
Abstract
Tonsillectomy, with or without adenoidectomy, is one of the most common surgical procedures in pediatric otolaryngology. 1 Pain is the main cause of morbidity in the postoperative period (PO) of tonsillectomy, and its management, be it in a hospital setting or at home, is longer than ideal. Among children who undergo tonsillectomy who receive analgesia at home with paracetamol, 90 percent have pain in the first 24 hours after surgery. 2 In the first three days, 60 to 70 percent of children have pain equal to or greater than 3 on the visual analog scale of 0 to 10, and pain can last longer than one week. 3
There has been growing concern about the quality of life of patients who undergo tonsillectomy, reflected by the publication in recent years of comparisons of several types of treatments for analgesia. Despite all of the investigations, it is necessary to utilize more than one analgesic medication in the PO, and it appears that it will be a long time before the development of a single treatment for postoperative analgesia. 4
Sucralfate is a disaccharide utilized in peptic ulcer. It binds to the protein matrix of the ulcer, forming a protective barrier, impeding aggression by gastric acidity, pepsin, and bile salts. It is believed to have a cytoprotective effect and to accelerate recuperation of mucosa. 5 In adults, two clinical trials have determined the effect of sucralfate in PO of tonsillectomy, showing reduction in pain in the first three days. 6 , 7 In children, one clinical trial showed reduction in pain with use of sucralfate. However, it was not placebo-controlled and did not measure pain with a validated method. 8 Another clinical trial evaluated the effect of sucralfate on oropharyngeal pain in children at six hours, 24 hours, and seven days after adenotonsillectomy, showing reduction in pain only at six hours. In spite of the use of sucralfate up to the end of follow-up, there were no measurements of pain between days one and seven. 9
Care must be taken in the evaluation of pain. Self-reporting using a visual analog scale (VAS) is considered the better method, but should be adapted to specific age groups. 10 It is known that linear VAS utilized in adults is not suitable for children. 11 Pain should be determined by using a faces pain scale well understood by children. 12
Due to the limitations of these studies, we evaluated the effect of topical sucralfate compared to placebo in reduction of pain in children submitted to adenotonsillectomy during the first five postoperative days.
Methods
Study Design
We conducted a randomized, double-blind clinical trial to determine the effect of topical sucralfate in comparison to placebo on reduction of postoperative pain in children submitted to adenotonsillectomy for five days after surgery.
Patients of both sexes who were four to 12 years old with an indication for adenotonsillectomy due to adenotonsillar hyperplasia with obstructive symptoms of superior airways were selected at the pediatric otolaryngology ward of Hospital da Criança Santo Antonio. Patients were excluded if there was evidence of clinically significant disease that contraindicated their participation in the study. The sample was selected in a consecutive manner, enrolling children who met criteria for inclusion and whose parent/guardian agreed to participation in the study.
This study was derived from a major protocol of analgesia with topical medications and also included an arm with use of topical clindamycin. In order to keep a balanced number of patients in each group, we elected to use randomized blocks. Prior to the beginning of the study, an independent investigator established randomized blocks with six patients: two in the sucralfate group, two in the clindamycin group, and two in the placebo group. These were distributed randomly within the block. Positions within the blocks were given increasing numbers, and this number identified a sealed opaque envelope containing treatment group. Each surgeon received his or her randomized blocks. The six patients of the same block were operated on by the same surgeon. At the time of surgery, the team contacted the hospital pharmacy and provided the patient's data and surgeon's name. The pharmacist in charge opened the corresponding envelope, which contained the type of treatment, and sent the medication for the study. Treatment was kept secret, revealed only after conclusion of the study.
Blinding was maintained in a manner in which the surgeon, main investigator, and patient/family had no knowledge of who was receiving intervention or placebo. Placebo was a lactose solution that was meant to have the same density, coloration, texture, taste, and bottle as sucralfate and was prepared in the hospital pharmacy.
Outcomes
The main outcome was the level of oropharyngeal pain during the first five postoperative days. Secondary outcomes were otalgia, frequency of paracetamol use, days of paracetamol use, type of diet, secondary bleeding, vomiting, and change in weight.
Procedures
In the anesthetic induction room, the child received midazolam 0.5 mg/kg orally. The patient remained in the company of one parent/guardian until inhalation induction was performed. In the recovery room, the child remained in the company of one parent/guardian.
Adenotonsillectomy was performed by five otolaryngologists who used the cold dissection technique, without utilization of electrocauterization, and hemostasis was achieved by compression with moist gauze and/or suture.
A solution of sucralfate was prepared at a concentration of 1 g in 60 mL of water. Placebo was 1 g of lactose diluted in 60 mL of water. Patients were randomized and received sucralfate or placebo solution intraoperatively and postoperatively.
At the end of surgery, while the patient was still anesthetized, the oropharynx was irrigated with sucralfate or placebo solution, which was left in place for one minute and then aspirated. On the morning after the procedure, the patient initiated use of sucralfate or placebo, rinsing his or her mouth with 10 mL of solution and then swallowing four times a day for a period of five days.
Study Protocol
Parents/guardians of children who met criteria of eligibility were informed about the study and signed a consent form. A diary was provided that was to be filled out every morning with regard to the variables of the study.
Pain was evaluated by using the Revised Faces Pain Scale. 11 The child had contact with the scale before the surgical procedure, for the purpose of becoming familiar with the method of evaluation. It was utilized for measuring intensity of oropharyngeal pain and otalgia. It was performed, always by the same investigator, on the first, third, and fifth postoperative day during an office visit. On the second and fourth day, it was measured by the parent/guardian.
For analgesia, 200 mg/mL paracetamol drops were prescribed, every six hours, when necessary. Paracetamol use was to be recorded in the diary, varying from zero times up to four times a day. It was recommended that initially the diet be liquid and soft, making it optional in subsequent days. Type of foods eaten (liquid/soft or solid) was recorded in the diary. Secondary bleeding was evaluated by absence of bleeding, presence of streaks of blood in saliva, or presence of flowing blood, and recorded in the diary, as was the occurrence of vomiting.
The main investigator examined patients on the first, third, and fifth postoperative day to verify adherence to treatment, correct use of medication, and adequate filling out of the diary. Weight and temperature of the child were determined. In case of high fever (above 38.5°C) or any effect that could be attributed to medication, patients were advised to contact the investigator for evaluation and possible removal from the study.
Statistical Analysis
For calculation of sample size, we accepted a type I error of five percent (alpha = 0.05) and a type II error of 20 percent (beta = 0.20), such that the power of the study would be 80 percent. Previous studies utilizing sucralfate showed a difference in proportions of pain between the sucralfate-treated group and placebo, diminishing in the subsequent days, where there was a statistically significant difference up to the third day. 6 , 7 Based on these data for calculation, we determined that we needed to enroll 35 patients for each group. Considering a loss of 15 percent, the number of patients necessary for each group was 41, totaling 82 patients.
Data with regard to oropharyngeal pain, otalgia, analgesic use, and alteration in weight were described as means and standard deviation (SD). As multiple measurements were taken of the same patient at different times, data were evaluated by repeated-measures ANOVA. Mean number of days of paracetamol use was calculated using the t test. Other data were categorized and analyzed as qualitative variables, utilizing the χ2 test or Fisher exact test.
Ethical Aspects
This study was submitted to and approved by the Committee of Ethics in Research of Complexo Hospitalar Santa Casa, under number 1119/05, with respect to the ethical and scientific aspects, as recommended by the Brazilian National Health Council.
Results
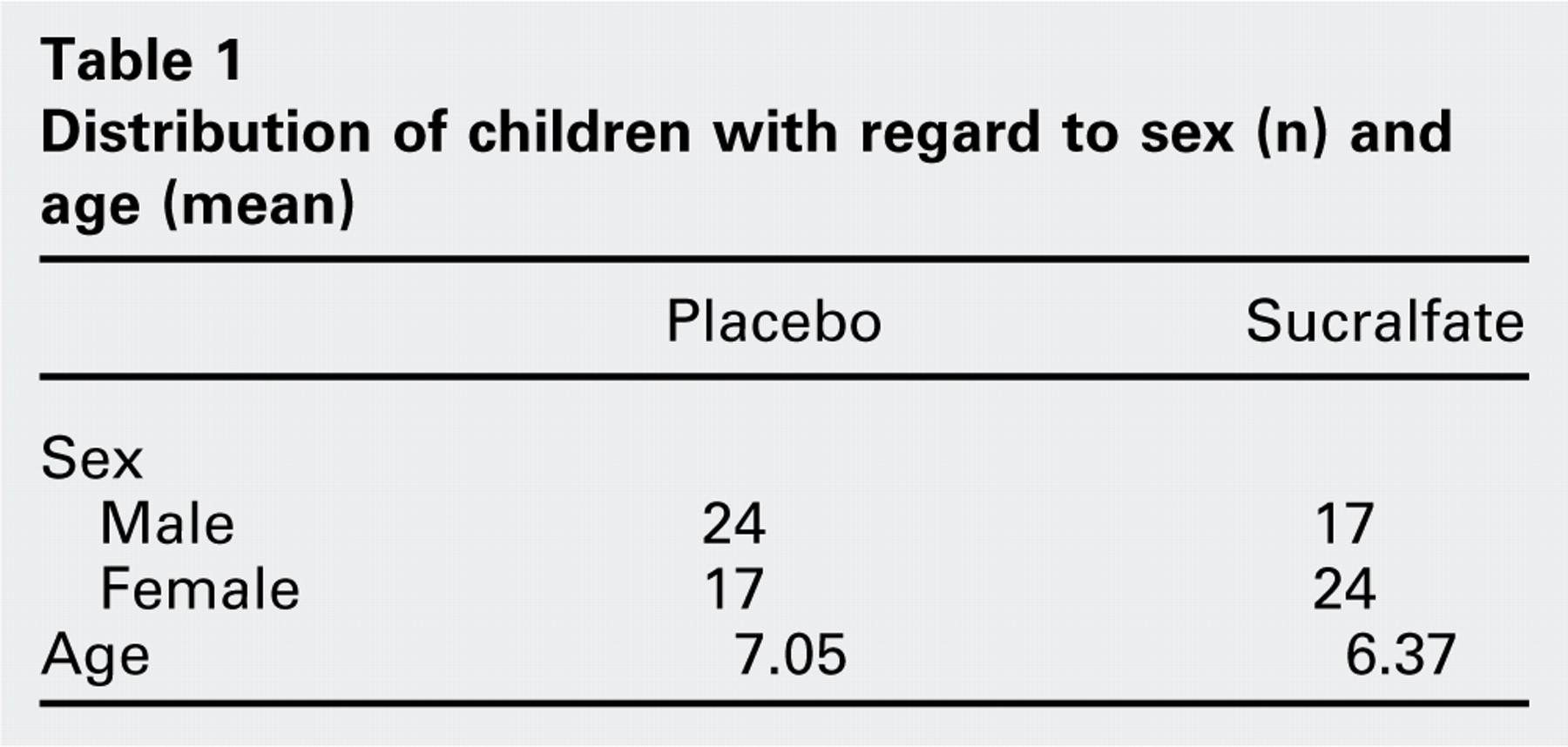
A total of 82 patients were randomized for the study. Because we chose to use randomized blocks, distribution was balanced with 41 patients in the sucralfate group and 41 patients in the placebo group. In the sucralfate group, one patient was excluded due to high fever, and one patient was excluded because of loss to follow-up (Fig 1). No patient was excluded because of intolerance or adverse effects to medication. No adverse effects were encountered. General characteristics of the patients are presented in Table 1.
Main Outcome
Oropharyngeal pain was evaluated during five days post-adenotonsillectomy, observing a significant effect in interaction between use of sucralfate and reduction of pain during the follow-up period (P = 0.006). Reduction of pain effect was significant during five days of treatment when compared to the placebo group (Table 2). Interaction between surgeon and pain was not significant (P = 0.68), demonstrating that development of pain was not influenced by the different surgeons.
Secondary Outcomes
With respect to otalgia, no significant difference was observed between use of sucralfate and reduction of pain in the follow-up period when compared to the placebo group (P = 0.216). In relation to frequency of analgesic use, there was no significant reduction in paracetamol use in the group of patients who received sucralfate (P = 0.368). The average number of days of paracetamol use was 2.61 days (SD = 1.69) in the sucralfate group and 3.14 days (SD = 1.58) in the placebo group, with a difference of 0.53 day (P = 0.15). Similarly, there was no demonstration of a significant reduction in weight in patients in the placebo group compared to the sucralfate group (P = 0.199) (Table 3). Return to solid food was gradual in the two groups, and there was no significant difference between them (P > 0.05). The level of secondary bleeding was low, with reference only to streaks of blood in the saliva, which showed gradual reduction, and no significant difference was seen between the two groups (P > 0.05). Occurrence of vomiting was low and without a significant difference between the placebo group and the sucralfate group (P > 0.05), and a total absence of vomiting by the fourth day of follow-up was observed (Table 4). Fever was a rare event and there was no significant difference between the groups (P > 0.05).
Discussion
In the methodological planning of our study, we took care to control factors with the potential to cause interference in perception of pain. With respect to use of premedication, all children received midazolam before surgery. Anesthetic procedure was also standardized. The child remained accompanied by a family member/guardian until anesthetic induction as well as later after awakening in the recovery room.
Despite a continuous search for alternatives in analgesia after adenotonsillectomy in children, the majority of studies neglect a very important factor, namely the method of measuring pain. Many authors utilize the VAS measured in millimeters. However, it is known that this method, which is often applied in adults, loses its reliability in children less than seven years of age. Therefore, results of various studies are impaired by this bias in measurement. In children under three years, the method utilized for evaluation of pain is based on observation of physiological, motor, and behavioral responses. For children between three and seven years of age, a better method for measuring pain is using faces pain scales. We chose a faces pain scale that has been validated and is easy to apply and understand. Although the scale can be utilized in children as young as three years of age, its interpretation depends on the cognitive development of the patient, which for this function is more consolidated after age four. 12 Therefore, we decided not to include patients under four years of age.
Freeman and Markwell 6 published, in 1992, a randomized, double-blind, placebo-controlled clinical trial in which 34 adults (16 in the sucralfate group) underwent tonsillectomy (cold dissection and snare; hemostasis with electrocautery) and received for 10 days a solution containing sucralfate or placebo (lactose). They found a reduction of oropharyngeal pain in the first three days, protection against otalgia starting at five days, and reduction in analgesia in the group that received sucralfate. 6
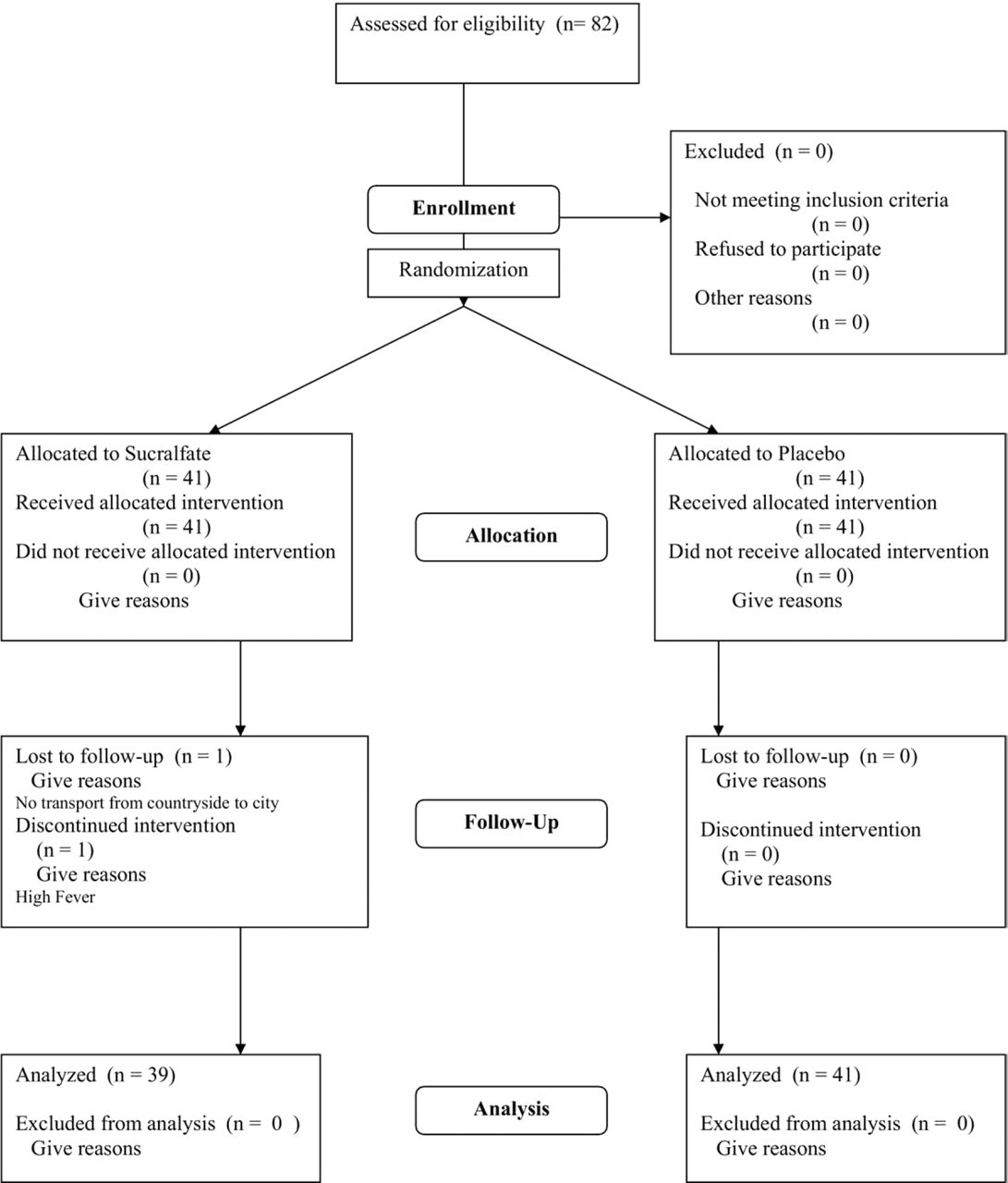
Patient flow diagram.
Özcan et al 7 published a randomized, double-blind, placebo-controlled clinical trial with methodology similar to the previous study. Tonsillectomy technique was cold dissection and snare, and hemostasis was with suture ligation. A total of 80 adults (50 in the sucralfate group) were evaluated for six days. A reduction of oropharyngeal pain was observed up to the third day and there was less necessity for paracetamol use up to the fourth day in patients who received sucralfate. 7
Esteban et al 8 conducted the first study of sucralfate in PO of tonsillectomy in pediatric patients. A total of 205 children were examined for five days. They found an association between use of sucralfate and reduction in oropharyngeal pain, as well as less need for analgesic use in PO. 8 Although the study was randomized, it was not placebo controlled. Besides, measurement of pain was subjective, determined either by the child or by a family member/guardian; a known and validated method was not used.
The most recent clinical trial of sucralfate was carried out in 69 children between 3 and 12 years old. Surgery was performed with cold dissection and hemostasis with suture ligation. Patients were evaluated at six hours, 24 hours, and seven days. A significant benefit (P < 0.05) was found in use of sucralfate for reduction of pain only at six hours postoperatively. Of all the previous studies on sucralfate, it is the one that showed the best methodology, with standardization of anesthetic procedure, avoidance of premedication, and utilization of a pain scale validated for children (Oucher). 9 It is not clear why the authors did not evaluate patients between the first and seventh day considering that prior studies in adults demonstrated benefit of sucralfate up to the third postoperative day.
Distribution of children with regard to sex (n) and age (mean)
Our study shows lower mean levels of pain in the group that received sucralfate during follow-up, and this effect was significant during five days of evaluation when compared to placebo. In relation to earlier studies, this effect is similar to that described by Esteban et al, despite methodological limitations of this author. 8 With respect to studies in adults, a benefit was also observed that was significant up to the third day after surgery. As the number of patients in these studies was smaller, it is possible that there was insufficient statistical power to demonstrate an effect on the fourth day of evaluation. The study of Sampaio et al did not measure pain between days two and six, and therefore it did not show the potential effect of sucralfate in this period. 9
Our results did not show a reduction in otalgia with the use of sucralfate, and although the study by Freeman and Markwell observed protection against otalgia starting on day five, other studies also found no benefit. 6 Otalgia is an indirect measure in assessing postoperative pain. Clinical epidemiology recommends care in highlighting results of secondary outcomes because the sample of patients is calculated to determine the main outcome. Unlike oropharyngeal pain, which is inherent to the procedure of adenotonsillectomy, otalgia is a symptom that is not present in all children. As a less common event, we would need more patients in both groups for the randomization to generate a balanced division. Otherwise, there is no way to predict who will feel this discomfort and thus balance the number of patients with otalgia in the sucralfate and placebo groups.
Evolution of oropharyngeal pain through five days: mean (SD; 95% CI)
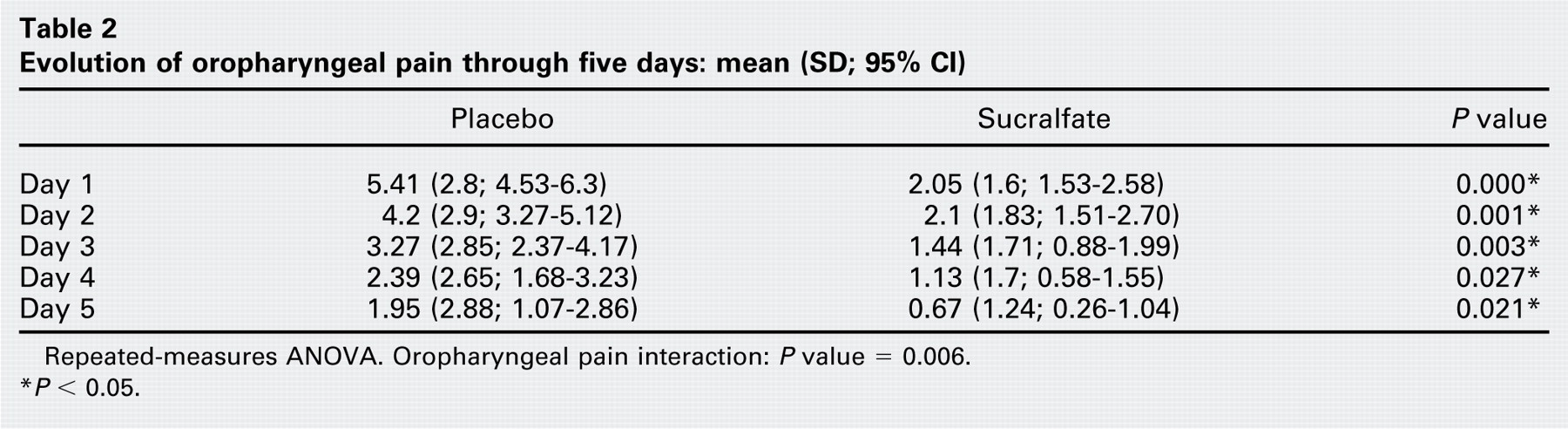
Repeated-measures ANOVA. Oropharyngeal pain interaction: P value = 0.006.
P < 0.05.
Evolution of otalgia, paracetamol use, and weight loss through five days: mean (SD)
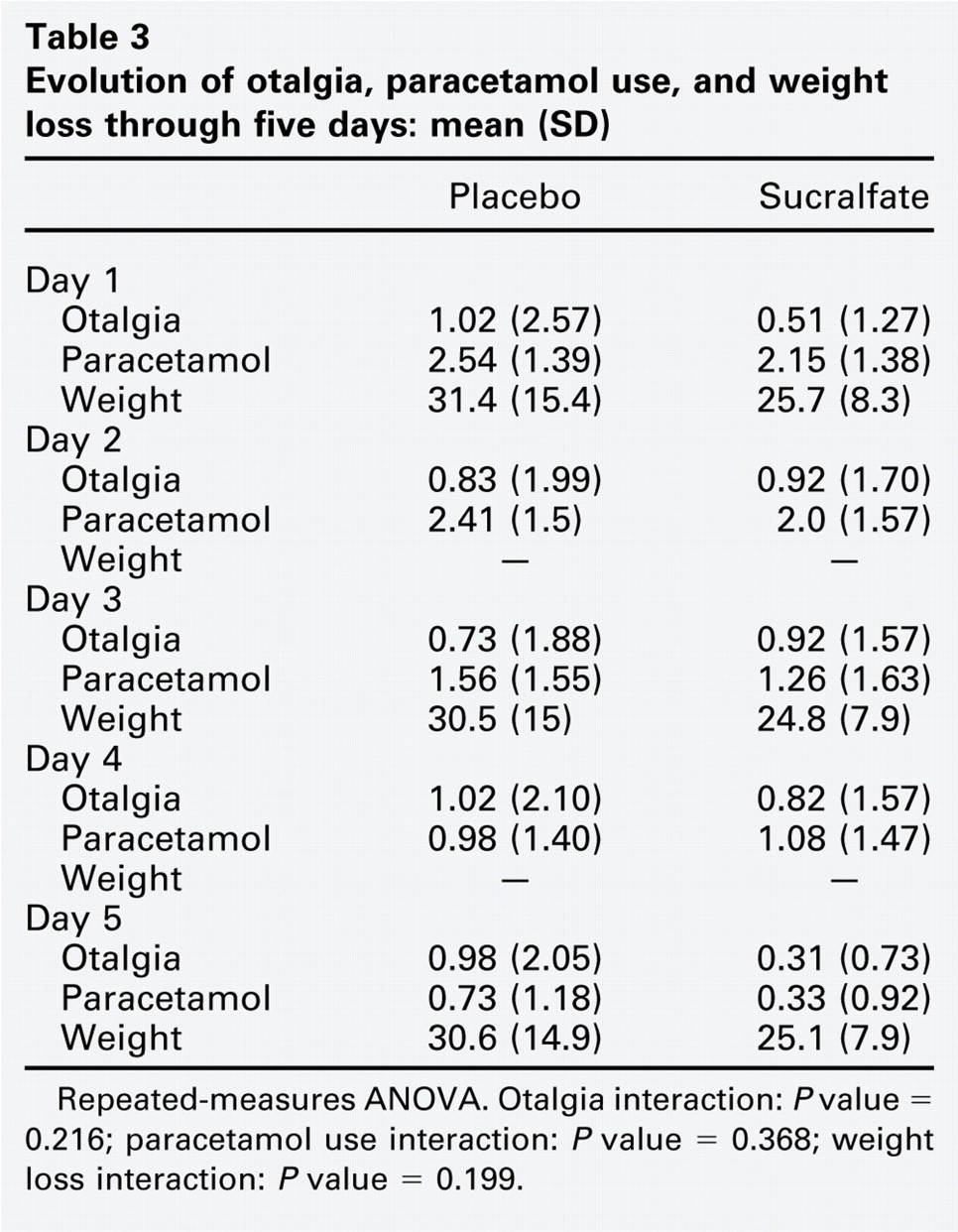
Repeated-measures ANOVA. Otalgia interaction: P value = 0.216; paracetamol use interaction: P value = 0.368; weight loss interaction: P value = 0.199.
There was no significant difference in frequency of paracetamol and days of analgesic use between the two groups. A trend toward lower frequency and fewer days of paracetamol use in the sucralfate group was observed (0.53 day). Freeman and Markwell evaluated use of paracetamol with codeine and observed lower consumption in the sucralfate group for a day and a half after surgery. 6 Özcan et al used paracetamol and observed lower consumption in the sucralfate group throughout follow-up. 7 Esteban et al evaluated analgesia by number of doses of paracetamol and by days of analgesic use. They found no significant difference in the number of doses of paracetamol in children who received sucralfate, but a trend to a lower rate. They noted reduction in paracetamol use in half a day in children who received sucralfate (P = 0.01). 8 Sampaio et al observed no difference in analgesic consumption. 9 Freeman and Markwell did not consider use of analgesics a good endpoint to assess the effect of sucralfate on pain in adults because they found that this was influenced by the pain tolerance of each patient and side effects of pain medication. 6 Studies in pediatric patients found no significant difference in frequency of paracetamol use. 8 , 9 As Freeman and Markwell pointed out, the patient may feel pain and have no need to use analgesics. 6 In children, besides tolerance to pain, we should consider that the analgesic will be administered by parents. The child may feel pain and not request the medication; parents may not realize that the child is in pain; or parents can have their own criteria for using analgesics. Based on these factors, frequency of paracetamol use may not be a strong outcome to assess pain, unlike the self-report of oropharyngeal pain. Since the sample is calculated for oropharyngeal pain, a greater number of patients would be necessary to detect a difference in this outcome. It is possible that a systematic review could clarify this topic and demonstrate that use of sucralfate in fact would reduce use of analgesics.
Type of diet, secondary bleeding, and vomiting through five days follow-up: % (n)
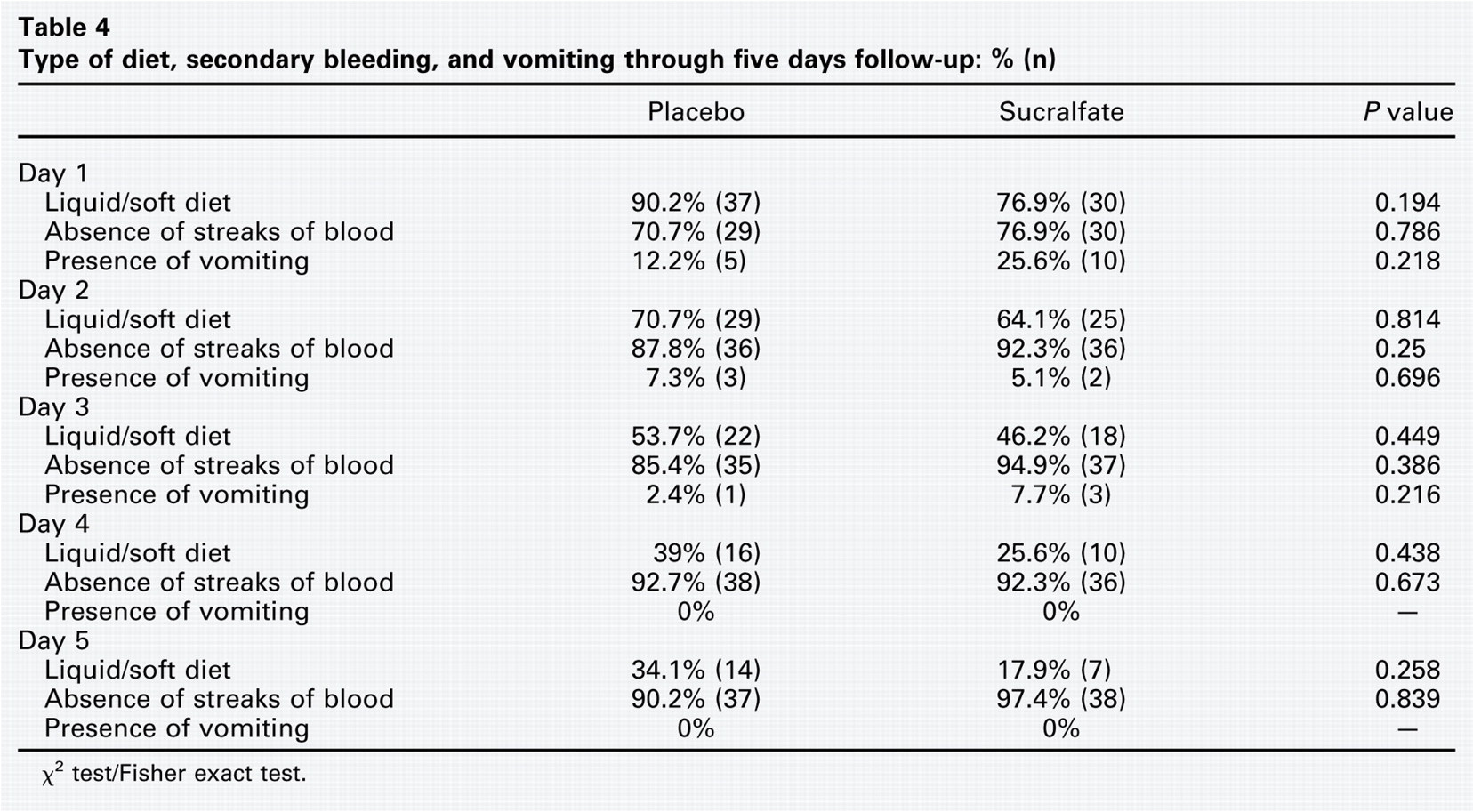
χ2 test/Fisher exact test.
As reported by other authors, we did not observe a more rapid return to a normal diet or change in weight. Fever, secondary hemorrhage, and vomiting were uncommon events, and there was no significant difference between groups.
Conclusion
To date, it is clear that use of sucralfate has a beneficial effect in reduction of oropharyngeal pain in PO of tonsillectomy. As studies have demonstrated by frequency of analgesic use, topical sucralfate does not have a potent effect to the point that it can be used as the only analgesic treatment. Because it is simple, safe, tolerated, and of low cost, it is our opinion that topical sucralfate is an important tool in adjuvant treatment of post-tonsillectomy pain.