
Abstract

Solitary fibrous tumor (SFT) is a relatively rare mesenchymal tumor that usually arises from the pleura. With respect to the head and neck regions, SFT in the larynx is extremely rare. To date, only seven patients with supraglottic laryngeal SFT have been described in the literature. However, no patient with laryngeal SFT present in the subglottic space has yet been described. We herein report the first case of laryngeal SFT localized in the subglottic space.
A 68-year-old man was referred with a six-month history of hoarseness and a one-month history of difficulty breathing. He had never smoked and was not on medication. Fiberoptic laryngoscopy revealed a smooth submucosal mass present in the subglottic cavity. The remainder of the larynx, including the vocal cords, appeared normal. The movement of the bilateral vocal cords was preserved well. The routine laboratory values were unremarkable. CT with contrast revealed a 2.5 × 4 cm well-defined mass with slight enhancement, which was located between the thyroid cartilage and the cricoid cartilage (Fig 1). Because his dyspnea was severe and it was speculated that it would become worse with surgical intervention, a tracheostomy was performed with the patient under local anesthesia, and a specimen was biopsied. The histologic features of the tumor were consistent with the diagnosis of a laryngeal SFT.1,2 In addition, the tumor had some atypical histologic features, such as hypercellularity, a high mitotic count, and a high Ki-67 labeling index, which indicated that the tumor had a malignant potential (Fig 2). The mitotic count was six per 10 high power fields. The patient's tracheostoma was maintained after the biopsy, and a curative resection was thereafter performed with the patient under general anesthesia. The tumor and a small portion of skin adherent to the tumor were separated from the surrounding normal tissue by electrode knife and excised by a transcervical approach without a laryngectomy. It lay at the center of the ligament cricothyroideum. Laryngeal mucosa, bilateral cricothyroid joints, and the recurrent laryngeal nerves were preserved. The postoperative course was without complications, and the patient was decannulated in nine days. Pathologically, the surgical margin was negative. The histologic results were the same as the preoperative biopsy. After 23 months follow-up, the patient has remained tumor free. We currently follow-up on the patient once every three months and consider a permanent follow-up necessary. We received Nagasaki Medical Center Institutional Review Board approval for this study.

Contrast-enhanced sagittal CT image of a mass located in the subglottic laryngotracheal transition region (asterisk).
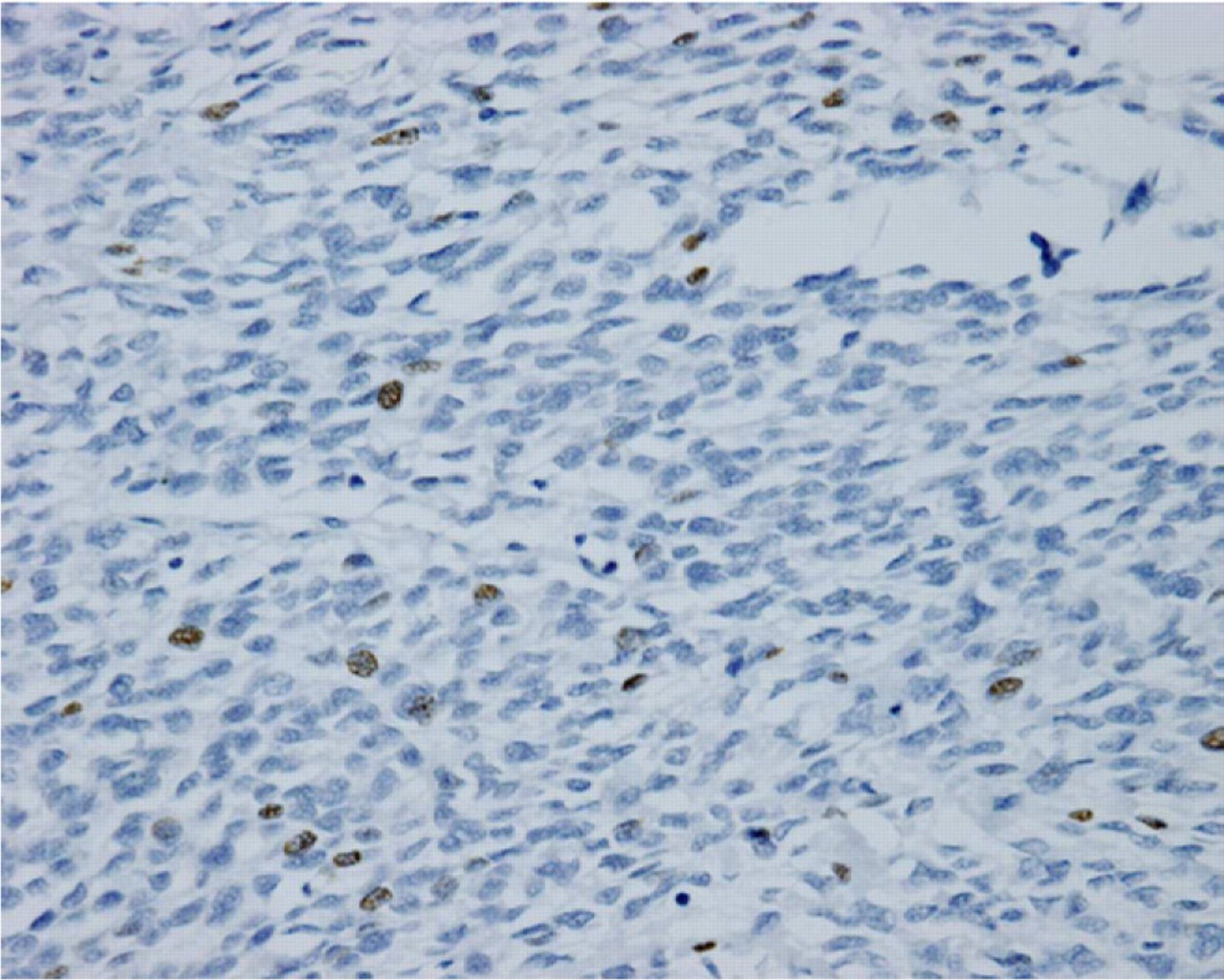
The findings of Ki-67 staining for the tumor. The dark brown stained nuclei were considered as immunopositive. The Ki-67 labeling index was seven percent.
Discussion
Preoperative diagnosis of a laryngeal SFT is difficult because the clinical symptoms, physical examination, and the imaging findings of ultrasound, CT, and MRI are not definitive. In general, a correct final diagnosis of SFT requires pathologic and immunohistochemical examination of the resected surgical specimens from the tumor preoperatively.1,3 With respect to the surgical resection, an important point of discussion is the malignant potential of SFT. It is known that an SFT recurs locally and even metastasizes to distant sites. The suggested pathologic criteria for the characterization of malignancy include high cellularity, more than four mitoses per 10 high power fields, nuclear pleomorphism, and necrosis. A positive surgical margin was associated with a statistically worse outcome in terms of local recurrence and metastasis.4 Ki-67 also is thought to be a useful prognostic indicator for SFT. Sun et al5 reported a higher Ki-67 labeling index (6.11 ± 1.05%) in malignant SFTs than in benign SFTs (1.9 ± 0.43%; P < 0.05).5 In the current case, biopsy revealed that the tumor had a malignant component. In the current case, the question arose regarding whether a total laryngectomy or a partial removal with preservation of the larynx should be performed. In supraglottic SFTs, an endoscopic resection by means of a CO2 laser or a partial laryngectomy is normally performed. However, in the current case, because the mobility of the vocal cord was good, the tumor was mainly present in the subcutaneous to the submucosal region of the larynx, the surface of the tumor was well-defined on CT, and the distance to the vocal cord was greater than 10 mm, we thought that the tumor could be completely removed by a transcervical approach without performing a total laryngectomy. Unless the surgical margin was negative, we had planned to perform a total laryngectomy because of the malignant potential of the tumor. With respect to the subglottic SFTs, although the resection area should depend on the extension of the tumor, a transcervical approach with the preservation of the larynx is considered to be one of the effective choices for surgical treatment.