
Abstract
Normal hearing requires the integrity of the outer, middle, and inner ear. The inner ear contains specialized sensory hair cells that function to transduce mechanical sound waves into neural signals. Because they are terminally differentiated and have lost the capacity to regenerate, loss of these sensory hair cells can lead to irreversible sensorineural hearing loss (SNHL). One common and preventable cause of hair cell loss is exposure to ototoxic medication, such as the aminoglycoside class of antibiotics. Despite their known side effects, 1 the aminoglycoside antibiotics are commonly administered because of their potent antibacterial activities.
Patients with cystic fibrosis (CF) most commonly suffer from infections involving their pulmonary and sinonasal systems. Virulent bacteria such as the gram-negative bacteria are commonly responsible for these infections, warranting treatment with the aminoglycoside antibiotics such as amikacin or tobramycin and less commonly, gentamicin. Because of their frequent exposure to aminoglycosides, these patients are at particularly high risk of developing SNHL. 2 - 4 A wide range of results exists on the prevalence of SNHL in patients with CF. Some authors have reported high prevalence in this population (28%), 2 , 5 whereas others have reported much lower percentages. 4 , 6 - 9 Some of these studies have focused on examining the adult but not the pediatric CF population, whose profiles are rather different from each other: 1) The pediatric patients are often less reliable in reporting their hearing deficits. 4 , 6 2) The aminoglycoside treatment regimen is often of shorter duration. 4 , 10
In addition, macrolides are being increasingly utilized in the management of CF patients because of their antibacterial and immunomodulating properties, as well as their inhibition of biofilm production. 11 However, macrolides have been, in a handful of case reports, associated with the development of hearing loss. 12 , 13
We designed this study to retrospectively examine the prevalence of SNHL in pediatric patients with cystic fibrosis and to identify potential risk factors for hearing loss in these patients.
Methods
Population
We reviewed the medical records of CF patients seen in the Department of Otolaryngology and Communication Enhancement at Children's Hospital Boston between March 1994 and December 2007. A total of 171 CF patients were identified; 51 of whom had received audiometric studies. Audiograms were not obtained in a systematic fashion; rather, the patients were referred at the discretion of the attending physician.
Audiometric Information
SNHL was diagnosed when pure tone air- and bone-conduction hearing thresholds were poorer than 15 dB HL at two or more adjacent frequencies between 250 and 8000 Hz. Hearing loss was thus defined because, compared with 25 dB HL in adults, a hearing threshold of 15 dB HL is considered a “low fence” for normal versus impaired hearing ability in pediatric patients. 14 One patient with a known SNHL and biallelic GJB2 mutations was excluded from our study. Demographic information for the remaining 50 patients was recorded and analyzed, including gender, age at audiogram(s); results of audiogram(s); tympanogram(s); history of inhaled, topical nasal, or systemic aminoglycoside treatment; history of systemic macrolide treatment; and CF genotype.
This study was approved by the institutional review board at Children's Hospital Boston.
Statistical Analysis
The objective of the analyses was to identify independent risk factors for SNHL. Logistic models were used for both univariate and multivariate models. Likelihood ratio tests and 95 percent likelihood–based confidence intervals were used in place of Wald-based methods owing to data sparseness (eg, no patients with five or fewer courses of nasal irrigation with aminoglycosides had SNHL). Logistic models were fit with the LOGISTIC procedure of SAS 9.1 (2002-2004; SAS Institute Inc, Cary, NC).
Results
Seven (14.0%) patients had SNHL, with the most common pattern being bilateral and high frequency. Uniformly, hearing loss was poorest at 8000 Hz, relative to lower frequencies (Fig 1). One (2.0%) patient had severe bilateral tinnitus without SNHL in the conventional audiometric frequencies. The average age of our patient cohort was 11.4 years old (n = 50). The average age was 15.0 years for the SNHL group and 10.9 years for the normal hearing group. Twenty-six patients were female and 24 were male; SNHL was identified in four (15%) females and three (13%) males (Table 1).
Cystic fibrosis patient data
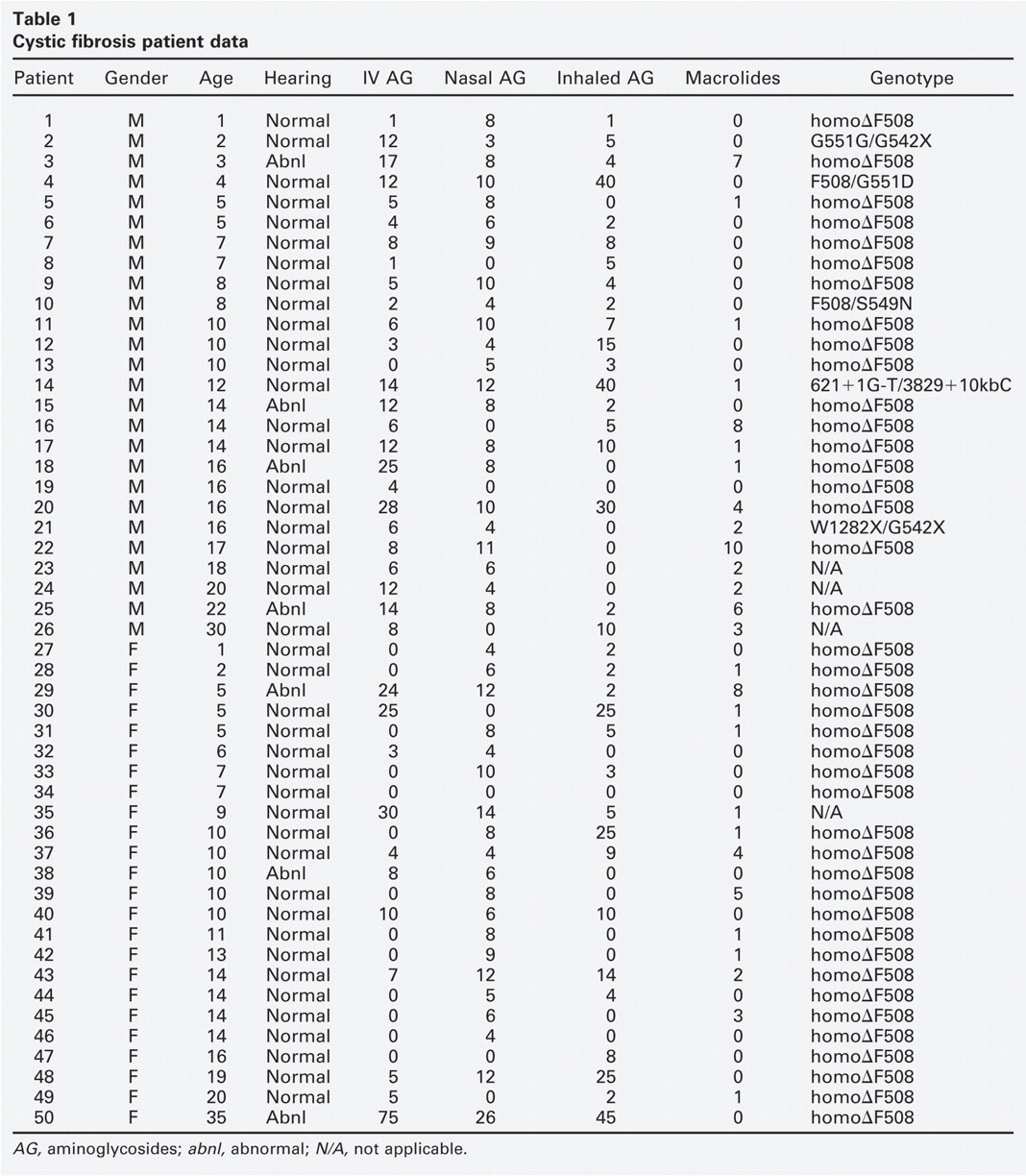
AG, aminoglycosides; abnl, abnormal; N/A, not applicable.
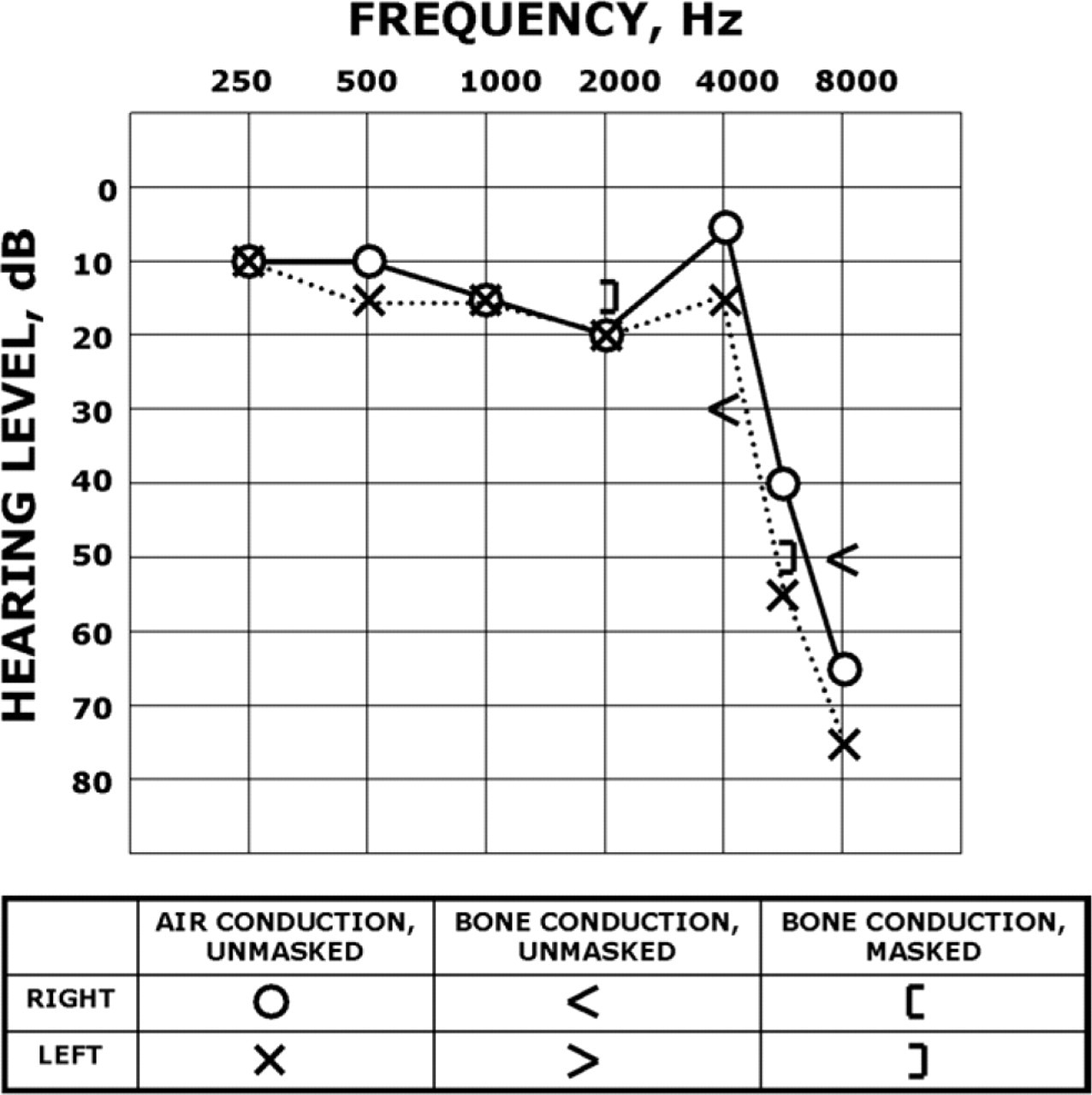
CF patient's abnormal audiogram depicting representative bilateral high-frequency SNHL.
To examine the effect of intravenous aminoglycoside treatment on the prevalence of SNHL, we separated our cohort into those who received 10 or fewer versus more than 10 courses of aminoglycoside antibiotics. SNHL was identified in only one patient in the former group (3%; n = 36) compared with six in the latter (43%; n = 14) (P < 0.001; odds ratio [OR] = 26.2; 95% CI, 3.8-533.7).
Patients who received topical nasal irrigation with aminoglycoside antibiotics were dichotomized into those who received five or fewer courses versus more than five courses of treatment. There were no patients with SNHL in the former group (0%; n = 19) compared with seven in the latter group (23%; n = 31). Although the maximum likelihood estimator of the OR was unbounded, the lower bound of the 95 percent confidence interval was 2.3, indicating that patients receiving nasal irrigation with aminoglycoside antibiotics are at higher risk of developing SNHL (P < 0.01).
There was no detectable effect of inhaled aminoglycoside treatment on SNHL. There were six patients with SNHL who had five or fewer courses of treatment (18%; n = 34) compared with one patient with SNHL among those who had more than five courses (6%; n = 16) (P = 0.249).
Four patients who received five or fewer courses of macrolide treatment had SNHL (9%, n = 45); whereas 3 patients who received more than five courses of treatment had SNHL (60%, n = 5) (P < 0.01; OR = 15.4; 95% CI, 2.0-148.7).
The genetic profile was known in 46 patients. Forty-one patients carried homozygous ▵F508 mutations in the CFTR gene, seven of whom had SNHL (17%, n = 41). Five patients carried biallelic CFTR mutations other than homozygous ▵F508, none of whom had SNHL (P = 0.185) (Table 1).
The univariate results suggest that intravenous aminoglycosides, topical nasal irrigation with aminoglycosides, and macrolide treatment are independent predictors for SNHL in CF patients. However, in a multivariate context, the effect of each risk factor is slightly diminished after accounting for the presence of the other two risk factors. This difference is due to the positive correlations between risk factors (eg, the correlation between macrolide and intravenous aminoglycoside treatments was 0.24). Therefore, in the multivariate analysis, for intravenous aminoglycosides, the OR was 18.8 (95% CI, 2.1-488.6; P < 0.01). For nasal irrigation with aminoglycosides, the odds ratio was unbounded, but the lower bound of the 95 percent CI was 1.1 (P < 0.05). For macrolide treatment, the odds ratio was 12.1 (95% CI, 0.7-525.2; P = 0.079).
Tympanograms were performed in 44 patients, of which nine (20%) were abnormal and showed evidence of middle ear effusion and/or eustachian tube dysfunction (types B and C). None of these patients with abnormal tympanograms had SNHL.
Discussion
SNHL is a well-recognized side effect of aminoglycoside treatment. Aminoglycosides are transported into both inner and outer cochlear hair cells, leading to generation of reactive oxygen species, activation of the cell death cascade, and eventually the demise of these hair cells. 15 Once uptake into the hair cells has occurred, the aminoglycoside antibiotics are poorly excreted and thus have a long half-life in the inner ear. For this reason, it has been observed that patients who have received multiple courses of aminoglycosides, especially within a short period of time, such as CF patients, are at particularly high risk for developing SNHL.
In our patient group, the overall rate of SNHL was 14 percent and was within the range reported in the literature. 2 , 4 - 9 Although the retrospective and “convenience sample” nature of our patient cohort does not allow a direct statistical correlation between the use of systemic or intranasal topical aminoglycosides or systemic macrolides and SNHL, we did identify several significant risk factors: more than 10 courses of intravenous aminoglycoside treatment and more than five courses of topical nasal irrigation with aminoglycosides. Although the cumulative effects of intravenous aminoglycoside treatment have been observed to lead to SNHL, 6 only one previous study has reported detectable levels of aminoglycosides in the bloodstream after nasal irrigation; in that study of 12 patients, the authors noted a unilateral threshold shift at 8000 Hz in one patient. 16 An additional study of tobramycin comments on the lack of hearing loss, but the presence of occasional tinnitus, in patients receiving tobramycin compared with placebo. 17 Finally, there is one case report of a CF patient with renal failure who developed profound SNHL following inhaled aminoglycoside treatment. 18 One possible explanation for the difference between these reports and the current study is that topical nasal irrigation results in higher systemic concentrations of aminoglycosides than with the inhaled application, and potentially reaches ototoxic levels when accumulated over repeated use.
In the univariate analysis we observed a higher incidence of SNHL in patients who received more than five courses of macrolides, such as azithromycin. In the multivariate analysis, however, the higher incidence did not quite reach significance. There have been several published case reports of SNHL associated with macrolide antibiotic treatments 12 , 13 in non-CF patients. Macrolides appear to confer, in addition to antibacterial properties against CF-related organisms other than Pseudomonas aeruginosa, antibiofilm activity, 11 and immunomodulating effects on pulmonary diseases with an inflammatory component, including CF; these drugs are therefore being increasingly used to manage these patients. 19 Further investigation with larger patient cohorts is needed to confirm the relationship between repeated macrolide use and SNHL.
The possibility exists that we have overestimated the prevalence of SNHL as a result of a selection bias at a tertiary referral center; this is intrinsic to a retrospective study. On the other hand, owing to our primary use of pure-tone thresholds from 250 Hz to 8000 Hz, we may have missed certain patients with subtle auditory deficits that would have been detected by high-frequency audiometry (above 8000 Hz) or otoacoustic emissions. For instance, the patient who had severe bilateral tinnitus without associated SNHL by conventional audiometry could have potentially benefited from these measures. High-frequency hearing and outer hair cells are typically first affected during aminoglycoside ototoxicity; therefore, methods using both high-frequency audiometry and otoacoustic emissions are potentially more sensitive in detecting early and mild auditory pathology and should be employed in future studies. 3 , 10 , 20
Conclusion
Pediatric patients with CF are at high risk for developing SNHL because of their frequent exposure to aminoglycosides. All CF patients should have routine and longitudinal audiometric evaluations as part of their overall management, especially after they start receiving systemic or intranasal aminoglycosides and possibly after starting macrolides. A larger, prospective study using conventional and high-frequency audiometry and otoacoustic emissions to screen SNHL in CF patients is warranted.
Author Contributions
Disclosures
Footnotes
Acknowledgements
James Daley, BS, and Sherri Horonjeff, PA: assistance with data collection; Jessica Guidi, BS: assistance with manuscript preparation.