
Abstract

Nasal septal surgery (NSS) in the form of submucous nasal cartilage resection or septoplasty is one of the most common operations performed in otolaryngology. As opposed to turbinate surgery, in which multiple modalities are used, the technique for NSS has remained practically unchanged since its introduction. Conventional NSS consists of an incision followed by bilateral mucosal flap elevation and septal recontouring via resection or septoplasty.1 A novel technique was introduced by Kamami2 when nasal obstruction was relieved by carbon dioxide (CO2) laser ablation of the anterior septal spur. This technological leap offers many advantages. It offers patient comfort by eliminating nasal packing, allows tailoring time because the office procedure is easily undertaken and does not require general anesthesia, and provides immediate improvement with minimal complications and possibly less pain. By eliminating conventional NSS complications, such as perforation or septal abscess, cerebrospinal fluid leak and anosmia are avoided. Because of its articulated mirrored arm and large handpiece with a nasal tip, the CO2 laser can only be used for anterior nasal spurs.2,3
We tried to overcome the limitations of the CO2 laser handpiece by using a more maneuverable laser fiber. The inexpensive tabletop mobile battery-operated diode laser is ideal for office procedures. Moreover, at a wavelength of 980 nm, this device has a high absorption rate for hemoglobin, which makes it ideal for soft-tissue applications in which good hemostasis is necessary. With a 300-μm flexible fiber, it is possible to address even the posterior spurs under the endoscopic view.
Methods
This was a multicenter retrospective study with 1000 charts reviewed for complications including perforation, crusting, synechia, bleeding, hematoma formation, or altered smell sensation. The St. Luke's-Roosevelt Hospital Center Institutional Review Board approved the study (09–040X). Patients selected for NSS included (but were not limited to) those with the following indications: sleep apnea and snoring, nasal obstruction causing breathing difficulties, rhinitis (allergic and nonallergic), and obstruction relief before endoscopic sinus surgery. Patient satisfaction was collected at follow-up visits or by telephone. Most patients were treated under local anesthesia without sedation. Nasal visualization was possible with anterior rhinoscopy and endoscopy using a 0° or 30° endoscope.
For the CO2 laser (Lumenis, Yokneam, Israel), a blackened Killian speculum and a specially designed nasal tip connected to the pharyngeal handpiece were used. The laser was set at 10 W using the SuperPulse continuous mode with a Surgitouch scanning device (Lumenis, Santa Clara, CA) with a 2-mm spot size.
The diode laser (ARC Lasers; Lumenis) was a 980-nm near infrared (NIR) laser operated in a continuous mode at 6 W. The laser was connected to a 300-μ bare and flexible fiber inserted to a specially designed handpiece. As opposed to the CO2 laser, the diode laser has to be activated in contact mode for effective tissue ablation.
The surgical technique included identification and direct transmucosal ablation of anterior or posterior cartilaginous spurs without incisions or elevation of the mucoperichondrial flaps. Bleeding was minimal, and nasal packing was not used. All the procedures were tolerated well. Patient satisfaction was a subjective improvement as expressed by the Nasal Obstruction Septoplasty Effectiveness (NOSE) questionnaire4 (any positive response regarding nasal congestion or stuffiness, nasal blockage or obstruction, troubled nasal breathing, or inability to get air) and was graded only as positive or other response. Acoustic rhinometry was used for objective confirmation in some patients.
Results
A total of 1000 laser NSSs performed in an office setting in the last 10 years were reviewed. The CO2 laser was used in 700 surgeries, and the NIR laser was used in the rest. Some patients were lost to follow-up. Fifty-two patients underwent NSS previously. Patient satisfaction was 96 percent (958/1000). Complications included crusting, which occurred in 71 percent of the patients. No septal perforation, hematoma, or alteration of smell was reported, and loss of productivity was minimal. Minor bleeding occurred in eight patients and was easily controlled. Thirteen patients had temporary altered sensation of the teeth. Seven patients developed synechia requiring secondary correction. Septal spurs before (Fig 1) and after removal (Fig 2) are shown. An instructional video is available online (Video 1, www.otojournal.org).
Discussion
When selection is careful, patients can undergo a limited laser NSS. The office setting is a safe environment, as shown by the limited complication rate associated with it.5 With the pioneer role of the CO2 laser in NSS, we could easily switch to the NIR laser, possibly with better results. The CO2 laser is a powerful laser that is the working horse in ENT practice. Hence, it may be used as an adjunct in the operating room for selected NSS. The advantages are no need of packing, a limited complication rate, possible reduced pain, a shortened operating time, and reduced operating room expenditure. The compact diode laser, while delivering less power, shows more diverse versatility with the proper handpiece in the office. Therefore, we conclude that the laser is a safe and advantageous tool for NSS for carefully selected patients.
Laser septal spur removal can achieve excellent physiologic results and patient satisfaction when held in the office, the patient need not take time off from work, and it still allows the option for additional surgery as needed. The diode laser and the CO2 laser were effective in 1000 patients. Although the CO2 laser is used when operating on anterior spurs, the diode laser can be used with posterior spurs as well. Because the mucoperichondrial flaps are not raised, septal surgical complications, such as hematoma formation, perforation, and cerebrospinal fluid leak, are avoided. Avoiding the raising of the mucoperichondrial flaps simplifies the operation, especially for the novice surgeon. The operation is performed under the endoscopic view, which allows teaching, as opposed to the classic single-surgeon's view used for septoplasty/submucous resection of the nasal septum.
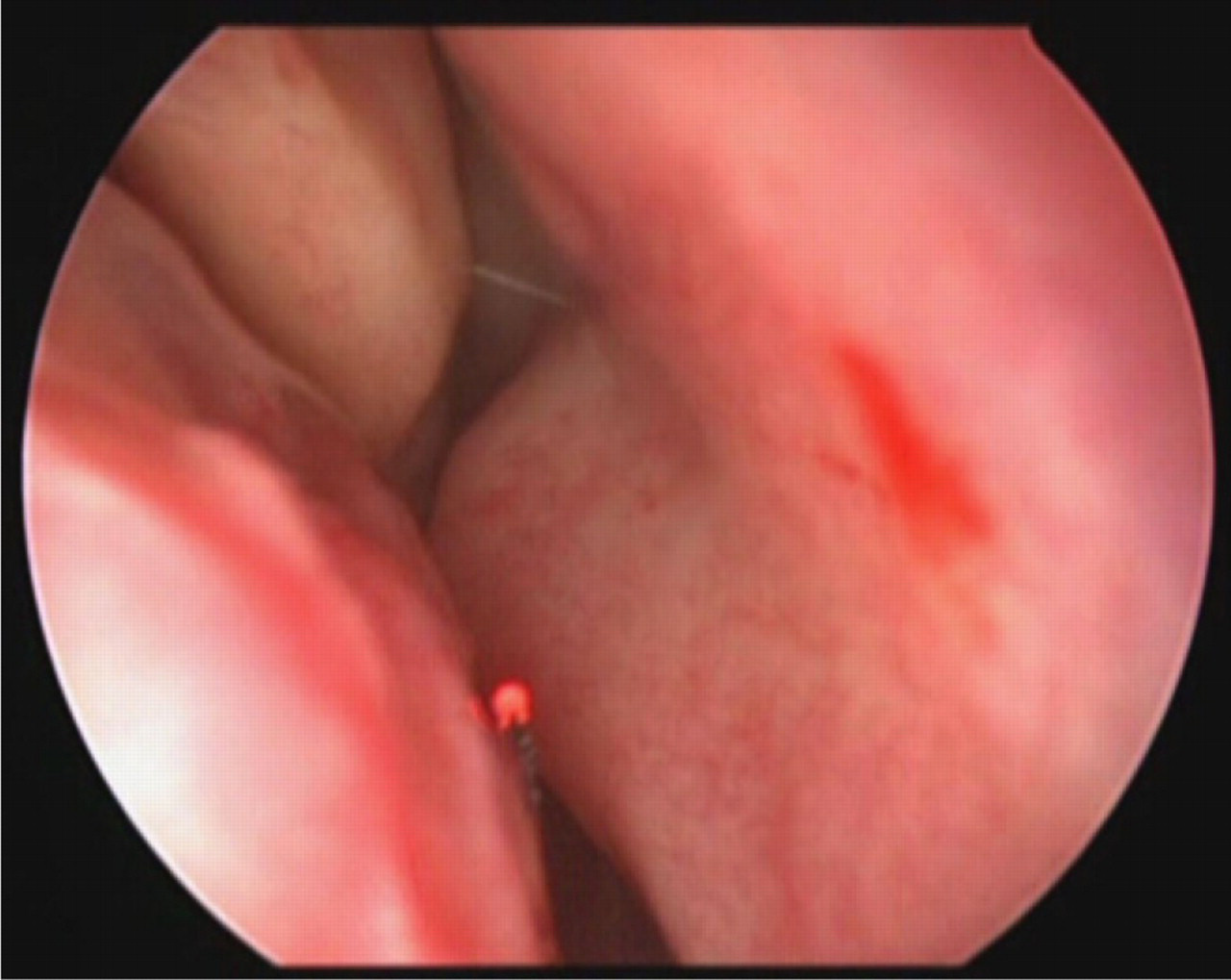
The posterior septal spur.

The septal spur ablated.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.