
Abstract
Obstructive sleep apnea (OSA) in children is characterized by snoring and sleep disturbance secondary to recurrent obstruction of the airway, and has been associated with a number of other health-related issues and behavioral problems. OSA is estimated to affect 1 to 4 percent of all children in the United States, 1 and has been increasingly recognized as a significant disorder warranting further evaluation and management. Traditionally, adenotonsillar hypertrophy has been thought to be the primary cause of OSA in children, and tonsillectomy and adenoidectomy (T&A) remains the preferred method for the surgical management of pediatric OSA in most patients.
With the increased use of preoperative and postoperative polysomnography, we now recognize that 10 to 20 percent of children will have persistent OSA following T&A. There are a variety of causes for this treatment failure, including primary lingual tonsillar hypertrophy (LTH) and secondary LTH, which occurs following T&A. 2 - 5 When the lingual tonsils have been recognized as the site of obstruction, lingual tonsillectomy has been the treatment; however, the traditional technique of lingual tonsillectomy has posed technical challenges due to access visualization and bleeding during tissue resection.
Here we describe our novel technique for the management of these difficult patients. This includes identification of lingual tonsillar hypertrophy by office and interoperative endoscopy as well as the technique of endoscopic-assisted coblation lingual tonsillectomy. The efficacy of this treatment for lingual tonsillar hypertrophy and persistent pediatric OSA will be discussed.
Methods
This study was approved by the Institutional Review Board of the Lucile Packard Children's Hospital, Stanford, California, and was conducted in compliance with the Healthcare Information Portability and Accountability Act. Medical records were obtained from all patients from June 2005 to January 2008 who were diagnosed with a persistent polysomnogram (PSG)-proven OSA despite prior T&A. Office flexible fiberoptic laryngoscopy was performed on each patient; if obstruction was suspected at the level of the lingual tonsils, the patient was then scheduled for flexible fiberoptic sleep endoscopy in the operating room. Sleep endoscopy was performed under spontaneous bag-mask ventilation, and the airway was inspected for dynamic collapse and obstruction at various levels from the nasopharynx to the larynx. If large lingual tonsils were identified and the airway demonstrated collapse at this level, the diagnosis of lingual tonsillar hypertrophy was made. The airway was further examined for any other synchronous levels of obstruction with microlaryngoscopy and bronchoscopy.
Endoscopic-assisted coblation lingual tonsillectomy was then performed. The technique is described in detail here. Lingual tonsillectomy requires nasotracheal intubation with the endotracheal tube secured gently to the forehead; care is taken to avoid pressure to the forehead as well as to the nasal ala. A dose of steroids (10 mg dexamethasone IV) is given. The surgical bed is then rotated 90 degrees. A Jennings mouth gag is placed to retract and open the mouth. A silk suture is passed through the tip of the tongue, and the tongue is retracted inferiorly. It is sewn under tension to a Mustarde table or Mayo stand that has been positioned much like it would be during a routine tonsillectomy and adenoidectomy. Additional exposure is achieved by retracting the palate with two red rubber catheters passed through both nares and secured with Schnidt clamps (Fig 1 A,B).
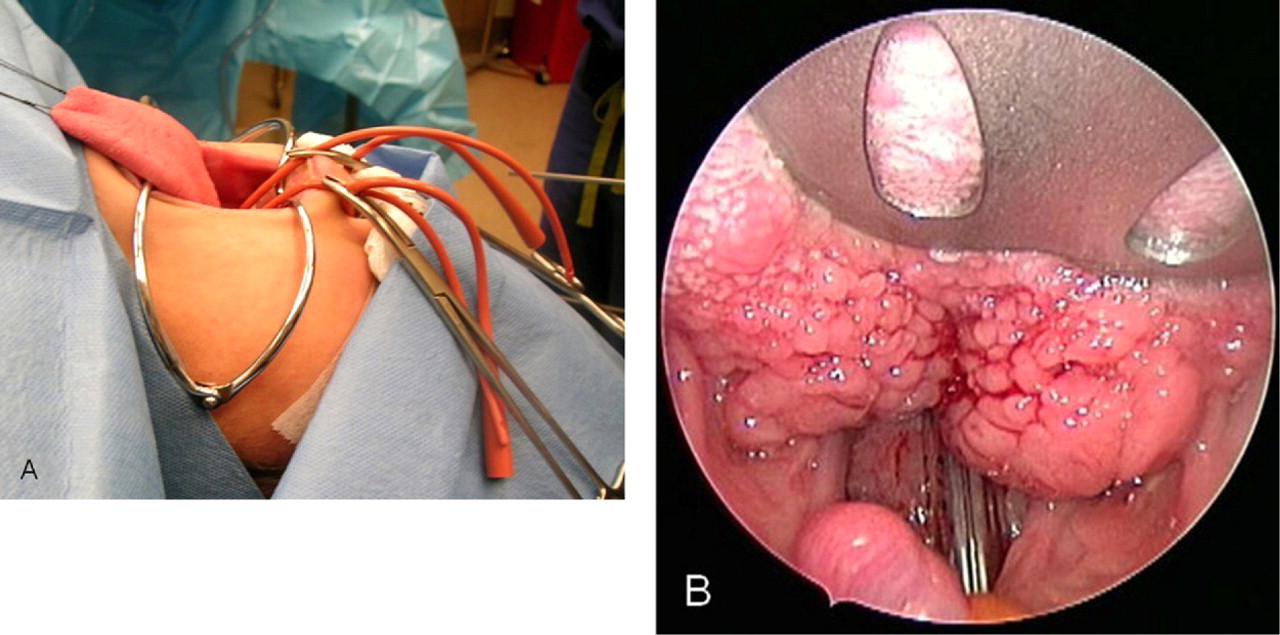
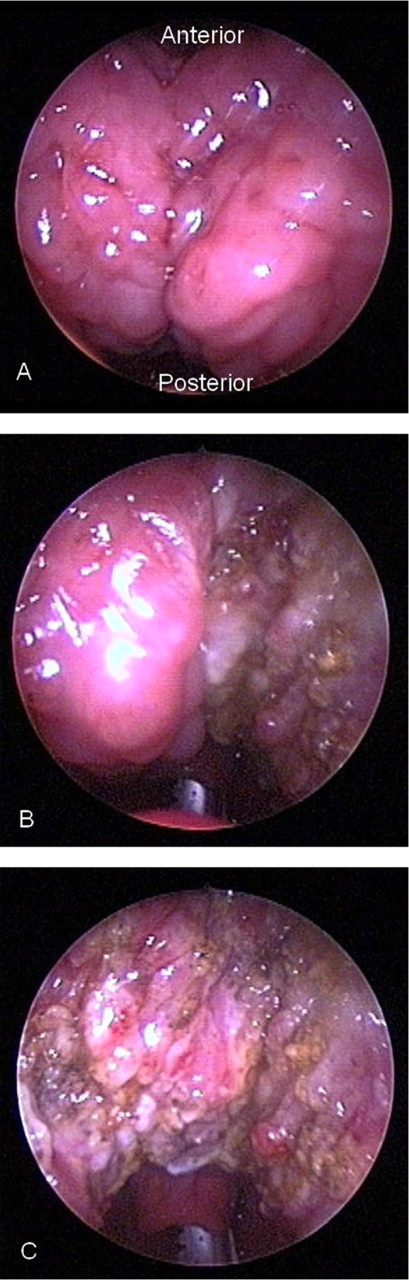
The surgeon stands at the head of the bed while the video tower is placed at the foot of the bed; as the procedure is endoscopic, a headlamp is not required. An assistant stands to the left of the bed and retracts the mobile tongue with a revised sweetheart retractor, utilizing the handle for retraction. This is a key component of the procedure, since it elevates the tongue base off of the posterior pharyngeal wall, facilitating full exposure of the vallecula and larynx. The surgeon passes a 4-mm 30-degree sinus endoscope into the oral cavity to visualize the base of tongue and lingual tonsils. A Coblator II Surgery System (ArthroCare ENT, Austin, TX) was used in this series with coblation settings of 8 and coagulation settings of 5. An EVac 70 coblation wand (ArthroCare ENT) is introduced into the oral cavity under endoscopic guidance. The lingual tonsils are then resected from superior to inferior from the circumvallated papilla to the vallecula. Any bleeding encountered is coagulated to prevent obscuring the endoscopic view. In most cases, the epiglottis is initially hidden by the lingual tonsils, but is later exposed as the lingual tonsils are coblated (Fig 2A-C). Care is taken to avoid injury to the mucosal surface of the epiglottis. While there is no clear demarcation between the lingual tonsils and the tongue musculature, the change in tissue quantities becomes readily apparent.
After coblation of the lingual tonsils and adequate hemostasis, the patient is taken out of retraction and extubated in the operating room. The patient is admitted overnight in a monitored hospital bed for observation. Postoperative antibiotics (amoxicillin) and pain medication are given. The patient is allowed to take a regular diet. If the child demonstrates good oral intake, he or she is discharged home the following morning.
In this study, the patients were asked to return for a follow-up visit a month after surgery. A postoperative PSG was then scheduled for three months later (four months postoperatively). Preoperative and postoperative PSG values (number of apneas, number of hypopneas, respiratory distress index [RDI], and minimum O2 saturation) were compared and analyzed statistically (two-tailed paired t test). A P value of <0.05 was considered significant.
The inclusion criteria for this study consisted of having PSG-proven OSA despite prior T&A, as well as documented lingual tonsil hypertrophy as seen by office and sleep endoscopy. Patients were excluded if preoperative and postoperative polysomnograms were unable to be obtained or if lingual tonsil hypertrophy was not thought to be the primary cause of persistent OSA after T&A.
Results
Twenty-six pediatric patients met the inclusion criteria for this study and had endoscopic-assisted coblation lingual tonsillectomies. All had persistent OSA despite prior T&A. Fourteen patients were male and 12 patients were female. The mean age was 11.0 years with a range from 3.4 to 20.6 years. Two patients were 19 years old or older and had syndromes requiring prolonged care at a pediatric care center; their treatment for OSA had spanned multiple years. The remaining 24 patients were 16 years old or younger. Twelve of the 26 patients (46%) had no comorbidities, while 14 of the patients (54%) had various disorders such as Down syndrome, Asperger syndrome, Beckwith-Wiedemann syndrome, and velocardiofacial syndrome. Two patients had isolated craniofacial anomalies.
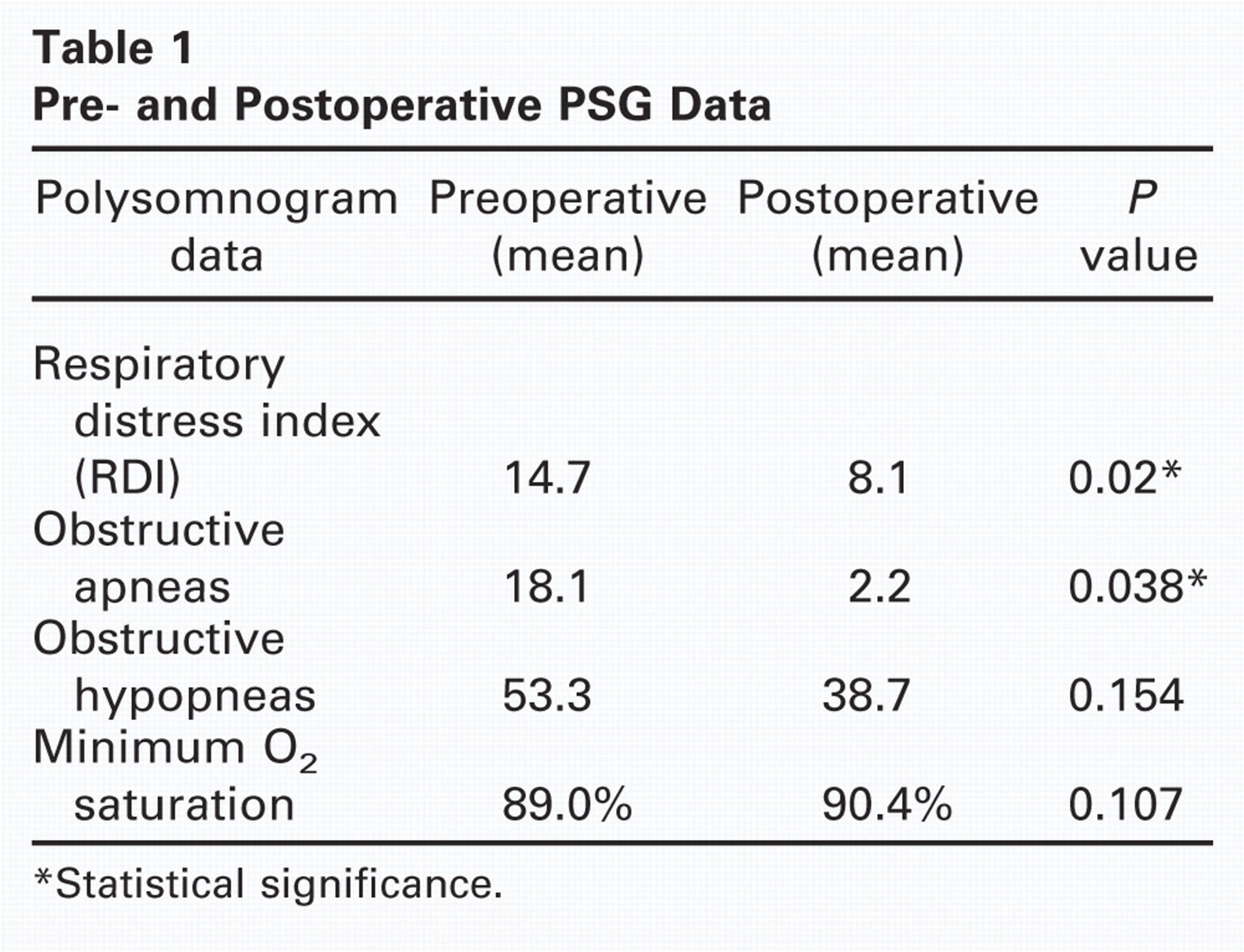
The mean preoperative RDI for these patients with persistent OSA was 14.7. After endoscopic-assisted coblation lingual tonsillectomy, the mean postoperative RDI was decreased to 8.1 (Table 1). This difference was significant (P = 0.020, two-tailed paired t test).
Pre- and Postoperative PSG Data
Statistical significance.
The numbers of obstructive apneas and hypopneas were compared. The mean preoperative number of obstructive apneas for these pediatric patients with persistent OSA was 18.1. After endoscopic-assisted coblation lingual tonsillectomy, the postoperative mean was 2.2. This difference was also significant (P = 0.038). The mean preoperative number of hypopneas was 53.3. The postoperative mean was 38.6 (Table 1). This difference was not significant, although a trend was suggested (P = 0.154).
The minimum O2 saturation was also examined. The preoperative mean for these patients with persistent OSA was 89.0 percent. This was in comparison to the postoperative mean, which was 90.4 percent (Table 1). This difference was not statistically significant (P = 0.107).
Discussion
Adenotonsillectomy is considered to be one of the most effective methods of alleviating OSA, yielding an average success rate of 80 percent as revealed by a recently published meta-analysis. 6 In clinical practice, a nocturnal PSG is frequently performed to establish the diagnosis of OSA before a T&A is performed, but this is not universal. However, the American Academy of Pediatrics recommends objective sleep testing prior to performance of T&A for OSA. 7 In children, the criteria used to diagnose OSA in children are variable, but in the strictest variation, OSA is diagnosed if more than one episode of apnea or hypopnea per hour is recorded. T&A is generally indicated when more than five episodes per hour are observed, or when the oxygen saturation falls below 90 percent at any time during sleep.
Factors that are known to contribute to treatment failure of T&A for OSA include craniofacial disproportion, hypotonia, oropharyngeal soft-tissue redundancy typically associated with obesity, laryngomalacia, and lingual tonsillar hypertrophy. In the past, these levels of obstruction have been difficult to identify with certainty in the young child. In addition, methods to treat these additional sites of obstruction have been limited. The use of flexible fiberoptic laryngoscopy, in the office as well as in the operating room, has aided the work-up of persistent pediatric OSA. Our ability to see dynamic collapse of the airway during flexible fiberoptic sleep endoscopy not only facilitates the identification of the site of obstruction during sleep, it also leads the otolaryngologist towards the potential treatment. Other diagnostic modalities such as cine MRI exist and may yet play a significant role in the work-up of persistent pediatric OSA. 8
Lingual tonsillar hypertrophy has been well described in the anesthesia literature as a potential area of airway obstruction. 2 - 5 The lingual tonsils and the base of tongue are particularly concerning in Down syndrome children with macroglossia and glossoptosis. 9 However, lingual tonsillar hypertrophy and its treatment in otherwise healthy children has not been previously described. In this series, 46 percent of the patients diagnosed with lingual tonsillar hypertrophy and obstruction at the level of the base of tongue were healthy, suggesting that this disorder is not necessarily limited to those with Down syndrome, other diseases with craniofacial manifestations, or neurologic disorders.
Lingual tonsillectomy for both adult and pediatric obstructive sleep apnea is historically well documented. A variety of techniques have been developed in the past to remove the lingual tonsils or to reduce the tongue base; recently the use of ultrasonic scalpel, microdebrider, coblation, and tongue suspension suture have been described. 10 - 13 Nevertheless, exposure of the lingual tonsils has been a universal limitation despite these innovative modalities. The use of endoscopes to assist in lingual tonsillectomy has been previously described 14 and has greatly improved access to this region and rendered the operation “routine.”
Our technique employs endoscopic visualization along with a number of other refinements, such as the Jennings mouth gag, retraction sutures, and a sweetheart retractor to elevate the tongue, all to improve oropharyngeal access. With the proper exposure, lingual tonsillectomy is no longer plagued by poor visibility and surgical uncertainty. The use of coblation as the technique of choice to remove the lingual tonsils has the advantages of low thermal energy (40 to 70 degrees Celsius) and ease of hemostasis. One potential disadvantage is the fact that coblation is an ablative technique; no specimen is delivered with coblation alone.
The results of this study suggest that children with persistent OSA despite prior T&A should be evaluated for other levels of obstruction, and when lingual tonsillar hypertrophy is the cause, it can be treated effectively by endoscopic-assisted coblation lingual tonsillectomy. While the average child undergoing lingual tonsillectomy is not necessarily “cured” of OSA, the severity as measured by PSG is significantly decreased (45.1%). In addition, there is a significant drop in the number of obstructive apneas, from over 18 events to approximately two events. Decreases in obstructive hypopneas as well as an increase in the minimum O2 saturation are suggested by the data, but with this limited cohort, these parameters are not yet significant. Of note, subgroup analysis between healthy patients (46%) and patients with comorbidities (54%) preliminarily shows no significant difference in outcomes, although there potentially may be a trend towards healthy patients having greater improvement. This is currently being investigated.
The procedure is surprisingly well tolerated by children; this may be largely due to the relatively low thermal energy delivered by the coblation wand. Patients subjectively complain of little pain and tolerate a regular diet soon after the effects of anesthesia dissipate postoperatively. While the patients in this study were kept overnight in a monitored floor bed for observation, no acute airway issues were encountered, and all children were able to be discharged the following morning. Two patients operated on early in this series were found to have adhesions between the epiglottis and tongue base on follow-up office flexible fiberoptic laryngoscopy; this was likely due to inadvertent injury to the mucosa on the lingual surface of the epiglottis during coblation. In spite of this, there appeared to be no consequential airway or feeding issues. Nevertheless, we have become more cautious with the ablation as we enter the vallecula.
It is conceptually easy to understand why lingual tonsillectomy was significantly effective for many of our patients. By removing excess lymphoid tissue from the tongue base, the airway aperture is enlarged. A more interesting conclusion is why the procedure is not more effective and why it fails outright in some. We have analyzed our patients and have found several reasons for failure. The most common is that while the lingual tonsils are present, the main cause of the OSA is tongue base prolapsed onto the posterior pharyngeal wall. This can be a consequence of a retruded mandible, but also can be due to muscle hypotonia. Anecdotally, we have found that a preoperative MRI can demonstrate the actual tissue thickness of the lingual tonsils, differentiating hypertrophy from normal lingual tonsils. Removing nonhypertrophied normal lingual tonsils, where there is prolapse of the muscular tongue base into the airway during sleep, does not yield consistently positive outcomes.
Another possible cause of failure is inflammation of the pharyngeal mucosa. Kheirandish-Gozal and Gozal have shown that mucosal inflammation plays an important role in pediatric OSA. 15 The same biologic process that results in pharyngeal lymphoid hyperplasia also involves the pharyngeal mucosa, contributing to the distortion. Clearly, lingual tonsillectomy does nothing to address this problem.
In conclusion, coblation-assisted lingual tonsillectomy with endoscopy is an effective and consistently reproducible procedure for treating OSA in children who have failed T&A and have demonstrated LTH. Adequate office fiberoptic laryngoscopy and operative endoscopic visualization of the dynamics of the tongue base (sleep endoscopy) is a critical component of establishing the diagnosis of LTH. A complete examination of the airway is also critical in establishing or ruling out synchronous lesions contributing to the OSA. Our failures and inability to cure OSA despite addressing the problem of LTH highlight the complex nature of this disease and the important work that remains to be done to improve our understanding of its multiple causes.
Author Contributions
Disclosures