
Abstract
Vestibular schwannoma (VS) is caused by an overproliferation of Schwann cells of the vestibular nerve and represents approximately 6 percent of all intracranial tumors.1 The estimated incidence of VS is approximately 0.3 to 1 per 100,000 persons per year, with a mean age of occurrence of 45 to 50 years.2
The diagnosis of VS is often delayed because the disease is uncommon and the symptoms are consistent with other more frequently occurring conditions. Such a delay usually means that the tumor has been allowed to grow and ultimately compress and damage vital structures. This reduces the effectiveness of therapy and increases morbidity. Therefore, the key to diagnosis of VS is a high suspicion. In our center, an auditory brainstem response (ABR) test is usually performed initially because it is less costly and more readily available than magnetic resonance imaging (MRI). Much has been published regarding the characteristics of ABR parameters measured for the suspicion of VS. However, despite a well-characterized relation between ABR and VS, their relation to tumor extension remains to be clarified. Bilateral ABR abnormalities are seldom considered estimate parameters or in the evaluation of VS tumor size.
The goal of the present study was to analyze bilateral ABR records of patients with VS and to investigate the relation between tumor size and ABR variables in order to understand how VS affects hearing levels and the ABR.
Materials and Methods
This retrospective study, based on chart reviews, was undertaken with the approval of the Research Ethics Committee of National Taiwan University Hospital. During the period 1995 to 2005, a total of 107 patients received a diagnosis of VS at our hospital. Of these, 30 patients with complete data for the presurgical ABR examination, along with images, were analyzed in this study. The VS tumor size was estimated on the basis of MRI and computed tomography as standardized methods, according to the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS)3 and was assessed by investigators who were blind to the ABR data. The size, pure-tone average, and waveform of the ABR were reviewed. The significance of waveform anomalies was evaluated bilaterally. An evoked potential system (Nicolet; Spirit, Madison, WI) was used to measure the latencies of different ABR components. Recordings were performed with rectangular electric clicks via an insert earphone (pulse width, 100 μs; frequency, 11.1/s; sweep, 2000 stimulations) with a digital low filter at 100 Hz and a digital high filter at 3 kHz. The ABR was recorded with a two-channel system consisting of an active noninverting electrode attached to the midline of the forehead and two reference electrodes attached to the ipsilateral and contralateral earlobes; both were connected to the same input terminal of the amplifier.
Normal ABR values used in this study
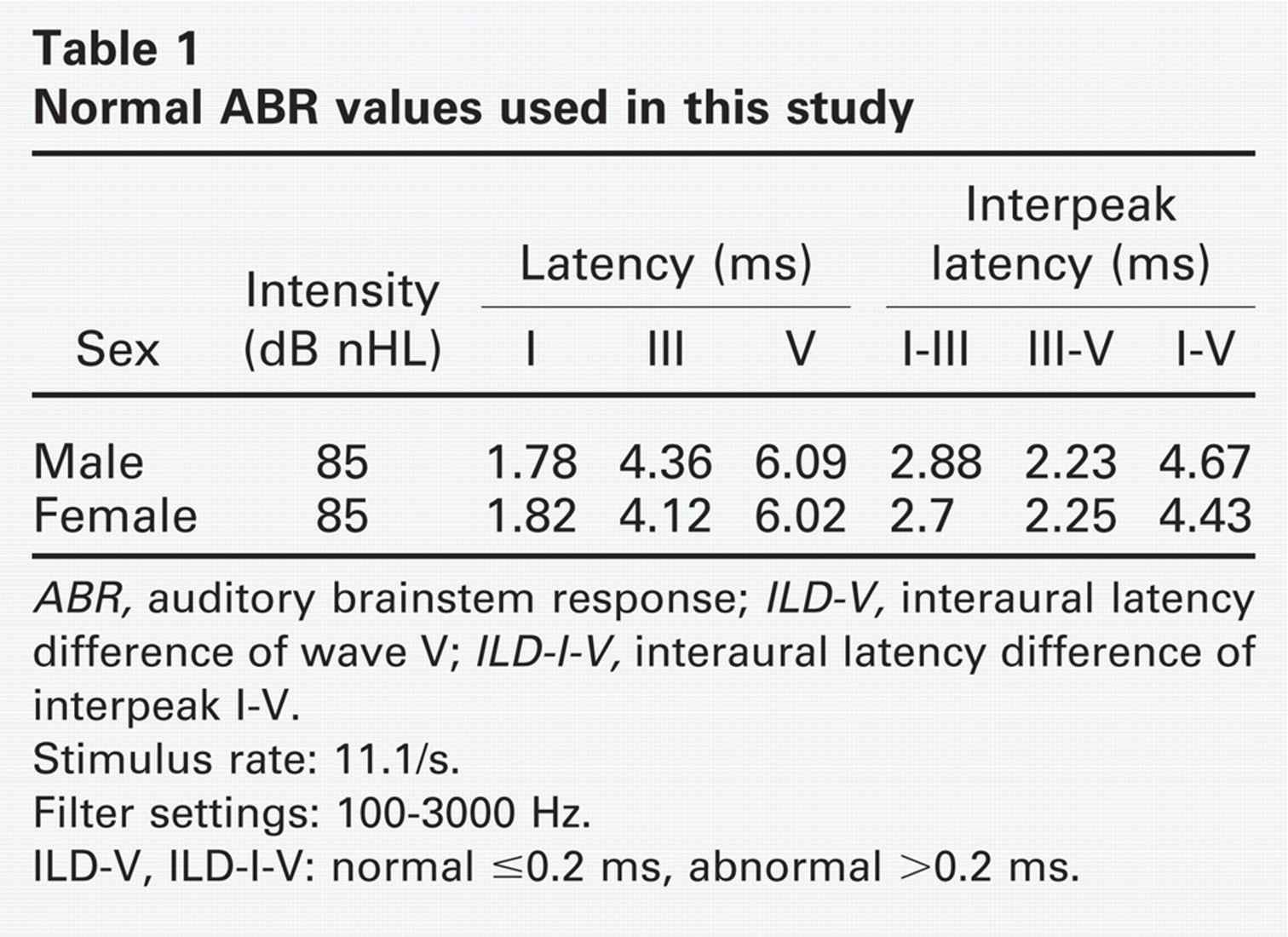
ABR, auditory brainstem response; ILD-V, interaural latency difference of wave V; ILD-I-V, interaural latency difference of interpeak I-V.
Stimulus rate: 11.1/s.
Filter settings: 100–3000 Hz.
ILD-V, ILD-I-V: normal ≤0.2 ms, abnormal >0.2 ms.
Analyzed ABR waveforms included the absolute latencies of waves I, III, and V; the interpeak latencies of waves I-III, I-V, and III-V; and the interaural latency difference (ILD) of wave V (ILD-V) and interpeak I-V (ILD-I-V). These were used as parameters for evaluating clinically relevant abnormalities of the ABR, which included prolonged absolute latencies or interpeak latencies and ILD-V or ILD-I-V longer than 0.2 ms. Prolonged absolute latencies or interpeak latencies were defined as those beyond the 95% confidence limit relative to previously established adult normative values obtained in our laboratory (Table 1, Fig 1). Complete absence of identifiable waves in the presence of adequate pure-tone average (hearing loss <75 dB) and poor waveform morphology were also considered abnormal responses.
Microsoft Office Excel 2003 and SAS 10.0 for Windows (SAS, Cary, NC) were used for data management and statistical analysis. Continuous variables are presented as mean ± standard deviation. Comparisons between groups were analyzed with the Student t-test for continuous variables and the Fisher exact test for categorical variables. Correlation between tumor size and severity of hearing loss or the total number of bilateral abnormal ABR parameters was calculated by linear regression. The predictive effect of the total number of bilateral abnormal ABR parameters on tumor size was further analyzed by multivariate linear regression with adjustments for age, sex, and pure-tone average. Statistical analysis was considered significant at P < 0.05.
Results
Patient Demographics
A total of 30 patients were included in this study. The mean age was 50 ± 14 years (range, 18–72 yrs). Patients included 17 men, with a mean age of 52.9 years, and 13 women, with a mean age of 46.6 years. Cases included 11 left, 17 right, and 2 bilateral VS tumors (both with right-side surgery and there was no cases of neurofibromatosis type 2) (Table 2). Twenty-five percent of patients developed VS before the age of 40, and 75 percent of patients were younger than 60 years.
The chief complaint at initial presentation included hearing loss (50%), tinnitus (40%), vertigo (26.7%), ataxia (16.7%), facial palsy (13.3%), and headache (3.3%), with 10 patients (33.3%) presenting with more than one symptom. Overall, the average tumor size was 2.48 ±1.31 cm, and 40 percent of the tumors were smaller than 2 cm. Twenty-four patients (80%) underwent surgical excision, and 6 (20%) selected observation. Among the observation group, one patient had a tumor size larger than 5 cm (the patient's family refused surgery owing to the advanced age and general weakness of the patient), three had tumors smaller than 2 cm, and two had tumors located in the internal acoustic canal. In the observation group, the average tumor size was 1.67 ± 1.57 cm. In the facial palsy group (4 patients), the tumor size was 4 cm in one case, 3 cm in two cases, and 2 cm in one case.
Ipsilateral ABR Waves
All 30 patients had abnormal ipsilateral ABR findings. Statistical analysis determined that symptoms of hearing impairment, tinnitus, vertigo, facial palsy, and headache had no significant relation to waveform change. In contrast, symptoms of ataxia were related to ipsilateral and contralateral changes of interpeak III-V latency (P = 0.044 and P = 0.002, respectively). Overall, the prevalence of abnormal ABR parameters of wave I was 66.7 percent, that of wave III was 76.7 percent, that of wave V was 96.7 percent, that of interpeak I-III latency was 56.7 percent, that of interpeak III-V latency was 63.3 percent, that of interpeak I-V latency was 90 percent, that of ILD-V was 93.3 percent, and that of ILD-I-V was 100 percent (Table 3). In this series, 90 percent of the patients had more than 3 abnormal ipsilateral parameters, and the most commonly affected parameters were ILD-I-V (100%) and the absolute latency of wave V (96.7%).
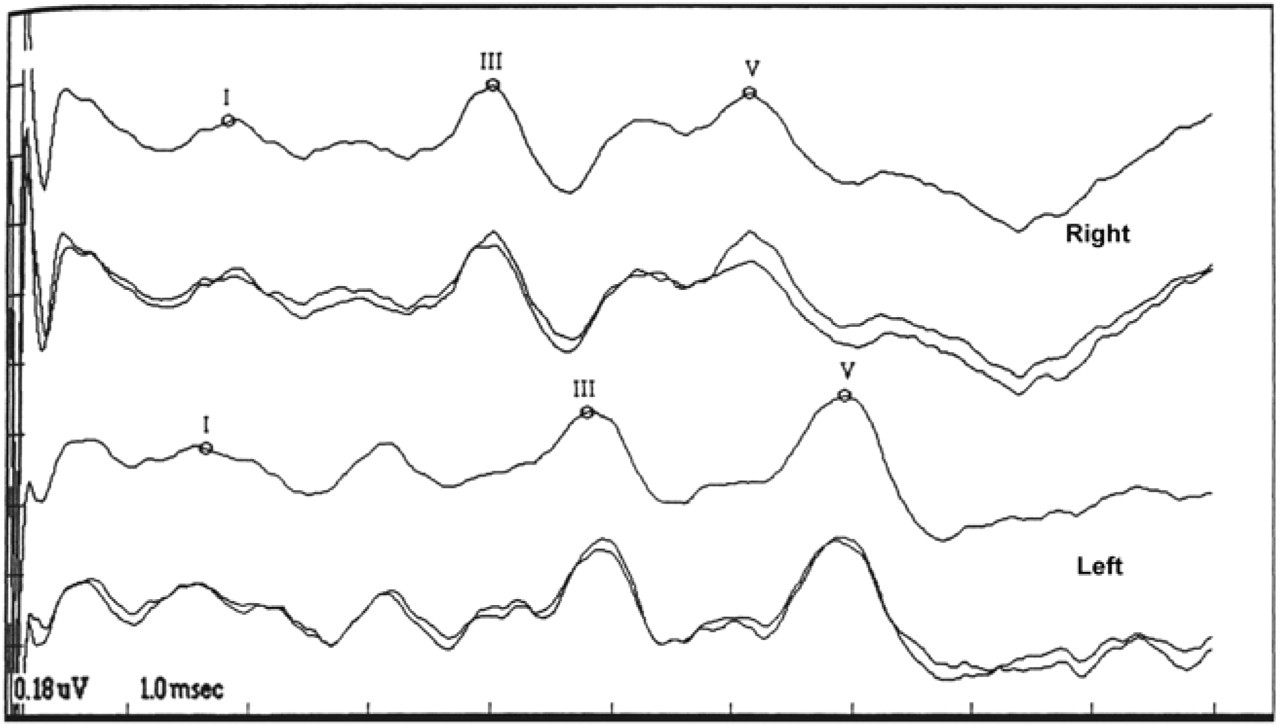
The auditory brainstem response of a 37-year-old man showed delayed wave III, wave V, and prolonged interpeak latency of I-III and I-V in his left ear. The interaural latency difference of wave V is also beyond the normal limit. The image study and operational finding confirmed a 3-cm tumor at left cerebellopontine angle.
Contralateral ABR Waves
Twenty-three patients (76.7%) had an abnormal contralateral ABR. However, in patients with a tumor size smaller than 1 cm, the prevalence of abnormal contralateral ABR was only 28.6 percent (2/7). In patients with a tumor size of 2 cm, the prevalence was 50 percent (6/12), and in patients with a tumor size larger than 2 cm, it was 94.4 percent (17/18). For all 30 patients, the prevalence of abnormal contralateral ABR parameters of wave I was 56.7 percent, that of wave III was 36.7 percent, that of wave V was 56.7 percent, that of interpeak I-III latency was 13.3 percent, that of interpeak III-V latency was 36.7 percent, and that of interpeak I-V latency was 20 percent (Table 4). The most commonly affected contralateral ABR parameters were latencies of waves I and V.
Patient demographics and clinical characteristics
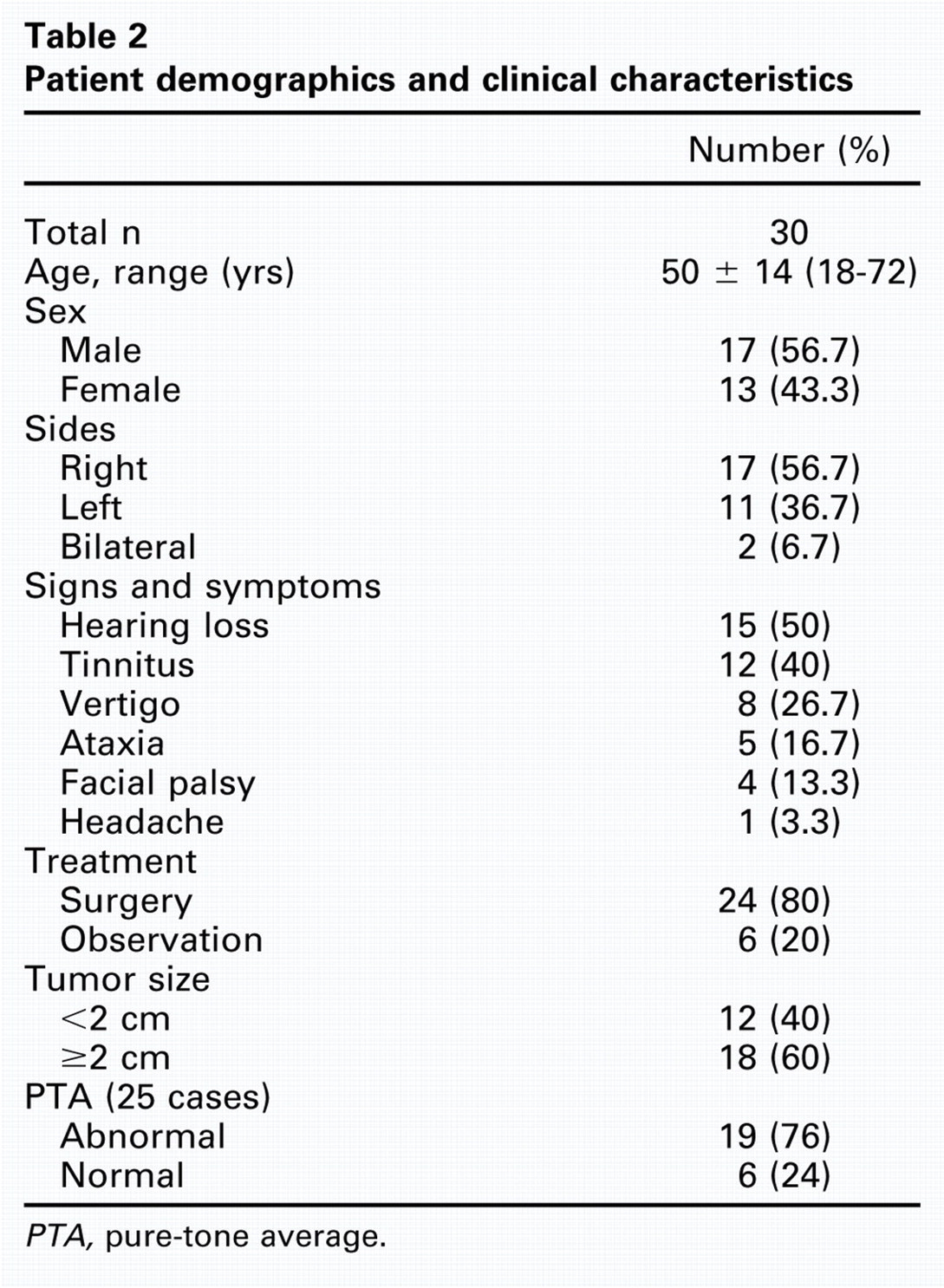
PTA, pure-tone average.
The prevalence of abnormal ipsilateral ABR parameters and their relation to the size of vestibular schwannoma
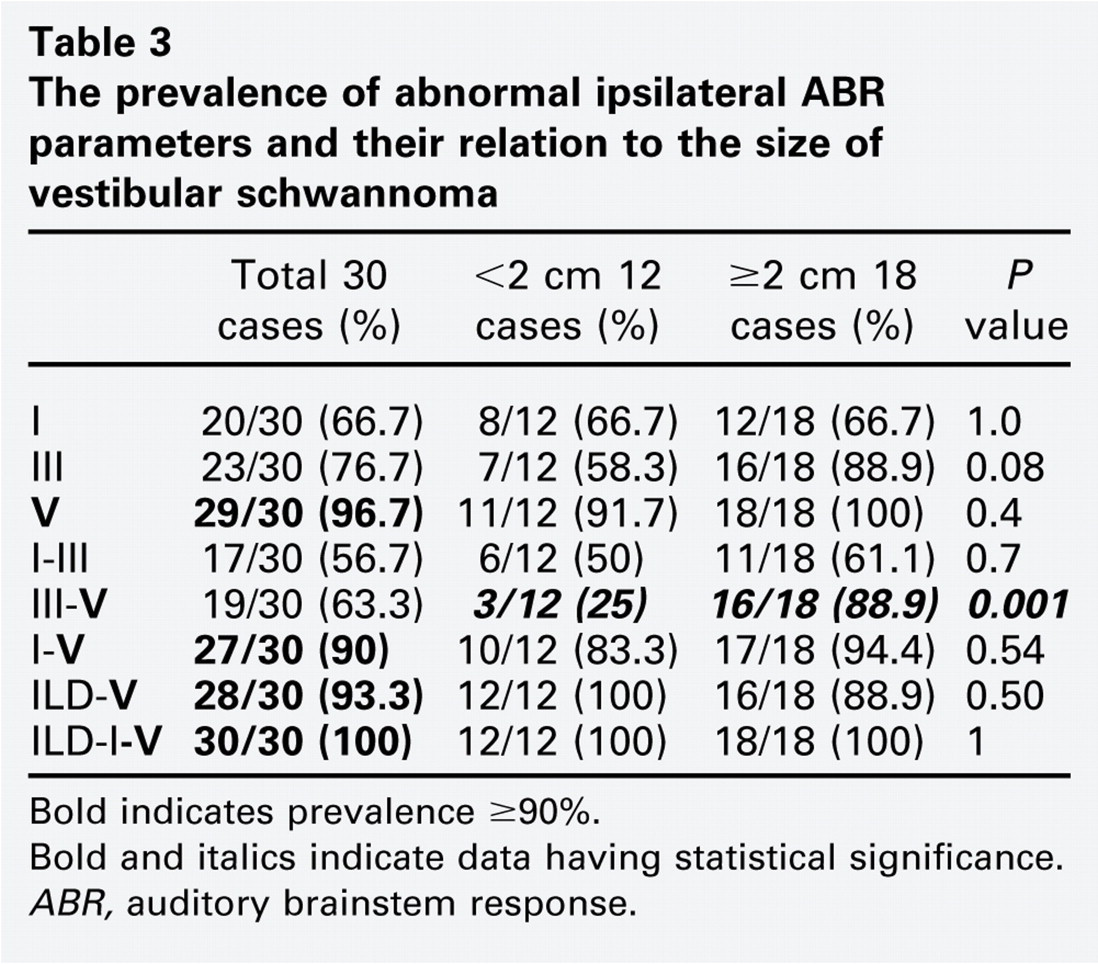
Bold indicates prevalence ≥90%.
Bold and italics indicate data having statistical significance.
ABR, auditory brainstem response.
Tumor Size and Audiometric Threshold
A positive linear correlation was noted between ipsilateral pure-tone average and tumor size (R2 = 0.2516, P = 0.0106) (Fig 2). The correlation remained significant after adjustment for age and sex (P = 0.026).
Tumor Size and ABR Parameters
A relation between tumor size and waveform changes was apparent. Comparing tumor sizes smaller than 2 cm and tumor sizes greater than or equal to 2 cm, there was a significant difference in ipsilateral interpeak III-V latency (25% vs 88.9%, P = 0.001) (Table 3). At a tumor size smaller than 2 cm, the prevalence of abnormal ipsilateral ILD-V and ILD I-V parameters both reached 100 percent. The relation between tumor size and contralateral ABR indicated that when comparing tumor sizes smaller than 2 cm and tumor sizes greater than or equal to 2 cm, there were significant differences in the absolute latency of contralateral wave V (25% vs 77.8%, P = 0.008) and the contralateral interpeak III-V latency (8.3% vs 55.6%, P = 0.018) (Table 4).
Comparison of the total number of bilateral abnormal ABR parameters (which included a prolongation of absolute latency or interpeak latency, ILD-V or ILD-I-V longer than 0.2 ms, a complete absence of identifiable waves, or poor waveform morphology) and tumor size indicated a positive linear correlation (R2 = 0.303, P = 0.004) (Fig 3). Adjusting for age, sex, and pure-tone average, correlations between the total number of bilateral abnormal ABR parameters and tumor size remained statistically significant (P = 0.0173).
The prevalence of abnormal contralateral ABR parameters and their relation to the size of vestibular schwannoma
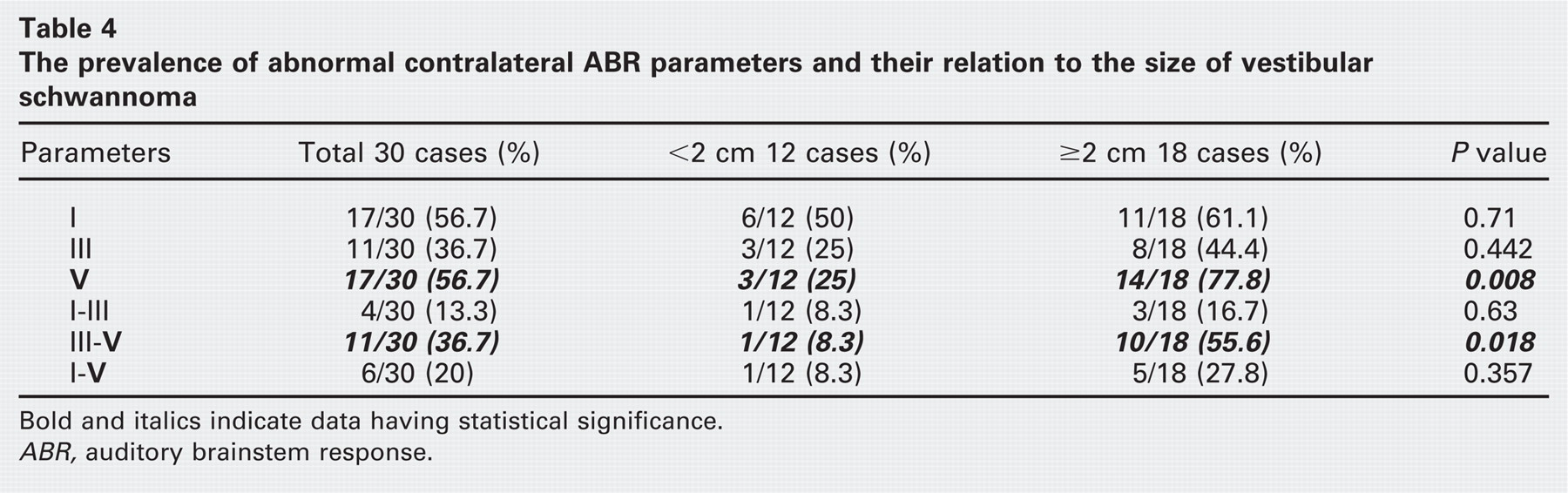
Bold and italics indicate data having statistical significance.
ABR, auditory brainstem response.
Discussion
For ABR results to be classified as abnormal, physicians rely on different methods and criteria. In 1977, Selters and Brackmann4 recommended using measurements of ILD-V. However, since then, nearly every author has suggested different criteria and has reported different predictive values. From a review of the literature,5–7 an ABR morphology suggestive of a retrocochlear lesion includes one or more of the following findings: (1) prolonged ipsilateral absolute latency of wave V, (2) prolonged interpeak I-III, I-V, or III-V latency, and (3) ILD-V or ILD-I-V longer than 0.2 to 0.4 ms. Which of these parameters is more reliable for identification of VS is an important issue because differences in methodology result in vastly different predictive values. Dornhoffer et al8 required an abnormality of ILD-V of 0.4 ms and an absolute latency of wave V longer than 5.9 ms and documented the prevalence of abnormal ABR as 93 percent. Musiek et al9 analyzed interpeak I-III, III-V, and I-V latencies as well as ILD-V and concluded that although the ILD is more sensitive than the interpeak measurement, when the ILD is unobtainable, one would be dependent on interpeak latency measurements for diagnostic ABR information. Schmidt et al10 used ILD-I-V and ILD-V longer than 0.2 ms as abnormal criteria, and their reported positive rate was 90 percent. Selters and Blackmann4 found ILD-V abnormalities in 97 percent of patients with VS, similar to Josey et al,11 who reported a 97 percent detection rate. Kanzaki et al12 compared various ABR parameters and found that ILD-V and ILD-I-V less than 0.2 ms yielded the lowest false-negative rates of all of the parameters examined. Also in our present study, regardless of tumor size, all of the patients showed abnormal ipsilateral ILD-I-V.
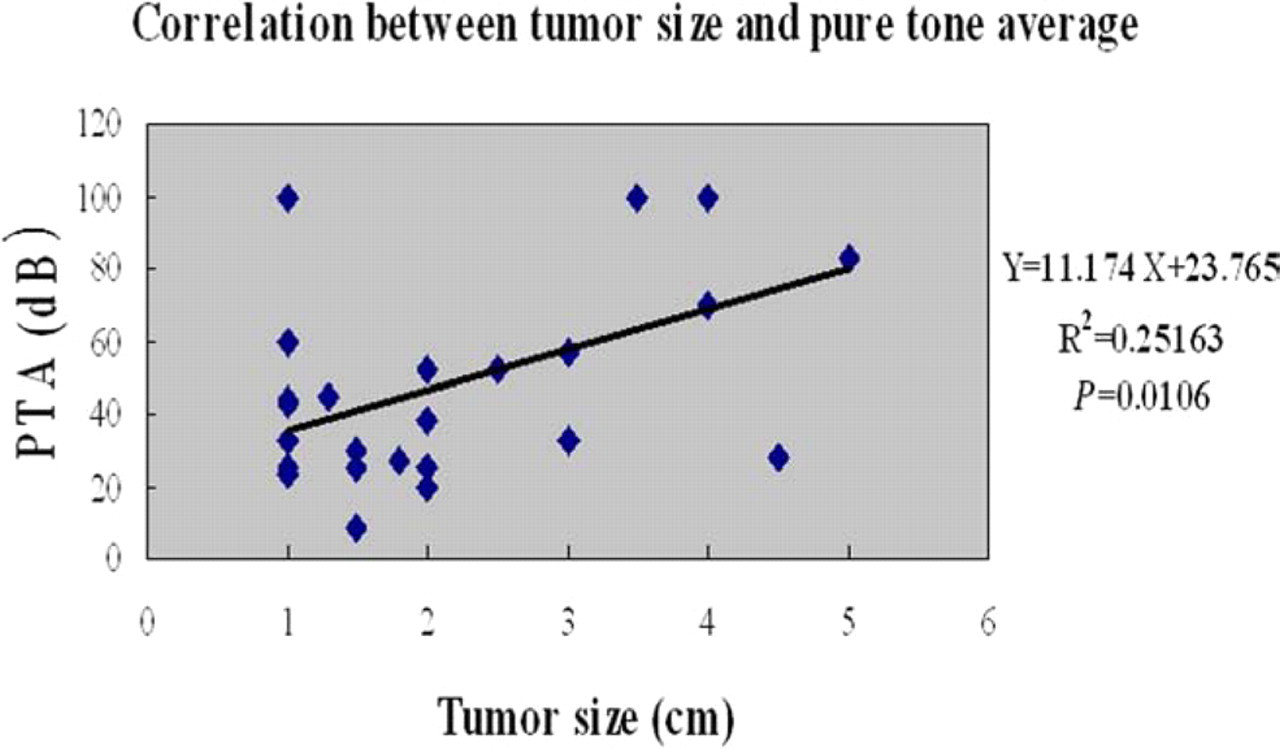
The correlation between pure-tone average (PTA) and tumor size, indicating a linear correlation.
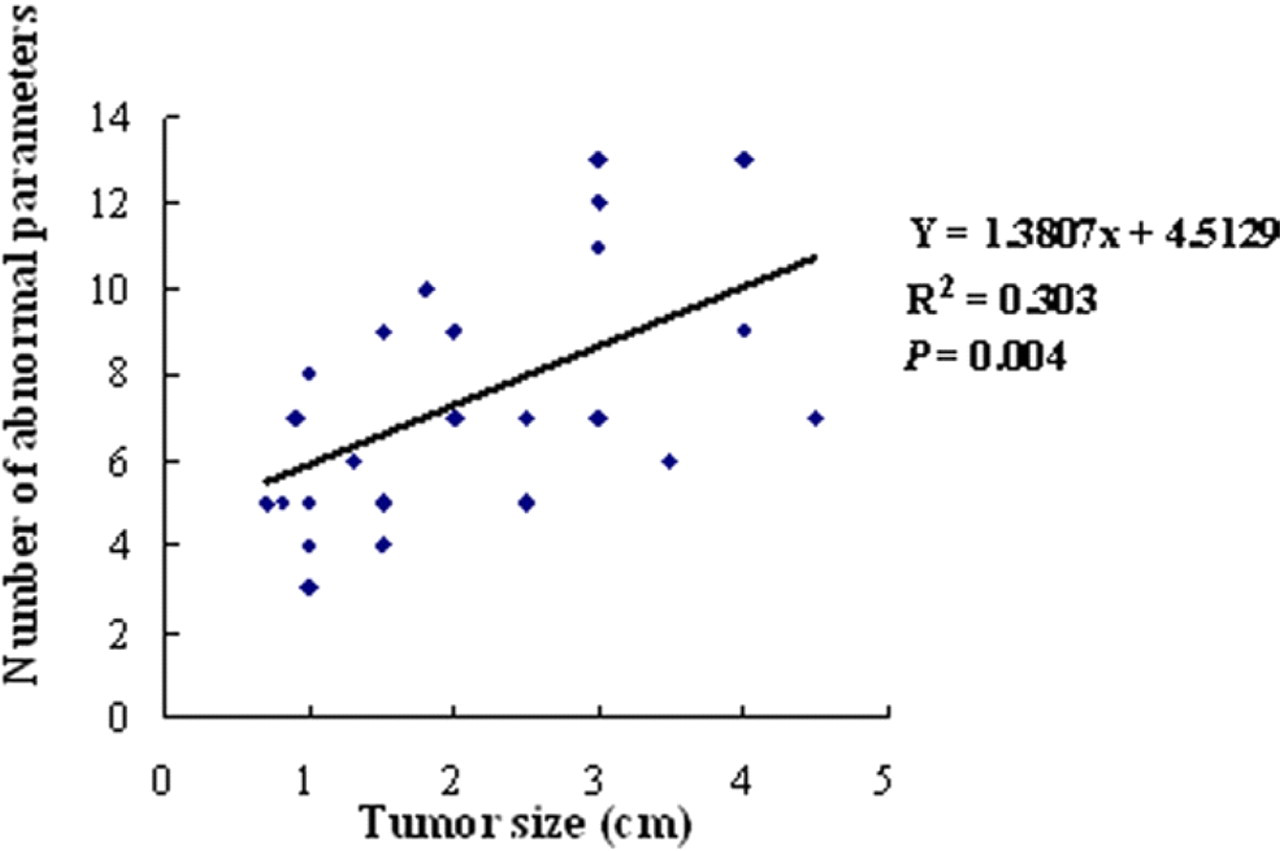
The correlation between bilateral abnormal auditory brainstem response parameters and tumor size, indicating a linear correlation.
Several researchers13–15 have reported ABR abnormalities recorded contralateral to the tumor side. Nodar and Kinney15 reported that 34.2 percent of their patients with cerebellopontine angle tumors larger than 2 cm had abnormal contralateral ABR readings. Musiek and Kibbe16 reviewed contralateral ABR parameters in 15 patients with VS, and 80 percent demonstrated abnormalities in waves IV and V. Johnson and Selters17 found that in patients with a VS tumor size larger than 3 cm, 52.4 percent had an abnormal interpeak III-V latency contralateral to the tumor. In our present series, 76.7 percent of all patients had an abnormal contralateral wave, and this prevalence increased to 94.4 percent in patients with a tumor size larger than 2 cm. The most frequent changes observed in our results were in contralateral wave I (56.7%) and contralateral wave V (56.7%). When the tumor size was larger than 2 cm, there was a significantly higher prevalence of abnormal wave V and interpeak III-V latencies. Therefore, if an abnormal contralateral waveform is found in wave I or V, the possibility of VS should be suspected, and an abnormal contralateral interpeak III-V latency and wave V suggests that the tumor size may be larger than 2 cm.
Most reports have suggested that ABR parameters do not predict tumor size. In the literature, bilateral ABR abnormalities are seldom considered simultaneously. In the present study, the number of bilateral abnormal ABR parameters was significantly correlated with tumor size. The predictive effect of the total number of abnormal ABR parameters from both sides persisted with adjustments for age, sex, and pure-tone average (P = 0.0173). To our knowledge, a correlation between bilateral abnormal ABR parameters and tumor size has not been reported. Our observation suggests that when both the ipsilateral and contralateral abnormal number of ABR parameters is considered as a presage factor, the predictive value of ABR for tumor size will increase. That is, as the sum of the ipsilateral and contralateral abnormal parameters increases, tumor size will also increase.
Audiometric parameters are not generally used as predictive factors for tumor size. However, a study of pure-tone audiograms and MRI measurement of tumor size showed a significant correlation (P = 0.001) in association with low-frequency sensorineural hearing loss.18 Recently, Day et al19 showed a trend of correlation between tumor size and audiographic configuration. Massick et al20 reported a significant linear correlation (P < 0.0001) between pure-tone average and change in tumor volume in vestibular schwannoma (being managed with observation). In the present study, our analysis confirmed a linear correlation between deterioration of pure-tone average and tumor size. Our observations suggest that an increase in tumor size may result in an increase in pure-tone average.
The main limitations of this study are that it was retrospective and included a relatively small number of patients. In addition, the criterion of ILD less than 0.2 ms is likely to increase sensitivity, but also reduce specificity. These issues, and analysis of the cost of ABR versus MRI, are beyond the scope of the present study. A point of caution regarding the conclusions from this study involves the measurement of tumor size. The ideal method of calculating tumor size is by volumetric analysis rather than two-dimensional assessment. Unfortunately, facilities to determine tumor volume were not available to us. To confirm the relation between ABR parameters and tumor size, a large, longitudinal, prospective study will be required.
Conclusion
In the present study, an ILD-I-V longer than 0.2 ms was an important parameter for the identification of VS. Prolonged ipsilateral interpeak III-V latency and contralateral wave V latency and interpeak III-V latency were associated with a tumor size potentially larger than 2 cm. The total number of abnormal bilateral ABR parameters was strongly correlated with tumor size.