
Abstract

Embryologically, the thyroid gland originates from the lingual foramen cecum. Its migration through the neck leads to the formation of the thyroglossal tract, which degenerates during embryological life.
In abnormal migration, abnormalities may arise, such as thyroglossal duct cysts (TGDCs) and thyroid gland ectopias. Those might even be associated. 1 The Sistrunk procedure is the accepted treatment for TGDCs, but there is no standardized procedure for thyroid ectopia. We present a rare case of dual thyroid ectopy, treated by the Sistrunk procedure. This study was approved by the local institutional review board.
A 28-year-old woman was hospitalized during the third trimester of pregnancy for upper gastrointestinal bleeding. After a C-section, performed for fetal suffering, an upper gastrointestinal endoscopy revealed a tongue base mass. Thyroid function tests revealed subclinical hypothyroidism. Thyroid scan showed dual foci of uptake at the tongue base level, with no signal in the normal thyroid bed. The patient was started on levothyroxine suppressive therapy.
After six months, a follow-up MRI confirmed the dual ectopy, with one part at the base of the tongue and the second directly infrahyoid, with two nodular formations in the infrahyoid part. A follow-up thyroid function test revealed a hyperthyroid state. The hormonal treatment was adjusted, and a decision was made to do a total thyroidectomy to prevent rebleeding and evaluate the nodules (Fig 1).
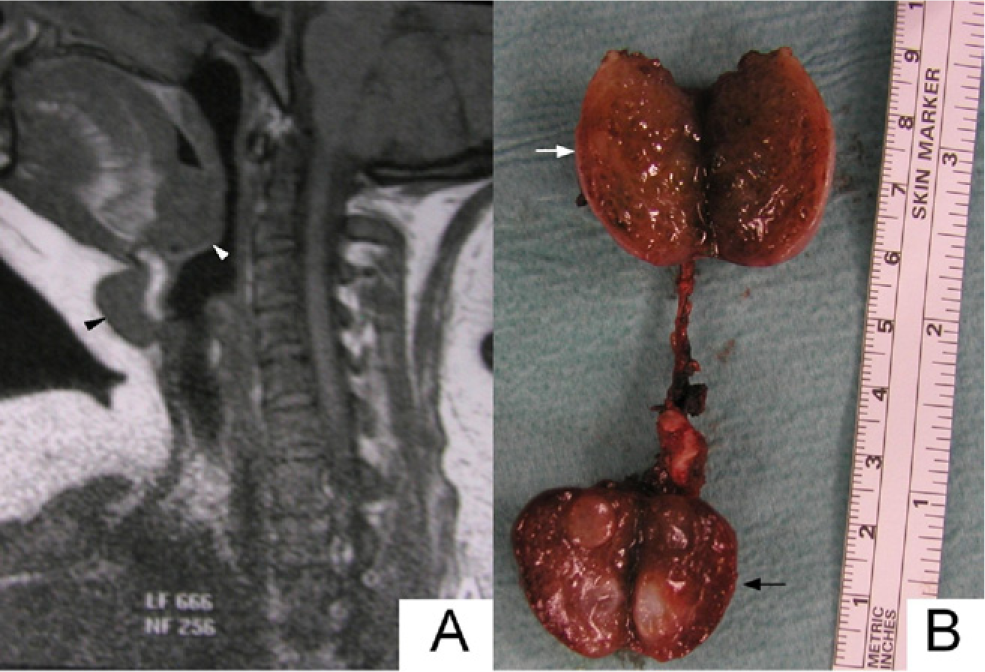
With the patient under general anesthesia, through a horizontal neck incision, the lower part of the ectopic gland, with its surrounding connective tissue, was dissected to the level of the hyoid bone. The body of the hyoid was resected and kept attached to the gland. At this level, a midline pharyngotomy was necessary to excise the upper submucosal part of the gland.
The pharyngotomy incision was closed primarily, and the wound was closed in layers. Postoperative feeding was started on the sixth postoperative day. Histopathological examination revealed normal thyroid tissue, with two follicular nodules measuring 2 and 3 cm in diameter.
Discussion
Thyroid ectopy is a rare clinical entity, with 90 percent of cases occurring at the base of the tongue. The subhyoid type is less common and is usually associated with lingual ectopy. Only 27 cases of dual ectopy have been reported to date. 2
When symptomatic, patients present with dysphagia, dyspnea, foreign body sensation, or bleeding. 3 Seventy percent of patients with a lingual thyroid have this ectopy as the only secreting tissue, with hypothyroidism in 75 percent of the patients. Cases with dual ectopy are less commonly hypothyroid. 2
The thyroid gland is known to be hyperstimulated during pregnancy. Massive bleeding is a known presentation for lingual ectopy. Nodular formations are known to develop during pregnancy, and these nodules do not completely regress after delivery. 4
There were several reasons to treat our patient with a total thyroidectomy: she had massive bleeding, nodular formations, and nonregression of the size of the gland under hormonal treatment. Lingual thyroids are usually accessed by transhyoid pharyngotomy or a transmandibular midline split of the tongue. 3
The Sistrunk procedure was described in 1920. The aim of this procedure is to excise the TGDC along with any potential residual tissue, to avoid recurrences. We believe that ectopic thyroid surgery should follow the same line of thinking, especially with double ectopy. Several reported cases of ectopic thyroid disease recurred after initial treatment and needed revision surgery or adjunctive radioactive iodine treatment. 3 , 5
Although in our case a pharyngotomy was necessary to complete the excision, the Sistrunk procedure, we believe, was an essential part of the procedure to remove any residual thyroid tissue along the thyroglossal tract to avoid recurrence. To our knowledge, this is the first time a Sistrunk procedure has been used for a dual ectopic thyroid.