
Abstract
Endoscopic sinus surgery (ESS) is widely accepted as the intervention of choice for chronic rhinosinusitis (CRS) refractory to medical therapy. 1 , 2 In fact, a growing body of evidence demonstrates that for recalcitrant disease in the general population, ESS is associated with improvement in disease symptoms, patient quality of life, and intranasal examination scores. 3 , 4 However, the effectiveness of ESS in adult CRS patients with concomitant severe systemic disease is largely undetermined. While it is certainly likely that such associated diseases may predispose individuals to develop CRS, it remains unclear whether it alters prognosis, leads to more severe disease, or requires alternative treatment paradigms when compared to the general adult population.
Cystic fibrosis (CF) is an autosomal recessive disease, characterized by aberrant pulmonary, sinonasal, and gastrointestinal tract mucociliary clearance, which leads to increased mucosal viscosity. Mechanistically, defective chloride channels lead to blockage of secretions with secondary infections, sinonasal polyposis, and marked inflammation. 5 , 6 Sinus CT imaging in CF patients often displays attachment of a demineralized or polypoid uncinate process to a medially displaced lateral nasal wall, typically sphenoid and frontal hypoplasia, and a predisposition toward mucocele formation. 7 Sinonasal polyps have a propensity for recurrence and mucosa generally fails to normalize following relief of obstruction in the CF population. 7
Surgical intervention is often sought to aid in initiating drainage of the paranasal sinuses and therefore attenuate the inflammatory cascade in patients with cystic fibrosis. 8 – 10 As the mean survival has improved over the last 30 years, CF patients increasingly present with CRS, refractive to conventional medical therapy, well into adulthood. 7 , 11 Little is known, however, about the effectiveness of surgical therapy in adult CF patients with recrudescent sinus disease. The purpose of our study was to evaluate the effectiveness of ESS on objective and disease-specific quality-of-life (QoL) outcomes in adult CF patients with CRS.
Methods
Patients were enrolled prospectively and followed at a tertiary care center. Approval from the Institutional Review Board (IRB) at the Oregon Health and Science University (OHSU) was obtained for consent and study protocols. All subjects were assured participation was voluntary. Informed consent was obtained for all participants meeting inclusion criteria.
Study Population and Inclusion Criteria
Adult subjects (≥18 years) presenting with diagnostic criteria for CRS, as outlined in the Rhinosinusitis Task Force (2003) and approved by the American Academy of Otolaryngology—Head and Neck Surgery, 12 were invited to participate after failing medical management and electing surgical management as the next treatment alternative. For CF cases, this treatment decision was made in consultation with the patient's pulmonologist in instances when both sinus symptomatology and pulmonary disease were considerations; however, sinus symptomatology was the primary factor in determining patient selection for ESS.
Demographic and Objective Measures
Demographic data and a detailed medical history were collected preoperatively and recorded on standardized forms. Factors and comorbidities of interest included age, gender, race/ethnicity, asthma, aspirin triad, nasal polyposis, tobacco use, history of depression, prior sinus surgery, allergies, and cystic fibrosis. Patients were defined as having cystic fibrosis after a positive sweat chloride test and meeting clinical criteria for this diagnosis following an evaluation by a pulmonologist or an internist. Baseline examinations of all subjects included standard bilateral nasal endoscopy and assessment of current CT imaging by the principal investigator (PI). Endoscopic examinations were quantified using the Lund-Kennedy (score range: 0–20) scoring system while CT scans were assessed utilizing the Lund-Mackay (score range: 0–24) scoring system. 13 In order to provide an objective measure of patient improvement, endoscopic examinations were performed again during postoperative follow-up evaluations by the PI. The PI was blinded to all QoL responses throughout the study duration.
Quality-of-Life Indicators
Subjects completed two validated disease-specific QoL instruments, the Rhinosinusitis Disability Index (RSDI) and the Chronic Sinusitis Survey (CSS). The RSDI is a disease-specific tool that evaluates self-perceived impact of CRS in a first-person descriptive format. It is a 30-item survey consisting of three separate subscales sensitive to predicting sinusitis-specific health outcomes in the physical, functional, and emotional domains. 14 The RSDI physical sub-scale consists of 11 items (score range: 0–44), the functional subscale consists of nine items (score range: 0–36), and the emotional subscale consists of 10 items (score range: 0–40). Total scores range from 0 to 120, with lower scores representing a lower impact of disease. In addition, the CSS was used as a disease-specific, complementary measure of duration-based (eight-week) symptoms and medical therapy. The CSS is a six-item questionnaire with total and subscale score ranging from 0 to 100, with higher scores representing a lower impact of disease. 15 In order to measure improvement in QoL status, subjects completed each survey both preoperatively and postoperatively.
Nested Case Control Design
Case subjects with comorbid CF and CRS were matched 1:1 on potential confounding variables (gender, race, and age) to control subjects without comorbid CF from the remaining cohort. For both subgroups, patients with at least six months of follow-up were selected, and the latest postoperative data were utilized for analysis.
Statistical Analysis
All data were recorded on standardized clinical research forms, transcribed, scored, and entered into a secure MS FoxPro (Microsoft Corp, Redmond, WA) database. All analyses were conducted utilizing SPSS v.16.0 statistical software (SPSS, Inc, Chicago, IL). Descriptive analyses of continuous variables were accomplished utilizing the Mann-Whitney U test for nonparametric distributions. χ2 testing was used for all frequency counts with Fisher exact test for small cell sizes and continuity corrections for all zero cell values. The magnitude of mean improvement in endoscopy exam and disease-specific QoL responses between preoperative and postoperative time points was assessed utilizing the Wilcoxon signed-rank test. Mann-Whitney U tests were utilized to rank differences between cases and controls for both mean preoperative and postoperative disease-specific QoL scores, as well as differences in absolute improvement between cases and control subjects. Means and standard deviations (± SD) were reported. An alpha level of 0.05 was considered statistically significant for all bivariate analyses.
Results
Subject Presentation
Twenty subjects with CRS and comorbid CF met inclusion criteria for the case group and were matched 1:1 with control subjects. As demonstrated in Table 1, there was no significant difference between groups in terms of demographics, including mean age and follow-up period. Furthermore, there were no appreciable differences in disease severity with respect to patients undergoing revision surgery. Subjects with CF did demonstrate a higher prevalence of nasal polyposis compared to control subjects, approaching statistical significance (P = 0.057). The prevalence of comorbid conditions was similar, except for a significantly higher proportion of allergic rhinitis in the control group (P = 0.008; Table 1).
Objective Measures
Baseline preoperative Lund-Mackay CT scores were significantly worse in the CF group as compared with controls (P = 0.001; Table 2). Preoperative mean endoscopy scores were significantly worse for CF cases than controls (9.3 ± 5.8 vs 5.7 ± 4.6; P = 0.049). Postoperative mean endoscopy scores were also significantly worse in CF cases compared to controls (7.9 ± 3.7 vs 3.9 ± 3.5; P = 0.001; Table 2). In comparing mean changes between preoperative and postoperative endoscopy scores (Table 3), neither cases nor controls showed a statistically significant improvement in endoscopy exam (–1.4 ± 4.3 vs −1.8 ± 4.2; P = 0.145 and P = 0.071, respectively).
Preoperative patient demographics, disease severity, and comorbidity prevalence for cases and controls∗
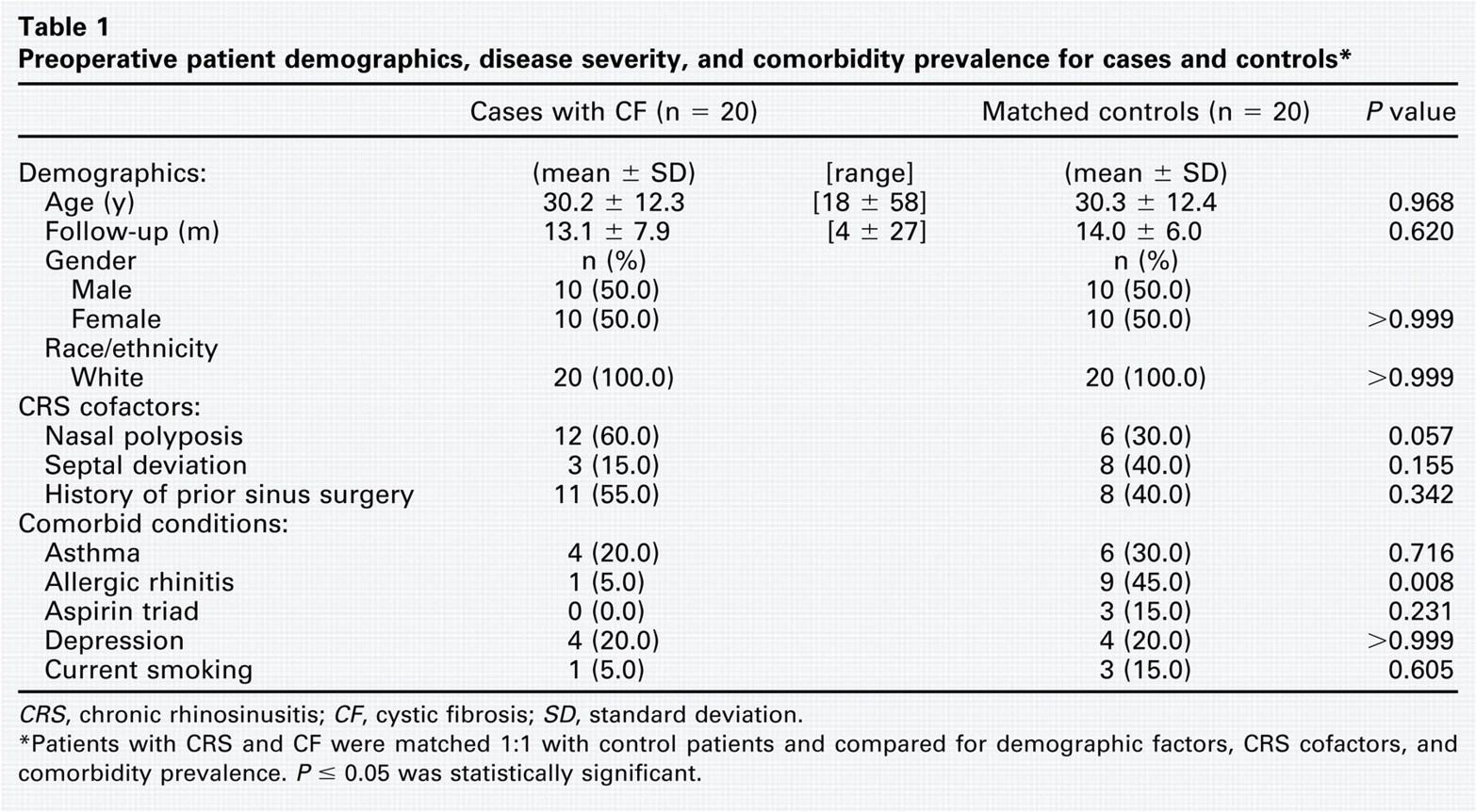
CRS, chronic rhinosinusitis; CF, cystic fibrosis; SD, standard deviation.
Patients with CRS and CF were matched 1:1 with control patients and compared for demographic factors, CRS cofactors, and comorbidity prevalence. P ≤ 0.05 was statistically significant.
Mean preoperative and postoperative differences in endoscopy and disease-specific quality-of-life measures for cases and controls∗
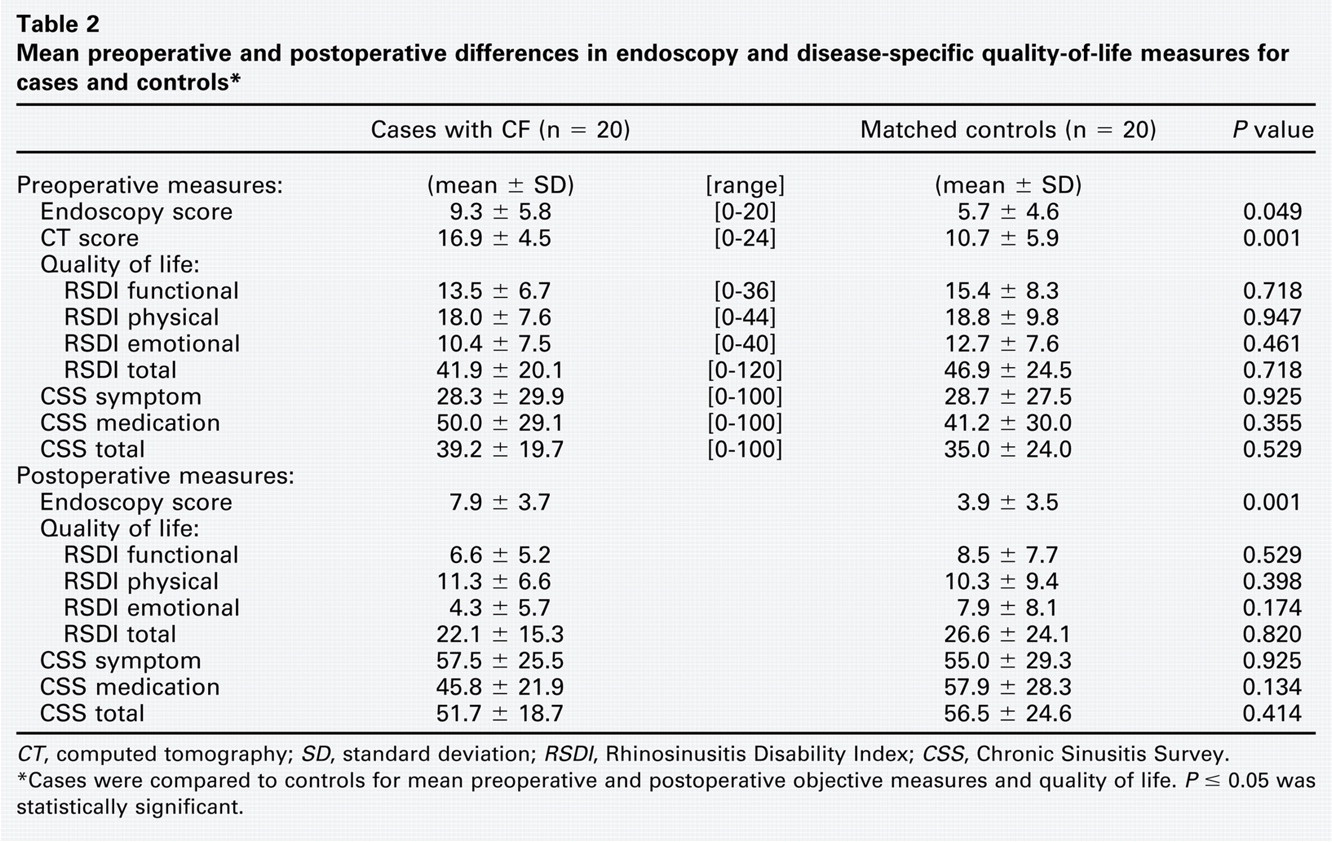
CT, computed tomography; SD, standard deviation; RSDI, Rhinosinusitis Disability Index; CSS, Chronic Sinusitis Survey.
Cases were compared to controls for mean preoperative and postoperative objective measures and quality of life. P ≤ 0.05 was statistically significant.
Mean postoperative improvement in endoscopy and disease-specific quality of life for cases and controls∗
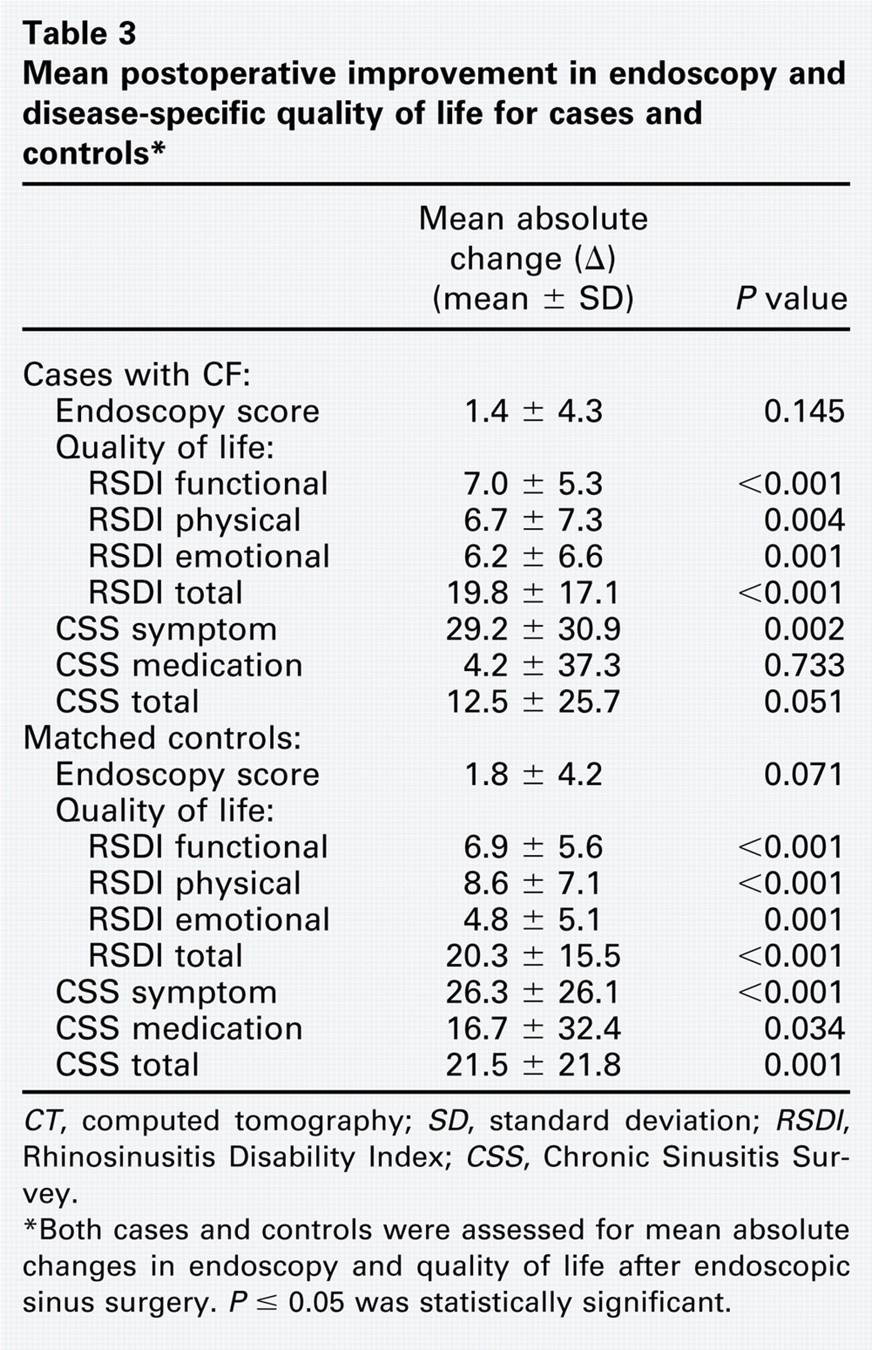
CT, computed tomography; SD, standard deviation; RSDI, Rhinosinusitis Disability Index; CSS, Chronic Sinusitis Survey.
Both cases and controls were assessed for mean absolute changes in endoscopy and quality of life after endoscopic sinus surgery. P ≤ 0.05 was statistically significant.
Disease-Specific QOL Measures
Cases with CF presented with a similar mean preoperative QoL compared to control patients (Table 2). There were no significant differences in preoperative QoL between subgroups for either total or subscale mean scores of the RSDI or CSS (P ≥ 0.355). Overall, both groups were found to have statistically significant improvement for disease-specific QoL measures, with the exception of CF case responses on the CSS medication subscale (P = 0.733; Table 3). The mean improvement on total CSS scores approached significance for the CF group (P = 0.051) compared with a larger significant improvement for control patients (P = 0.001; Table 3).
Cases with CF reported significant improvement in the RSDI subscales (all P ≤ 0.004) and the symptom subscale of the CSS (P < 0.002). Control patients were found to have improvement in all RSDI subscales (all P ≤ 0.001) and all CSS subscales (all P ≤ 0.030). No significant differences in postoperative QoL improvement were found between cases and controls (all P ≥ 0.134), indicating that both groups experience and describe similar benefit in QoL after surgical intervention for CRS symptoms.
Discussion
In this study, we evaluated the effectiveness of ESS for CRS in adult patients with comorbid CF. As expected, subjects with CF had significantly worse baseline CT and endoscopy scores as compared with control subjects with CRS. Our data suggest that adult CF patients experience significant improvement in sinonasal symptoms and QoL impairment following endoscopic sinus surgery. The magnitude of improvement is similar to that experienced by the general CRS population and is maintained approximately one year postoperatively. Furthermore, the degree of improvement on endoscopy exam is similar in the adult CF and general CRS populations up to one year after ESS. In contrast, when compared to the general CRS population, adult CF patients present with significantly worse preoperative endoscopy scores and maintain significantly worse postoperative endoscopy scores approximately one year after surgery.
Improved life expectancy has introduced new challenges in the overall management of patients with CF. 5 – 7 The past few decades have witnessed increasing numbers of adult CF patients with recalcitrant sinus disease, yet evidence-based treatment recommendations for this unique population remain elusive. This subgroup of CRS patients represents one of several challenging subtypes of CRS for which optimal management strategies remain a topic of intense investigation. 5 – 8 , 11 Management of CF patients involves a multidisciplinary approach to assess maturation of lung function at a young age and vigilant attention to preventing infectious complications. The marked heterogeneity observed, in terms of disease severity and progression, makes it difficult to accurately gauge progress and estimate prognostic factors.
Surgical intervention is often sought to improve quality of life and to attenuate the inflammatory cascade within the sinonasal complex of CF patients. 7 – 10 Keck and Rozsasi followed 26 children and adolescents with CF for a mean postsurgical follow-up period of 23 months. 16 Although they demonstrated improved symptom score, complete remission of nasal polyposis was observed in only 31 percent of patients. In fact, Yung et al reported a median interval of four years between sinus surgeries owing to polyp recurrence in their pediatric CF patients. 6 Furthermore, Rowe-Jones and Mackay reported on a 28-month follow-up of their cohort of 46 CF patients and observed that by 24 months, 50 percent of patients required another surgical intervention. 17 Interestingly, Shatz retrospectively reported marked improvement in symptoms and endoscopic findings in a cohort of 15 pediatric CF patients who underwent aggressive sinus surgery, which included a middle turbinate reduction, a Caldwell-Luc approach, and a medial maxillectomy. 18 These patients had already failed multiple endoscopic procedures. Our study is unique in that it prospectively assessed QoL and objective outcomes in adult CF patients and provides much-needed evidence to evaluate ESS as a treatment modality in this population.
While CF patients in our study demonstrated significant improvements in disease-specific QoL, there was no significant change in the medication subscale of the CSS following ESS. This is primarily reflected by the fact that CF patients continued to use antibiotics at a similar rate following surgery, demonstrating the challenge of managing ongoing infections of the upper and lower respiratory tract in this population. Conversely, the symptom subscale of the CSS demonstrated significant improvement following ESS. This change, however, was offset by the lack of improvement in the medication subscale, thereby limiting improvement in the total CSS score.
There are a number of limitations that must be taken into consideration to accurately translate the findings of this study. Generalizability of QoL outcomes may be limited due to the fact that all study subjects were enrolled within the same geographical region and were operated on by the same primary surgeon. Furthermore, we did not control for measures of adherence to medical therapy in the postoperative period, which is known to impact long-term surgical outcomes in the general CRS population. 19 The relatively small sample size may be insufficient to detect smaller mean QoL improvements and might have led to a lack of statistically significant differences between subgroups. Despite this, our study represents one of the largest prospective cohorts of adult CF patients with concurrent CRS to date.
Conclusion
Patients with CF present with more severe disease at baseline, as measured by CT and endoscopy. However, our data demonstrate that patients with CF experience similar improvement in both QoL and endoscopy following ESS for treatment of recalcitrant CRS. Future investigations should enroll a larger case population involving multi-institutional participation, and determine whether CF genotypes (ie, 8F508, R117H, etc) respond differently to medical and/or surgical intervention.