
Abstract
Over the last 30 years, great progress has been made in the management of pediatric subglottic stenosis (SGS). Improvement in the care of premature newborns as well as infants with comorbidities has resulted in an increasing incidence of acquired SGS due to prolonged intubation. In all of the published series from different centers, partial cricotracheal resection (PCTR) in infants and children has shown excellent results for the most severe grades (III and IV) of SGS. PCTR has progressively gained global acceptance as a superior therapeutic alternative to laryngotracheal reconstruction (LTR) for grade III and IV SGS, according to the Myer-Cotton classification.1–6 Nevertheless, the appropriate age and weight for an infant to be considered a candidate for such an operation remains a matter of debate. The goal of early decannulation, with its evident benefits on the child's development and quality of life, is counterbalanced by the risk of potential complications or surgical failures due to the small size of the airway and uncertainties concerning the growth development of the larynx after such a procedure. Inevitably, the “optimal time” to perform this kind of operation is questioned. Some very encouraging results have been published by Johnson et al7 and by Garabedian et al8 in their series of children aged less than two years and weighing less than 10 kg who underwent PCTR for the correction of SGS.
This article aims at contributing to the analysis of the specific characteristics and long-term outcome of PCTRs performed in children weighing less than 10 kg. We compared the safety and efficacy of these operations to those of a group of older children weighing more than 10 kg.
Patients and Methods
This study was approved by the Institutional Review Board of the University Hospital (CHUV), Lausanne, Switzerland.
Study Group
From a prospectively collected database, a retrospective study was performed by searching the files of the first 101 consecutive children who underwent PCTR at our institution over the last 30 years (1978–2008).
We identified 36 children (21 males, 15 females) weighing less than 10 kg at the time of surgery. Their mean age was 16 months and their mean weight was 8.8 kg (range 4.4–9.9 kg). Seven children were between two and three years of age, 18 were between one and two years of age, and 11 were less than one year of age at the time of surgery. The majority of children older than one year belonged to the group of severely premature babies.
The etiology of the stenosis was considered congenital in 10 (28%), acquired in 16 (44%), and mixed (acquired on congenital) in the remaining 10 (28%) children. The majority of these children (27/36, 75%) presented with a grade III SGS according to the Myer-Cotton classification. Eight (22%) children presented with a grade IV SGS, and only one (3%) presented with a grade II SGS. The stenosis was purely subglottic in 26 (72%) children. A glottic involvement was present in the other 10 (28%) children: four children presented with a complete fusion of vocal folds with 1 to 2 mm of residual lumen diameter, another four presented with an anterior fusion of vocal folds, and two presented with a posterior inter-arytenoid stenosis.
Previous treatment had been performed on seven (19%) children referred to our institution for salvage surgery (1 failed LTR, 1 failed T- tube, and 5 failed endoscopic laser treatments). Primary PCTRs were performed in the other 29 (81%) children.
Concerning their medical history, 14 (39%) children were born prematurely, with a gestational age ranging from 25 to 36 weeks (mean 29 wks). Children known for congenital syndromic or nonsyndromic anomalies and other comorbidities represented 56 percent (20 cases) of the whole group (Table 1).
Control Group
The group of 65 children weighing more than 10 kg, to which the study group was compared, presented the following characteristics. Their mean age was seven years (range 22 mo to 16 yrs). The subglottic stenosis was of acquired origin in 40 (62%), of congenital origin in seven (11%), and of mixed etiology in 18 (27%). Isolated subglottic stenosis was identified in 41 (63%) patients. A glottic involvement was present in 24 (37%) patients. Twenty-nine (45%) of these patients had undergone previous endoscopic (14) and open (15) surgeries. The other 36 (55%) patients had PCTR as their primary treatment. According to the Myer-Cotton classification, there were 25 (38%) grade IV SGSs, 37 (57%) grade III SGSs, and three (5%) grade II SGSs. The percentage of children presenting with associated congenital anomalies or comorbidities reached 42 percent of this group.
Associated malformations, comorbidities, and syndromes of the group of children weighing less than 10 kg (n = 20/36 [56%])
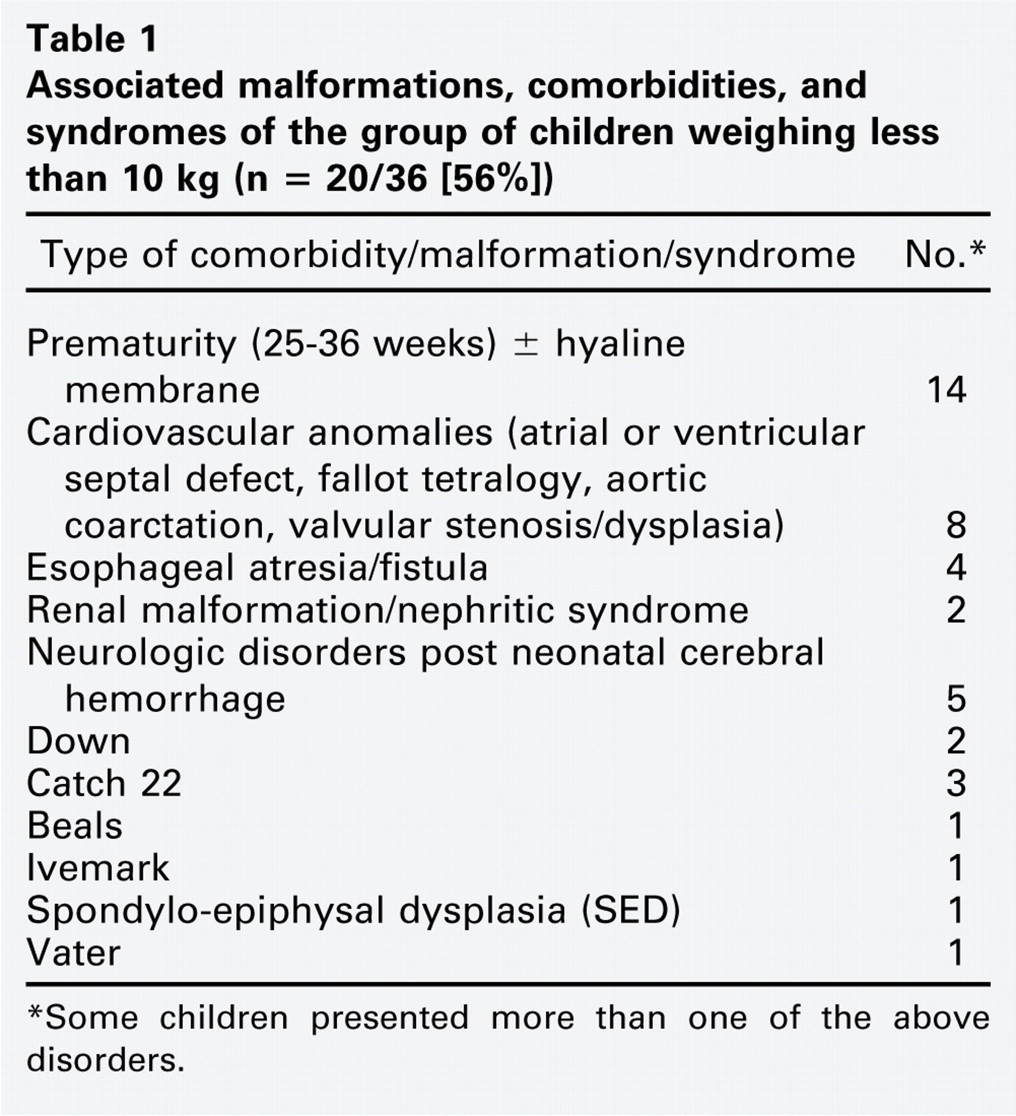
∗Some children presented more than one of the above disorders.
Group Comparison—Statistical Analysis
The Kaplan Meier method and the log-rank test were used to examine “time to decannulation” hazard ratio differences in the two weight groups (<10 kg or >10 kg). The test was also carried out adjusting for single-stage and double-stage procedures. Cox regression analysis was carried out to examine the influence of the following parameters on the time of decannulation: sex, grade of stenosis, associated anomalies and comorbidities, previous treatment, type of surgery (single-stage or double-stage PCTR), and complications requiring revision surgery before decannulation. The proportional hazards assumption did not hold for “stage technique” according to the Schoenfeld residual test and graphs and was used as a stratification variable. The variables with a P value <0.20 were used in the model and were tested with backward likelihood ratio elimination (P < 0.05). Possible interactions as well as changes in the effect of the previously nonsignificant variables were examined.
The homogeneity of the two weight groups was also controlled by the χ2 test examining comorbidities, revision surgery, grade of SGS, glottic involvement, and the type of PCTR proportions between them.
Cochran's and Mantel Haenszel tests as well as the estimation of the odds ratio were used to examine the correlation between decannulation rates and children's weight (<10 kg or >10 kg), controlling for either single-stage or double-stage technique, respectively. Data were analyzed using SPSS version 15.0 (SPSS Inc, Chicago, IL). A P value of <0.05 was considered significant.
Long-Term Outcome Evaluation
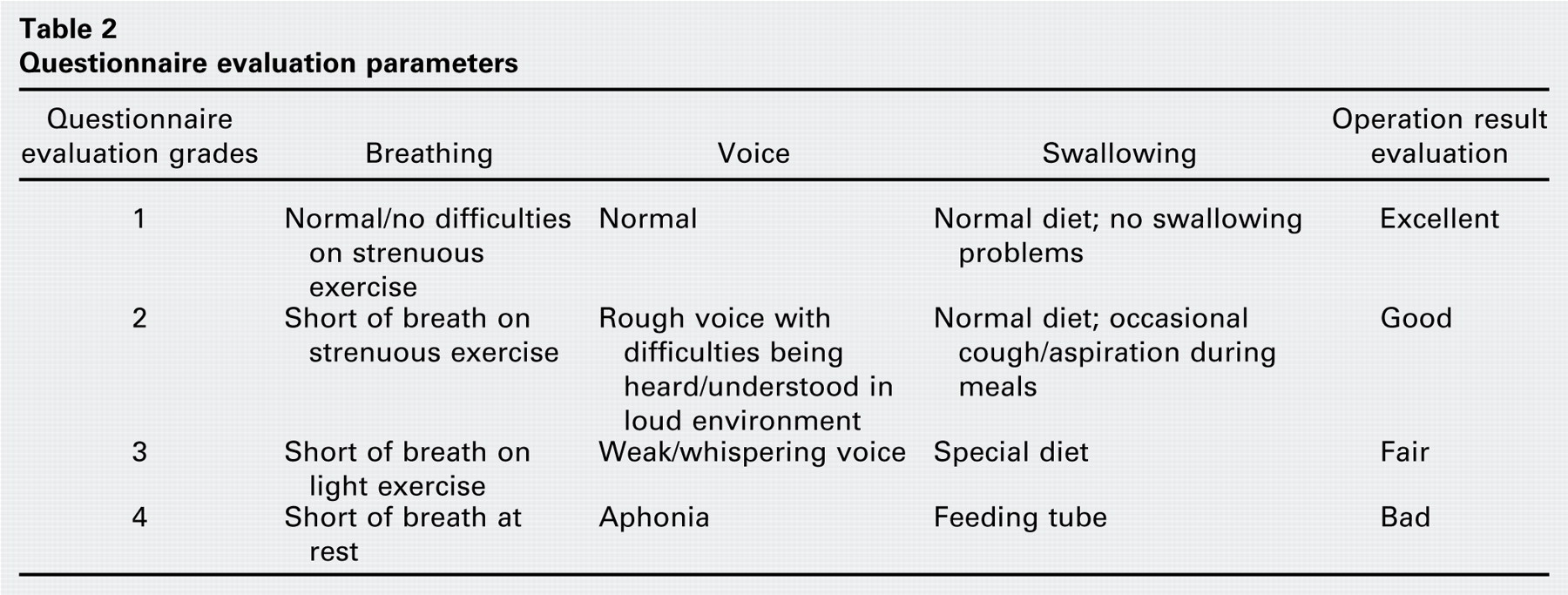
Questionnaires assessing the functional outcome in terms of breathing, voice, swallowing, and overall satisfaction were sent to the patients' families. These parameters were rated in a four-grade scale, as presented in Table 2. A minimum one-year follow-up was the sole criterion for inclusion in the long-term evaluation. This criterion was chosen because a previous study (Jaquet et al3) had revealed that reproducible and long lasting results were obtained when the postoperative outcome at three months was judged as good or excellent. Two of the patients had reached adulthood, and they completed the questionnaires by themselves. For younger patients, the questionnaires were filled out by their parents. Data concerning patients who did not respond to the questionnaire were based on our latest clinical and endoscopic evaluation or on the examination done by the local ENT specialist who continued to follow these patients.
Questionnaire evaluation parameters
Results
Children Weighing Less than 10 kg
A single-stage procedure was performed in 27 (75%) patients, with a mean period of 10 days (range 5–21 d) until final extubation. Two patients needed anastomotic revision before eventual extubation due to a partial dehiscence of the anastomosis. Another two patients needed a secondary temporary tracheotomy before final decannulation. The first of these two patients needed revision surgery for recurrent posterior glottic stenosis. He underwent a posterior cricoid split and costal cartilage graft. Decannulation was achieved 22 months after the initial PCTR. The second case in this group was a male patient with retrognathia responsible for oropharyngeal obstruction in the context of Beals syndrome.9 The final decannulation was achieved 31 months after PCTR, once the patient had successfully undergone distraction osteogenesis of the lower mandible and supra-glottoplasty. The decannulation rate for single-stage PCTR was 100 percent (27/27).
Nine children underwent a double-stage procedure. In three of them, the surgery was associated with a posterior cricoid split with costal cartilage graft and stenting by the LT-mold (laryngotracheal stent).10 The other six children underwent a double-stage PCTR, with posterior subglottic scar tissue excision and LT-mold stenting in two of them.
Of these nine children, five were decannulated within six months, one within 20 months, one is still awaiting decannulation, and two died nondecannulated. The first of these two children had congenital spondylo-epiphysal dysplasia (SED)11 that was diagnosed only during the postoperative period, and he died of respiratory insufficiency at home after PCTR while he was still tracheotomy-dependent. The second child died at home from cannula obstruction one year after surgery. The patient that is still awaiting decannulation presents a central coordination disorder secondary to neonatal cerebral hemorrhagia, resulting in major laryngospasms preventing decannulation even though the airway size could permit it. In the double-stage PCTR group, six out of nine (67%) children are presently decannulated. The current overall decannulation rate for the whole group of children weighing less than 10 kg is 92 percent (33/36 cases).
Children Weighing More than 10 kg
The group of children weighing more than 10 kg presented the following operative data: 57 percent (37/65) underwent a single-stage procedure and 43 percent (28/65) underwent a double-stage surgery. Revision surgery before final decannulation was necessary in 14 percent (9/65) of the children (posterior cricoid split and costal cartilage graft in 4, reinforcement of the anastomosis in 2, and revision PCTR in 3).
In the single-stage group, the mean time until extubation was 10 days. One patient needed a temporary secondary tracheotomy and was finally decannulated four months later. Another patient needed a tracheotomy after surgery and underwent a second PCTR for restenosis. The final decannulation was achieved nine months after the first surgery. Another patient who needed secondary tracheotomy died from cannula obstruction at home four months after surgery. The patient who is still tracheotomy-dependent and who had undergone revision PCTR is known to have neurologic dysfunction and respiratory insufficiency due to campomelic dystrophy.12 Decannulation rate for the single-stage subgroup is 95 percent (35/37).
In the double-stage group, 13 patients reached decannulation within six months, five within one year, and five in more than one year (these last patients needed revision surgery). One patient included in our earlier series (from 1980) is still tracheotomy-dependent due to restenosis. Four patients undergoing surgery in the last two years are still awaiting decannulation. Decannulation rate for the double-stage subgroup is 82 percent (23/28).
Cox regression results: variables in the equation
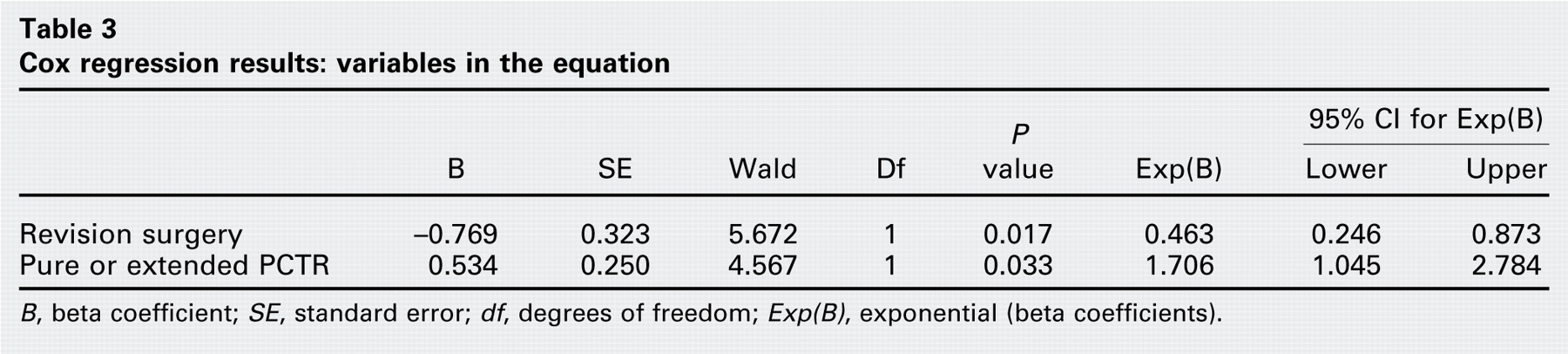
B, beta coefficient; SE, standard error; df, degrees of freedom; Exp(B), exponential (beta coefficients).
The present overall decannulation rate for the whole group of children weighing more than 10 kg is 89 percent (58/65 cases).
Statistical Analysis
Statistical analysis comparing the two groups (<10 kg and >10 kg) did not show any significant differences in terms of time to decannulation, neither when each group was analyzed as a whole (P = 0.473) nor when the analysis was adjusted to the type of surgery (single stage or double stage, P = 0.463) (Fig 1). The χ2 test did not show any significant differences in proportions of the aforementioned parameters (revision surgery, P = 0.312; comorbidities, P = 0.933; glottic involvement, P = 0.618; grade of stenosis, P = 0.321; type of PCTR, P = 0.717) between the two cohorts.
Cox regression analysis showed no influence of sex, grade of stenosis, associated congenital anomalies and comorbidities, single-stage or double-stage surgery, or previous treatment on the hazard ratio of the time until final decannulation for the two groups.
Irrespective of the group, a significant P value (0.033) was found when comparing the influence of PCTR for isolated SGS and extended PCTR for glotto-subglottic stenosis on the time to decannulation. Revision surgery also showed statistical significance (P = 0.017) for the time to decannulation. These two factors are known to prolong the time until final decannulation (Tables 3 and 4).
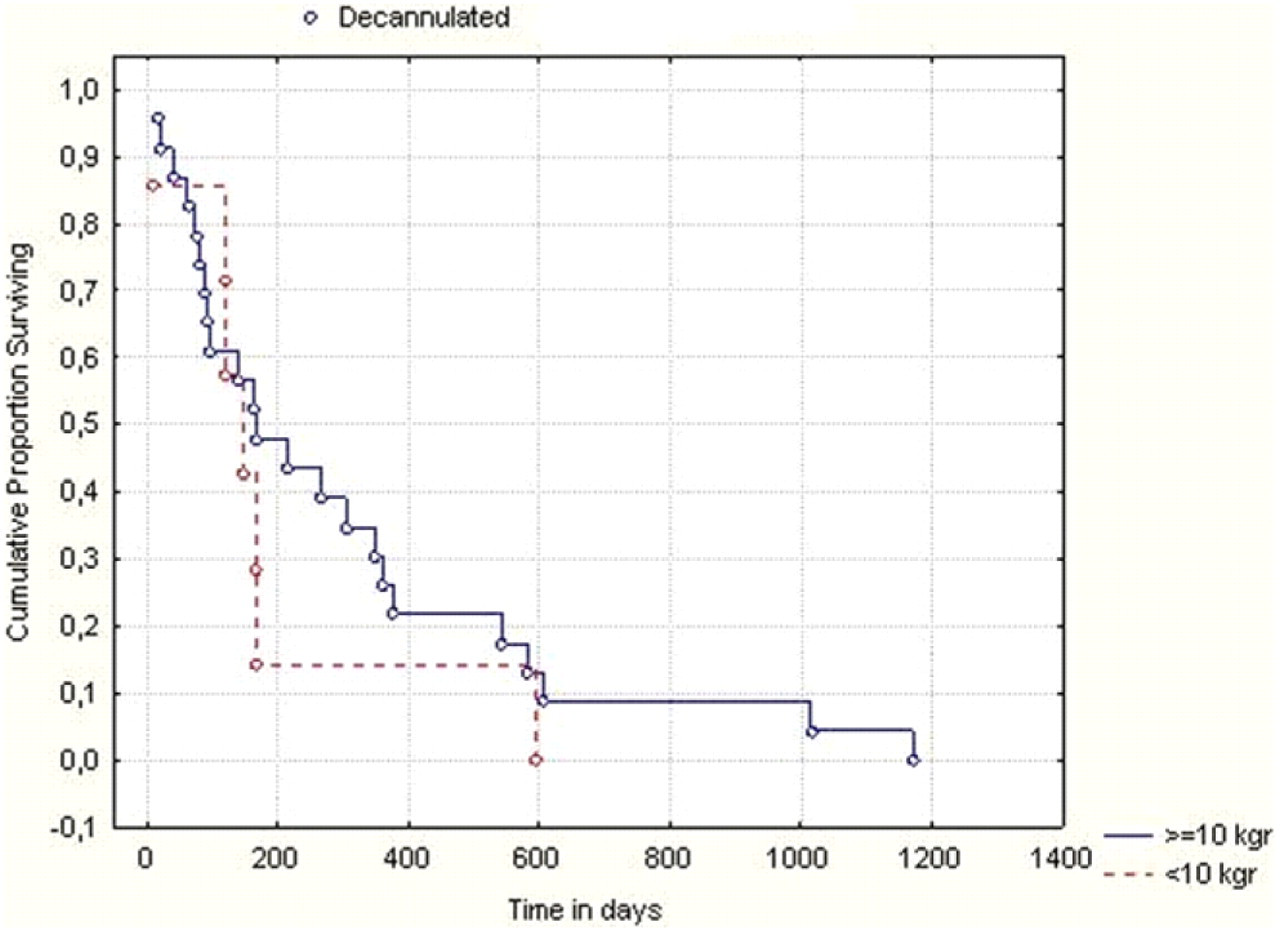
Kaplan-Meier survival curves comparing decannulation time for the double-stage procedures of the two weight groups (P = 0.463).
Finally, there were no significant differences between the two groups (<10 kg and >10 kg) in terms of decannulation rates (P > 0.800) adjusted to the operation stages (single-stage vs double-stage surgery) according to the Cochran's and Mantel Haenszel tests. The estimated odds ratio was 0.406 (95% CI, 0.073–2.265).
Long-term Follow-up
Within the group of 36 infants and children weighing less than 10 kg, 28 of 30 (93%) questionnaires were completed by the patients or their ENT specialists. Two patients were lost to follow-up. Among the six patients who were excluded from the analysis, three died after decannulation from causes unrelated to the surgery, namely their associated congenital anomalies (2 died from major cardiovascular malformations and 1 Catch 22 syndrome patient died from a massive aspiration episode). Two patients died nondecannulated: one from progressive respiratory insufficiency secondary to congenital SED and one from cannula obstruction at home. The patient who is still awaiting decannulation was also excluded from the questionnaire evaluation.
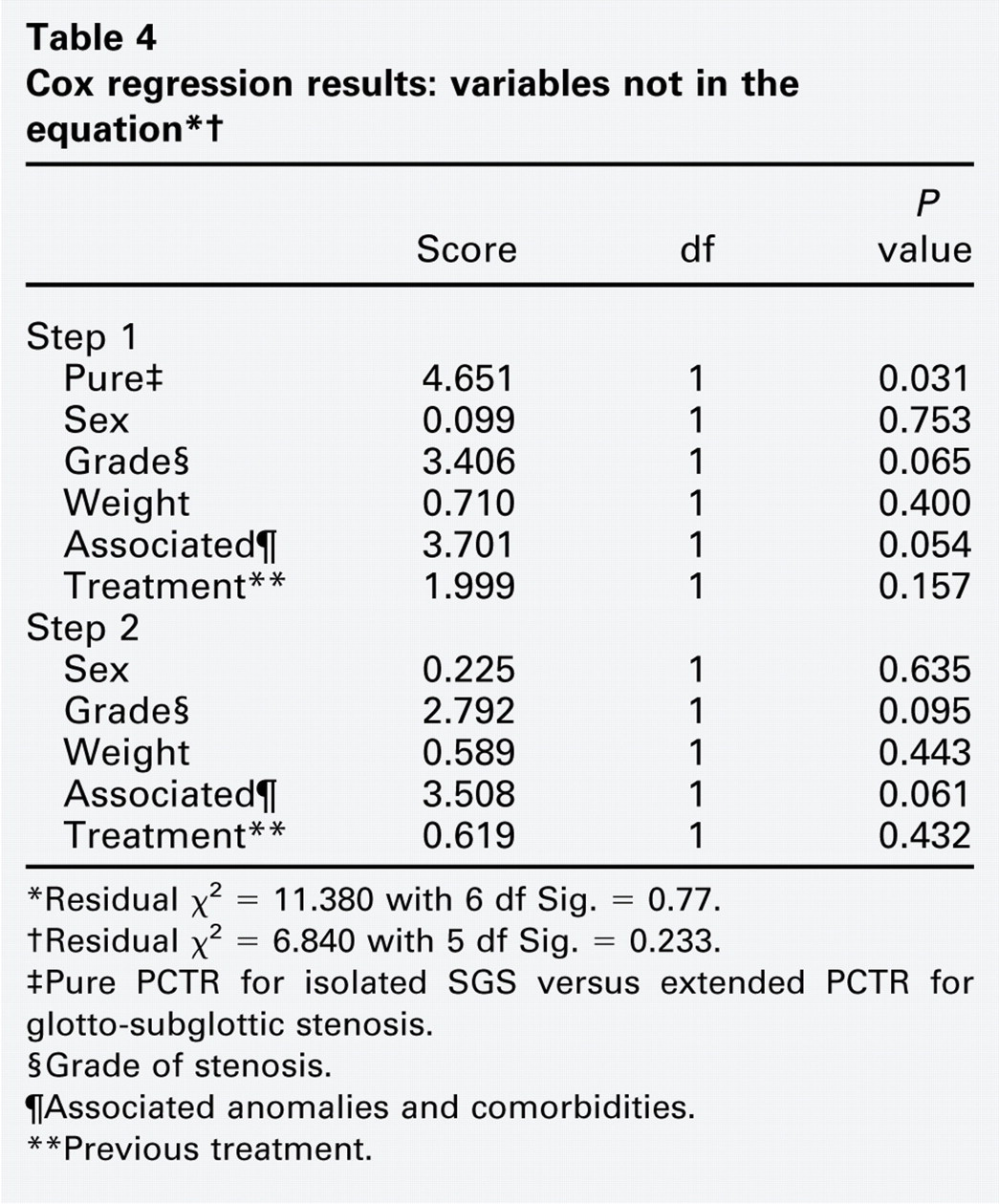
∗Residual χ2 = 11.380 with 6 df Sig. = 0.77.
†Residual χ2 = 6.840 with 5 df Sig. = 0.233.
‡Pure PCTR for isolated SGS versus extended PCTR for glotto-subglottic stenosis.
§Grade of stenosis.
¶Associated anomalies and comorbidities.
∗∗Previous treatment.
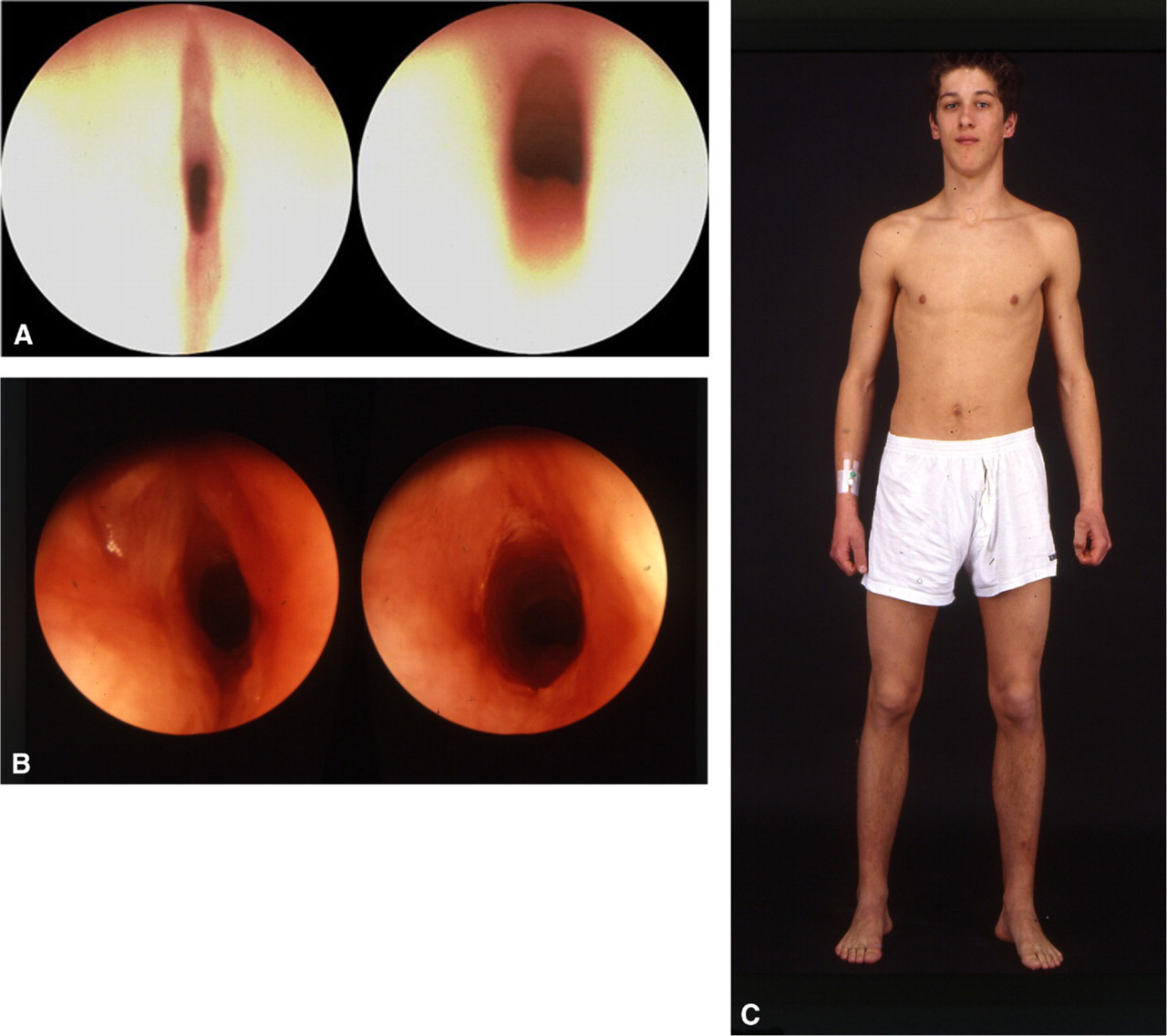
A 2.5-month-old infant weighing 4.4 kg underwent PCTR for congenital grade III SGS (elliptical cricoid). (
In the group of the 28 of 30 (93%) eligible patients who filled in the questionnaire, the median follow-up period was nine years. Two patients have reached adulthood, with a follow-up period of 23 (Fig 2) and 20 years, respectively. Among the other patients, nine had a follow-up ranging between 10 and 15 years, ten between five and 10 years, and seven between one and five years.
The postoperative result was assessed as excellent in 19 out of 28 (68%) evaluations. Six patients (21%) rated the result as good. Three (11%) patients were moderately satisfied because of residual dysphonia.
Breathing was reported as excellent in 27 (72%) patients; namely, no exertional dyspnea even with strenuous physical exercise. Seven (25%) patients still had some breathing difficulties during physical exercise, and only one (3%) patient experienced dyspnea even with slight exertion. No patient had rest dyspnea.
The voice was evaluated as normal in eight (29%) children, as reported by the parents. Fourteen (50%) patients estimated that their voice was rough and that they were facing some difficulties being heard or understood in a loud environment. Five (18%) characterized their voice as weak and whispering, and one (3%) patient assessed the voice as “absent,” which corresponded in fact to a very breathy voice.
In 25 (90%) patients, swallowing was completely normal, with no need for a special diet. Three (10%) patients reported normal swallowing function with some occasional cough due to mild aspiration. No patient was in need of a special diet or feeding tube.
Discussion
The statistical analysis and long-term results of this series of 36 infants and children weighing less than 10 kg at the time of PCTR contribute to the clarification of some concerns regarding the potential risks of this kind of operation on neonates and children of low body weight. Concerns regarding laryngotracheal growth as well as potential arytenoid prolapse after PCTR in this young age group have been reported by others.7,13 The long-term follow-up of this series and endoscopic monitoring did not show any anatomical or functional arytenoid impairments. Moreover, some residual anterior commissure scarring occurring after surgery at this very young age involved a much smaller portion of the vocal cords at a later age. Slight circumferential scarring also grew with the larynx and was almost eliminated after dilatation at three months postoperatively.
Additionally, early successful surgery was highly beneficial to the child's normal development in terms of social impact on the whole family's life. Hopkins et al and Hartnick et al have demonstrated a significant negative impact on the quality of life of tracheostomized children and their parents.14,15 Finally, the financial costs of care giving for tracheostomized children also remains a non-negligible parameter. In a retrospective study using standardized outcome measures, Jiang et al demonstrated that achieving decannulation before the age of 15 months results in a better outcome for speech and language development.16 Furthermore, Simon et al showed that children decannulated during the prelinguistic stage had skills that were commensurate with their intellectual development, while children decannulated during the linguistic stage exhibited specific spoken language delays and phonological impairments.17 Last but not least, early decannulation eliminates the risk of dying from a plugged cannula, which in our series amounted to two percent (2/101) of patients.
The voice outcome in children after PCTR is very difficult to assess in terms of quality. Jaquet et al demonstrated a significant improvement in voice quality after PCTR in a five-year follow-up period of 57 children, but the only comparison was between the postoperative and the preoperative voice, which was either very poor or absent (grades III and IV SGS).3 The subjectivity of parents' estimations of their child's voice as well as difficulties in performing objective assessment in small children result in a lack of data on voice analysis.3,18 The responses on our questionnaire regarding assessment of voice vary when comparing these results to our own clinical and endoscopic findings at the last follow-up. Even though postoperative residual dysphonia evaluation and management remain an unresolved issue requiring further investigation and precise objective evaluation, all published series on pediatric PCTR and LTR have shown that some residual voice problems are without any doubt preferable to a permanent tracheostoma. The high decannulation rate after pediatric PCTR for severe SGS shows that the initial goal is generally achieved.1–8 Improved voice evaluation should represent the next step in the postoperative assessment of PCTR and LTR. However, the high referral rate for patients coming from long distances and the ages of small children almost preclude any prospective voice evaluation because most of these patients will not accept long travel just for an outpatient consultation.
Conclusion
The results of this study have demonstrated that PCTR in infants and children weighing less than 10 kg is a safe and efficient procedure without evidence of any significant difference when compared to results from a group of older children. The experience gained from our series of over 100 PCTRs performed at our institution indicates that a satisfactory result at three months postoperatively is maintained during long-term follow-up. None of the children who were successfully decannulated at three months needed further revision surgery. However, every case should always be independently evaluated by the surgeon, taking into account the patient's individual characteristics before a final therapeutic decision is made.
Cricotracheal resection is a challenging and demanding technique, which can, without any doubt, play a major role in the therapeutic management of pediatric subglottic stenosis, even in infants and children weighing less than 10 kg.
Footnotes
Acknowledgements
We thank all infants and children who underwent PCTR in Lausanne and their parents for kindly replying to the questionnaire.