
Abstract
Orbital floor fractures were first described by MacKenzie 1 in Paris in 1844. The term “blow out fracture” was coined in 1957 when Smith and Regan 1 described inferior rectus entrapment with attendant decreased ocular motility in the setting of an orbital floor fracture. The first attempts at orbital floor repair through a Caldwell-Luc approach date back to the 1970s as described by Walter. 2 This approach was abandoned for open approaches through the subciliary and transconjunctival approach because of the difficulty in maintaining fracture reduction and possible damage to the orbital contents. These open approaches, however, have been reported to have up to a 5 percent lower eyelid complication rate including scleral show or gross ectropion. 1
Although there is no agreed on approach to orbital floor repair, there is also no agreed on indication for repair. Burnstine 3 reviewed 20 years of literature on the topic of orbital floor fractures and developed a set of recommendations for repair of isolated orbital floor fractures. Based on his review, Burnstine described three time periods for repair: immediate, within two weeks, and observation. Immediate repair was recommended in cases of fractures with orbital soft tissue entrapment with a nonresolving oculocardiac reflex or early enophthalmos or hypoglobus with associated facial asymmetry. 4 Early intervention is also warranted in children with evidence of ocular muscle entrapment. This tissue entrapment can cause a “white-eyed” appearance and can lead to muscle or fat ischemia and resultant diplopia. Several studies in children have shown that earlier time to surgical repair yielded better clinical outcomes. 5 - 7 Surgical repair within 2 weeks is warranted in cases of symptomatic diplopia with positive forced duction testing, evidence of an entrapped muscle or perimuscular soft tissue on CT examination, and minimal clinical improvement over time. Large floor defects, greater than half of the orbital floor that are depressed with resultant enophthalmos, should also be considered for surgical correction. 3 Repair should also be considered if there is progressive infraorbital hypoesthesia. Finally, there are circumstances for which observation is appropriate. Patients with minimal diplopia, good ocular mobility, and no significant enophthalmos or hypophthalmos can be observed. Late correction, however, may not produce as good a result as early intervention.
In this article, we will review our favorable experience with endoscopic transantral repair of orbital floor fractures.
Methods
A case series with chart review was undertaken of all patients who underwent endoscopic orbital floor repair treated by the senior author (YD) from 1998 to 2007 in a tertiary referral private practice and county hospital. IRB approval was obtained. Subjects were gathered from the senior surgeon's facial trauma database. All orbital floor fracture patients who underwent endoscopic repair were included in this review. Demographic data, size and location of fracture, outcomes, and complications were collected from the chart review by both authors. Patients with an associated medial orbital wall fracture, displaced and fractured inferior orbital rim or significant zygoma, and Lefort II and Lefort III fractures that required open repair were treated with transconjunctival technique. This was to allow for direct plating of the rim and visualization of the greater wing of the sphenoid articulation in the lateral orbital wall to assess the adequacy of reduction of zygoma fractures.
Technique
After induction of general endotracheal anesthesia, 1 percent lidocaine with 1:100,000 epinephrine is injected in the upper gingivobulcal sulcus on the side of the fracture (Figs 1-5). A standard Caldwell-Luc approach to the maxillary sinus on the fracture side of the face is undertaken through a gingivobuccal incision. The window into the maxillary sinus is made with a fine side cutting drill bit after identification and preservation of the infraorbital nerve. The initial cut is made to preserve the medial and lateral maxillary buttresses. The fragment is removed in a kidney bean fashion to maximize size and possibly use as an autograft. The bone fragment is preserved in saline solution for possible future use. A combination of 0 and 30 degree endoscopes are used to view the fracture through the maxillary sinus. With the use of a modified curved elevator, the mucosa of the maxillary sinus around the fracture is elevated. The edges of the fracture are exposed. Any less than 1 cm fragments are removed. The curved elevator is now used to elevate the intraorbital periosteum for a distance of approximately 5 mm around and beyond the entire fractured segment. If the fracture is a simple trap door fracture, replacement of the bone in an anatomic location with overlap of the edges is attempted. If this is unsuccessful, the bone removed from the face of the maxilla can be used to repair the defect. If the defect should be larger than the bone harvested, a piece of titanium impregnated Medpor (Porex surgical, Newnan, GA) or other similar product can be used to fill the defect. The gingivobuccal incision is closed and no further packing is required. Postoperative antibiotics (1st generation cephalosporin or clindamycin) and continued for 5 days postoperatively.
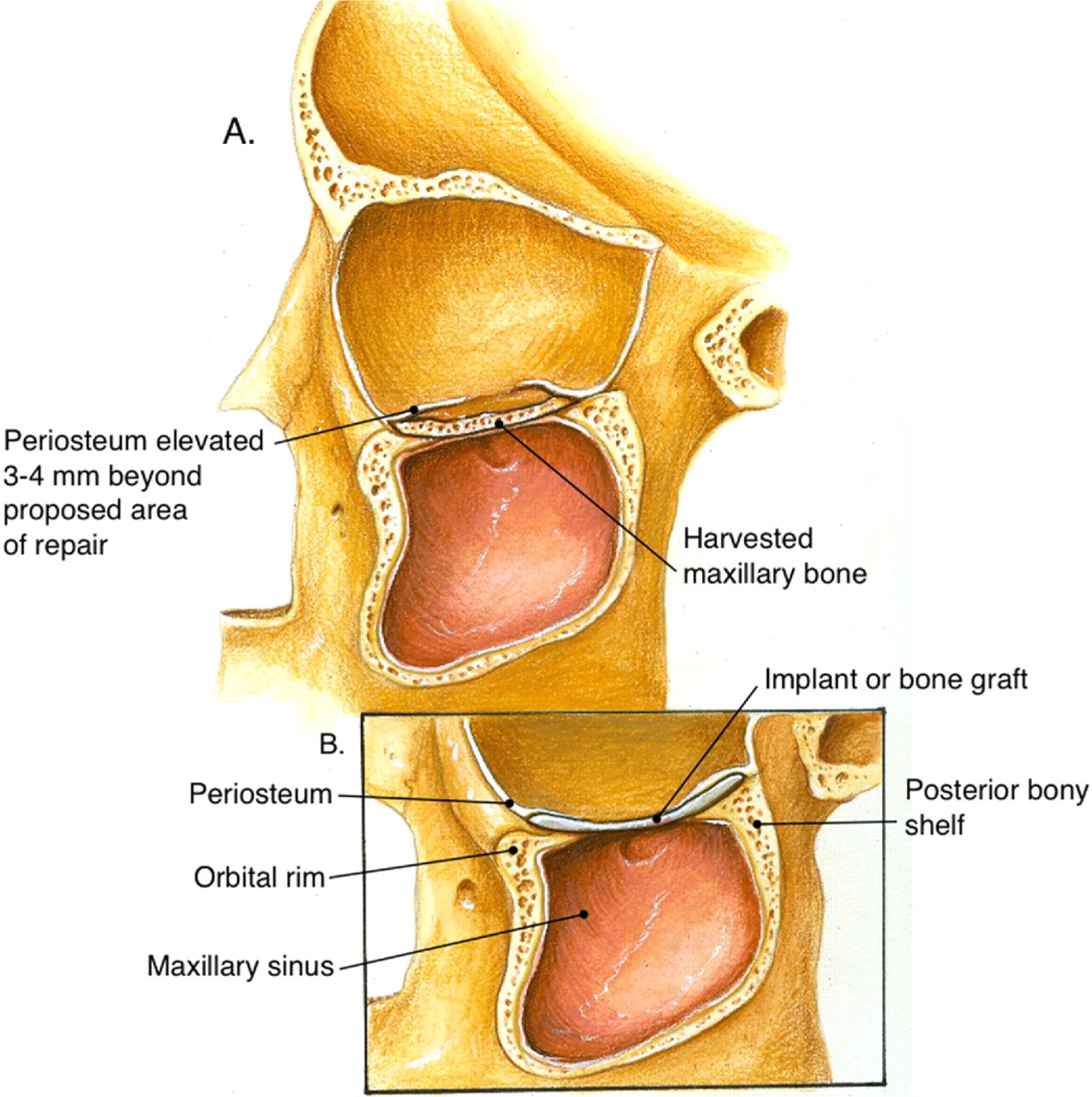
Fracture has been reduced and stabilized with autograft, alloplast or titanium.
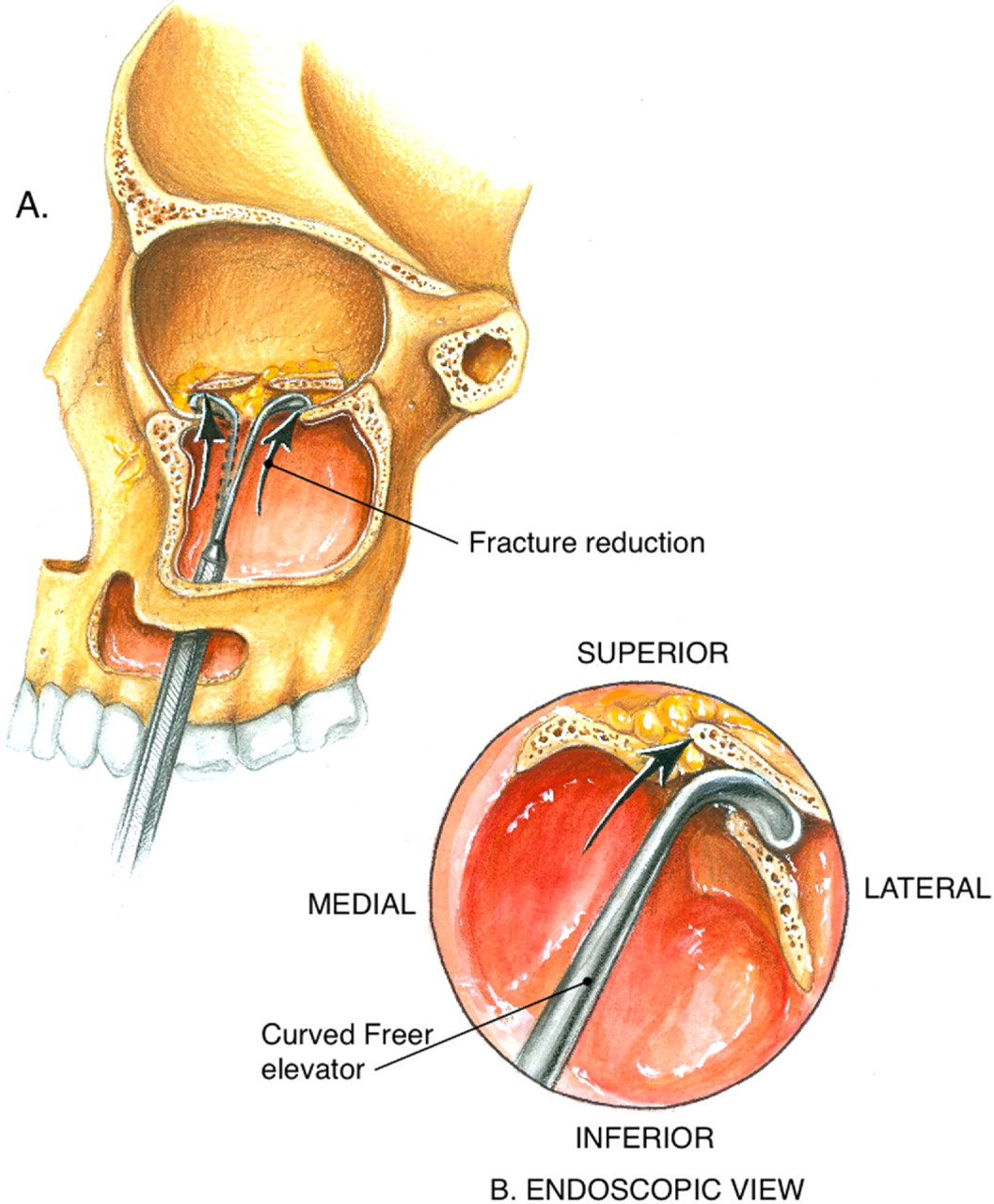
Herniated orbital contents are being reduced within the orbit from the transantral route.
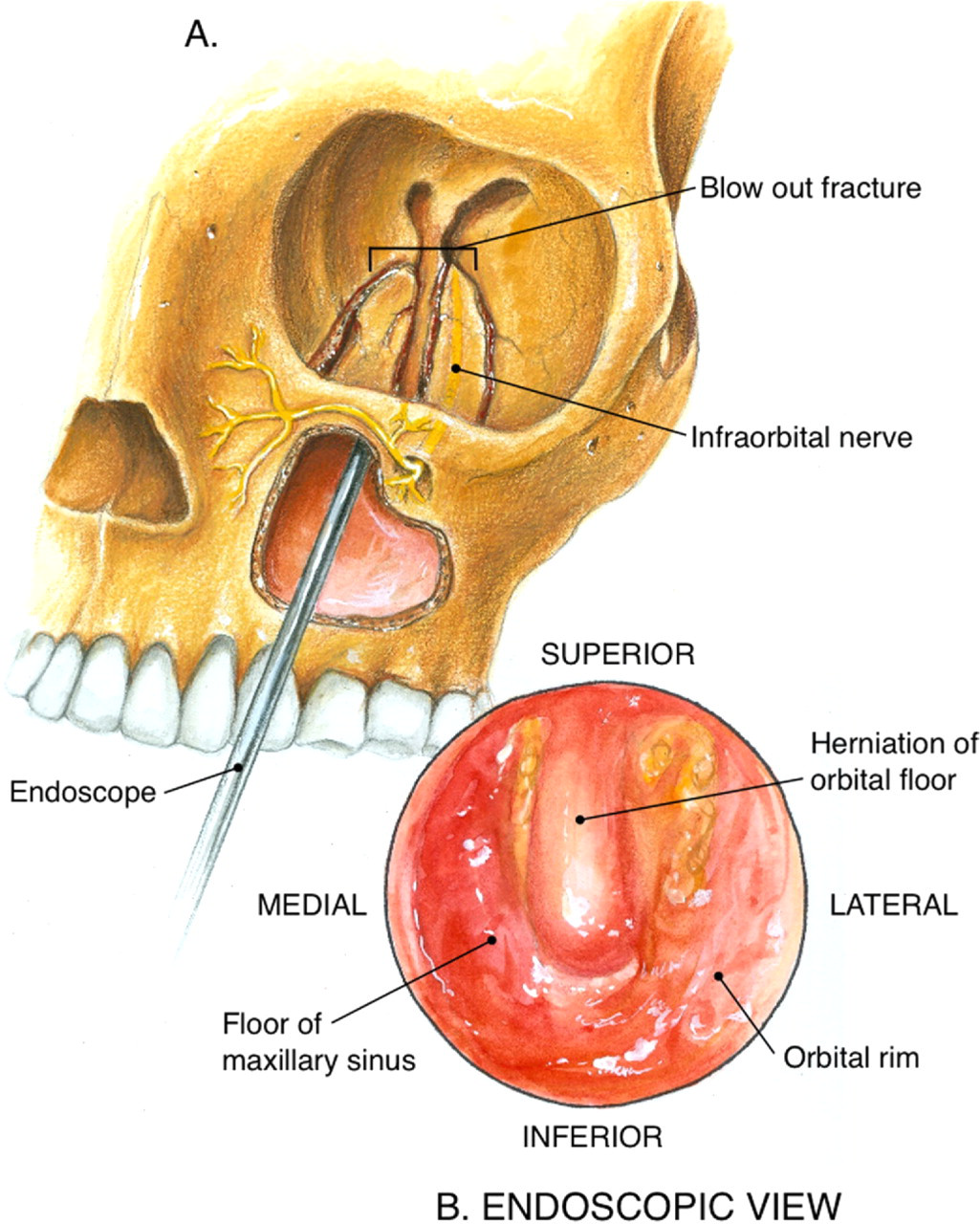
Endoscopic view illustrates herniated orbital contents.
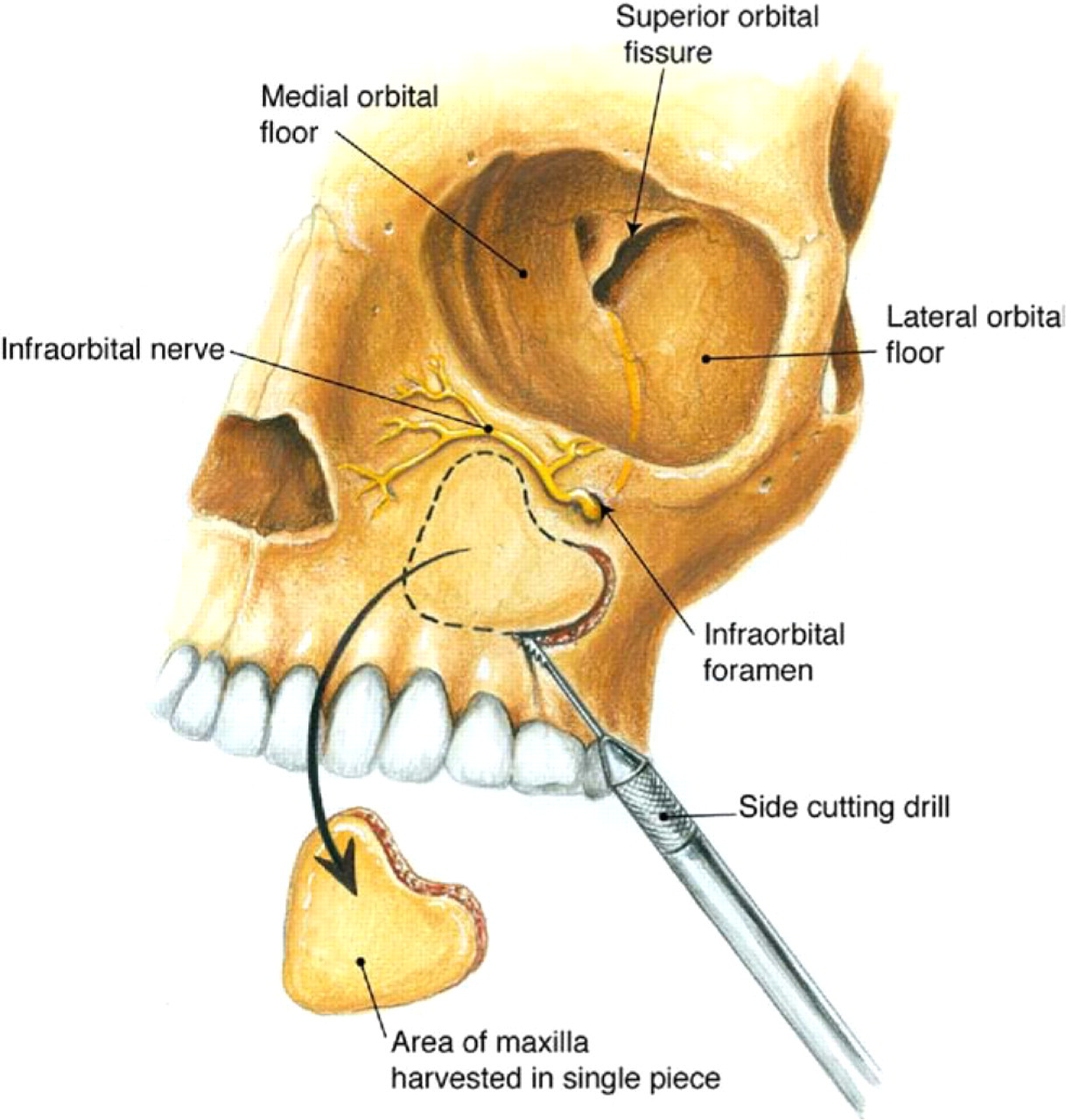
Removal of bone window is performed with a side-cutting burr taking care to preserve the medial and lateral buttresses as well as the infraorbital nerve. The window may be replaced, discarded, or used as an autograft for orbital floor stabilization per surgeon preference.
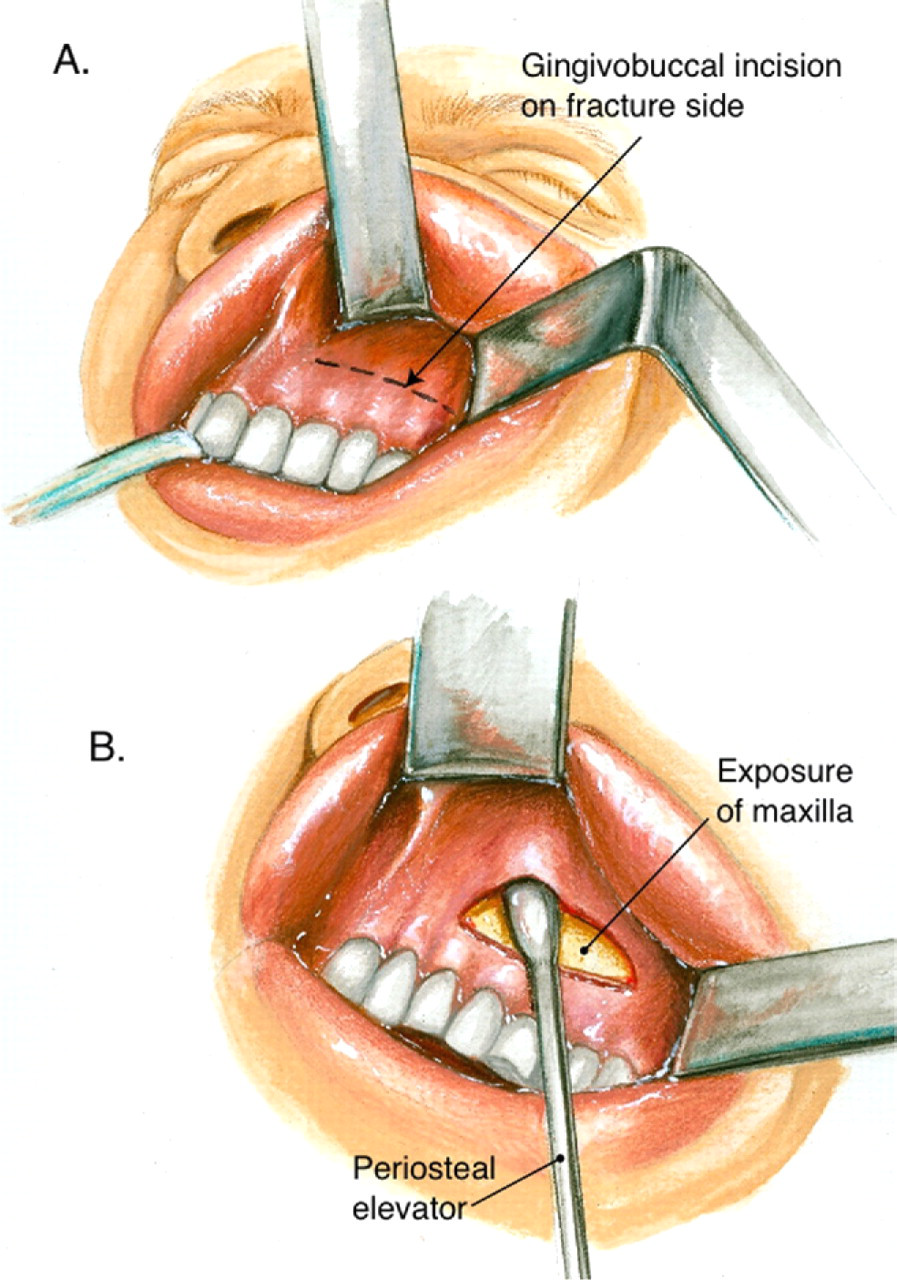
Upper gingivobuccal incision is made allowing exposure of the maxilla for osseous cuts.
Results
A total of 63 patients (44 male, 19 female) were treated with the described technique. Average age was 29.2 (range, 18 to 78 years). Thirty-nine patients underwent autograft placement from the anterior maxillary sinus wall harvest/exposure. Fourteen patients underwent placement of various alloplasts; the remaining 10 patients underwent reduction of the contents and floor repositioning. Two patients underwent repeat repair due to inadequacy of initial repair. Both were repaired endoscopically on the revision procedure. Both of these complications occurred in the subgroup of patients who underwent simple repositioning. No cases required conversion to an open approach. There were no cases of blindness, permanent new diplopia, ectropion, entropion, or new infraorbital anesthesia. No long-term sinus problems were encountered in our patient population although these may occur many years postoperatively and may not come to the attention of the facial trauma surgeon. We do not routinely use an antrostomy of any kind in this patient population as we have not had any significant problems with not using one.
Discussion
When a repair is undertaken, a decision as to approach must be made. The lower eyelid crease and subciliary incisions can leave unsightly scars and all have rates of ectropion ranging from 3 to 42 percent. 8 In addition, the transconjunctival incision has been reported to cause scleral show in 3 percent of cases. 9 Endoscopic approaches allow repair of orbital floor fractures without facial scars and without risk of ectropion. They also allow for immediate fracture repair without the need to await resolution of edema.
Several endoscopic approaches have been taken for repair. Ikeda et al 10 suggested the least invasive method was to use a urethral balloon catheter placed through an endoscopically opened maxillary sinus. 10 This results in an imprecise repair without fracture visualization. Others rely on an osteotomy in the anterior maxillary wall. 8 , 11 - 13 Materials for repair of the defect varied between the use of bone grafts made from the anterior maxillary wall osteotomy, 11 resorbable plates (poly L-lactic acid/polyglycolic acis, PLLA/PGA sheets), 8 silicon-Teflon-silicon balloons left in place for two weeks, 13 Medpor implants, 12 , 14 and titanium mesh placement. 15 All of these approaches seem to have excellent results with minimal postoperative morbidity.
With the advent of newer endoscopic instruments, older techniques for orbital floor fracture repair have become new again. Through a classic Caldwell-Luc incision, orbital floor repair can be easily undertaken. Risk of eyelid deformity is alleviated, and visualization of the fracture is greatly improved. This technique does have its limitations and cannot be used in cases where repair of the orbital rim must be undertaken as well as repair of the orbital floor. As noted, parethesia of the infraorbital nerve is still a risk, but in our experience was a transient occurrence. Only two patients required re-exploration, and no patients experienced any eyelid deformity after surgery. There were also no occurrences of persistent new diplopia.
Though there are several acceptable materials used to repair the orbital floor defect, we have found it best to be able to use the patient's own bone if possible. This avoids the risk of infection seen with implants and in theory promotes osseous integration over time though we have not performed an indepth illustration of this. If the patient's native bone is not sufficient, we believe titanium impregnated Medpor or similar material is a good alternative. The titanium implant allows for molding of the Medpor that allows for easier placement through the maxillary wall defect. This also allows for visualization on CT scan if a postoperative scan is necessary to evaluate for implant placement.
Traditional subciliary or transconjuctival techniques may allow for visualization of the entire orbital contents, even those lateral and medial to the fracture site. However, we do not feel this is generally important in fracture repair. Nevertheless, all patients have consented to a possible conversion to an open approach should this be required. Familiarity with traditional techniques needs to be maintained and taught to resident staff.
Conclusions
Endoscopic orbital floor fracture repair can produce excellent results without the risk of eyelid abnormalities seen with other open approaches.
Author Contributions
Disclosures