status as the binary (yes or no) dependent variable and the following predictor variables, which were entered into the model simultaneously: age at surgery, OSA severity, neurodevelopmental/neurosensory comorbidity, cardiac comorbidity, Down syndrome, RAD, GERD, any comorbidity, and multiple comorbidity. Individual patient complications and comorbidities are summarized in Table 2.
Summary of individual patient complications and comorbidities
Summary of most common comorbidities
The model did not significantly predict complication status (P > 0.1), suggesting that the risks of postoperative complications were not significantly affected by age, severity of OSA, or comorbidities.
Discussion
The group of 61 infants and young toddlers treated with surgical intervention for OSA had a significant decrease in AHI after intervention. The medical treatment group had no significant difference in posttreatment AHI. The findings of this study support previous findings by Greenfeld et al, 9 who observed an improvement among infants with OSA due to adenotonsillar hypertrophy after adenotonsillectomy. After surgical intervention, they observed an improvement in developmental delay, body weight percentile, and snoring. In contrast to the Greenfeld study, which excluded all children with craniofacial abnormalities, a large number of patients in this study had a variety of craniofacial abnormalities, syndromic features, and neurodevelopmental/neuromuscular disorders. In fact, 63 of the 73 patients in this study had significant medical comorbidities. Thus, our results may be more useful in validating the safety of surgical treatment in higher acuity, young, tertiary-center patients. Of course, AHI is not the only important data in OSA treatment. We chose this as our main outcome data because it serves as a single objective measure. Reviewing mean and maximum ETCO2, oxygen desaturation, mean saturation, and other parameters might be useful in the future.
The occurrence of respiratory distress as a surgical complication was high given that 10 (16.4%) surgically treated patients had this complication. Nine of these 10 patients had a preoperative AHI > 10 on their PSGs. These findings are similar to those found in a recent study by Slovik et al 7 in which OSA severity was identified as an important factor in determining the risk of postoperative respiratory complications in children younger than 2 years. Nine of the 10 patients with postoperative respiratory distress had comorbidities. However, in this study the proportion of patients with complications who had comorbidity was the same as the proportion of patients without complications who had comorbidity. This finding differs from what we predicted. We expected our findings would match those of Werle et al 8 who found that most patients requiring prolonged postoperative respiratory support had significant comorbidities. One would expect dehydration secondary to postoperative pharyngeal pain to be more common in very young patients after adenotonsillectomy. The patients most at risk for dehydration may have been the same as those suffering other complications. Thus, they received intravenous fluids during the management of those complications, avoiding dehydration. Additionally, the small size/power of this study may not adequately reveal the actual rate of dehydration. Our logistic regression analysis did not reveal which of the comorbidities may have the strongest effect on complications. This may be due to the small size of the study and multiple confounding factors.
It should be noted that none of the patients in our study group were cured of OSA with respect to objective data (AHI < 1). The range of AHI after both surgical and medical treatment was highly variable. We follow patients with persistent OSA in conjunction with our pediatric pulmonology colleagues. On the basis of severity of the PSG (moderate or severe OSA), risk of complications (cor pulmonale), and behavioral symptoms, CPAP may be considered. Other procedures such as tongue base reduction/ablation, orthognathic surgery, genioglossus advancement, and others considered for adults are still under study for pediatric patients and are infrequently used in our patients at this time. More mild residual OSA might be observed. Serial PSGs are often used with long-term pulmonology follow-up.
Limitations of this study include the small number of subjects in the control group and the inherent problems of a retrospective review. There was no randomization between patients receiving medical treatment and those receiving surgical treatment. We had difficulty finding patients treated medically for OSA. This may be an inherent bias of treatment at our center among our otolaryngologists and pediatric pulmonologists who refer the majority of these patients. The rationale for patients receiving medical treatment instead of surgery in our study was either documented in the chart as a lack of obstructive anatomical features, family preference, or clinical decision by otolaryngologist or pulmonologist for medical management. We acknowledge that a randomized, prospective study will be needed to provide further information.
Conclusion
This study sought to review our experience and to objectively assess the outcomes and safety of surgical treatment in young infants and toddlers with OSA. These data support surgical treatment and demonstrate that this approach may be taken with an acceptable complication rate in those with comorbidities. The surgically treated group of infants and young toddlers significantly improved in AHI after intervention. None of the patients in our study group were cured of OSA with respect to objective data (AHI < 1). The range of the AHI after both surgical and medical treatment was highly variable. Patients with persistent OSA as demonstrated on posttreatment PSG are followed long-term by our pediatric pulmonology colleagues. Further medical or surgical treatment should be considered on an individual basis given the clinical picture and posttreatment PSG results.
Author Contributions
Disclosures