
Abstract
Anterior skull base defects may give rise to complications that result in significant morbidity and mortality. Pneumocephalus represents a rare, but potentially fatal, sequela of a direct communication between the paranasal sinuses and the intracranial vault. 1 Pneumocephalus is universal after craniotomy; 2 however, persistent, expanding, or spontaneous development of pneumocephalus represents an abnormal physiological mechanism with the potential for significant consequences for the patient.
Management of anteriorly based skull base defects has traditionally involved open approaches with the use of pericranial flaps, and various non-autologous grafts. 3 - 8 During the last three decades, the development of rigid endoscopes and specialized sinonasal instrumentation forced a paradigm shift favoring the use of transnasal endoscopic techniques in the management of select skull base pathologies. Endoscopic approaches have been employed successfully in the management of cerebral spinal fluid (CSF) leaks of the anterior skull base. 8 , 9 Data in the literature are limited, however, on the outcomes of the endoscopic management of skull base defects associated with pneumocephalus. In addition, there is a paucity of information on the role of endoscopic techniques in managing previously failed neurosurgical skull base repair. We present an initial report on the outcomes of the endoscopic management of symptomatic pneumocephalus following previous neurosurgical repair of skull base defects.
Methods
Following institutional review board approval through the Committee for the Protection of Human Subjects Office of Research Support Committees at the University of Texas Health Science Center at Houston, we retrospectively reviewed patients who presented with symptomatic pneumocephalus following neurosurgical intervention and whose skull base defects were subsequently repaired endoscopically between April 1, 2005, and July 1, 2008. Inclusion criteria for the study were 1) radiographic evidence of pneumocephalus associated with anterior or mid skull base defects, 2) neurological symptoms attributed to pneumocephalus; 3) prior open neurosurgical intervention, and 4) subsequent transnasal endoscopic repair of skull base defects.
CT imaging documented the presence and extent of pneumocephalus. Volumetric calculation of the amount of intracranial air was performed by utilizing the area calculation tool (GE Centricity Radiology RA 1000, GE Medical Systems, Milwaukee, WI) multiplied by a standardized slice thickness of 5 mm. The volumes were then summated to calculate the amount of pneumocephalus. This was performed to assess the degree of pneumocephalus at presentation as well as to provide an objective reference for postoperative comparison on serial CT imaging. Three-dimensional (3D) reconstruction demonstrated the extent and configuration of intracranial air. Thin-cut axial CT images (1.25 mm contiguous slices) were obtained for preoperative planning and intraoperative surgical navigation. All patients underwent endonasal endoscopic repair of skull base defects. Successful closure was defined as no recurrence of pneumocephalus or evidence of CSF leak.
Surgical Technique
After induction of general anesthesia, the neurosurgical team placed a lumbar drain through which fluorescein was instilled as previously described. 8 Briefly, 0.1 mL of 10 percent intravenous fluorescein was diluted in 10 mL of autologous CSF and then delivered through the lumbar drain over 30 minutes. An additional aliquot of 5 cc of CSF was used to clear the line to ensure that the entire dosage of fluorescein was delivered.
Appropriate endoscopic dissection of the paranasal sinuses was performed to expose the surgical targets defined during preoperative planning, with careful observation for fluorescein. Standard xenon light illumination without any filters was used. After confirmation of the defect location, a 2- to 3-mm rim of mucosa was elevated from the margins of the defect. When present, encephaloceles were fulgurated with bipolar cautery.
After inspection, small (2-3 mm) or linear defects were closed with a free mucosal graft. If the site was unfavorable for intracranial placement of graft material, such as defects on the lateral lamella of the cribiform plate, or if the dura could not be safely elevated without risk of intracranial injury, only an intranasal mucosal graft was placed, followed by routine packing. Larger defects (> 4-5 mm) were closed with a multilayer technique, 8 in which dura was elevated from the intracranial side of the defect to facilitate intracranial graft placement. Two or more layers of acellular dermal allograft (Alloderm; LifeCell Corp., Branchburg, NJ) with or without a cartilage-free graft were placed to close the defect. A free mucosal graft was then placed over the layered reconstruction. In all instances, fibrin glue sealant was used to hold the mucosal graft in place, and then the reconstruction was supported with a variety of packing materials including absorbable gelatin (Gelfoam; Pfizer, Inc., New York, NY), microfibrillar collagen (Avitene; Alcon Inc., Fort Worth, TX), and gelatin/thrombin matrix (Floseal; Baxter Healthcare, Deerfield, IL) followed by the placement of a small nasal tampon.
Postoperatively, patients were observed in an intensive care unit setting for 24 hours. All patients were placed on postoperative antibiotics with gram-positive coverage and were advised to refrain from nose blowing, bending, lifting, and exertion for six weeks. Postoperative evaluation and follow-up included CT imaging to evaluate the status of pneumocephalus. Follow-up times were based on date of surgery to last clinical evaluation.
Results
Patient demographics, clinical presentation, and prior interventions are summarized in Table 1. Six patients (3 men and 3 women, mean age 54 years, range 32-67 years) met the inclusion criteria. Symptomatology at presentation included headache (2), altered mental status (3), and suspected CSF rhinorrhea (4). Two of four patients with suspected CSF rhinorrhea had a positive beta-2 transferrin test. In addition, one patient was noted to have preoperative meningitis with altered mental status.
Clinical presentation and prior intervention
CSF, cerebral spinal fluid.
Two patients had undergone craniotomy for aneurysm clipping of the proximal internal carotid. Both patients then had sustained defects allowing intracranial communication with the sphenoid sinus attributable to a pneumatized anterior clinoid process. The neurosurgical repair at the initial surgery had involved patching the defect with bone wax and oxidized regenerated cellulose. Additionally, two patients had been treated for anterior skull base tumors (one meningioma and one adenocarcinoma). The patient treated for meningioma suffered an ethmoid roof defect reconstructed with a pericranial flap, fat graft, and a titanium reconstruction plate. The patient with adenocarcinoma developed local recurrence following prior resection with orbital exenteration and radiation. The patient underwent salvage resection and reconstruction of the skull base with a bovine pericardial dural patch, pericranial flap, and temporalis rotational flap. He then developed symptomatic and expanding pneumocephalus postoperatively. The remaining two patients sustained traumatic defects of the skull base. One patient had been involved in a motor vehicle collision in 1986. He had undergone revision craniotomy and repair of his defect with a subsequent shunt revision for the development of pneumocephalus seven weeks prior to our repair. His pneumocephalus subsequently recurred. The other patient had sustained anterior skull base trauma after a fall from a fork lift. Both patients had undergone repairs previously through frontal craniotomies. One patient had received a free bone graft and a pericranial flap, whereas the other had received fascia lata graft with a pericranial flap. Average time from neurosurgical intervention until endoscopic repair was 28 days (range 7-49 days).
Preoperative imaging demonstrated intracranial air in all patients (Fig 1A). The volume of calculated pneumocephalus ranged between 7.2 and 82.8 cc. Preoperative planning with image guidance technology successfully identified all defect sites as confirmed intraoperatively (Fig 2). The extent and configuration of pneumocephalus in relationship to the nasal cavity and paranasal sinuses are demonstrated on a reconstructed 3D model (Fig 3).
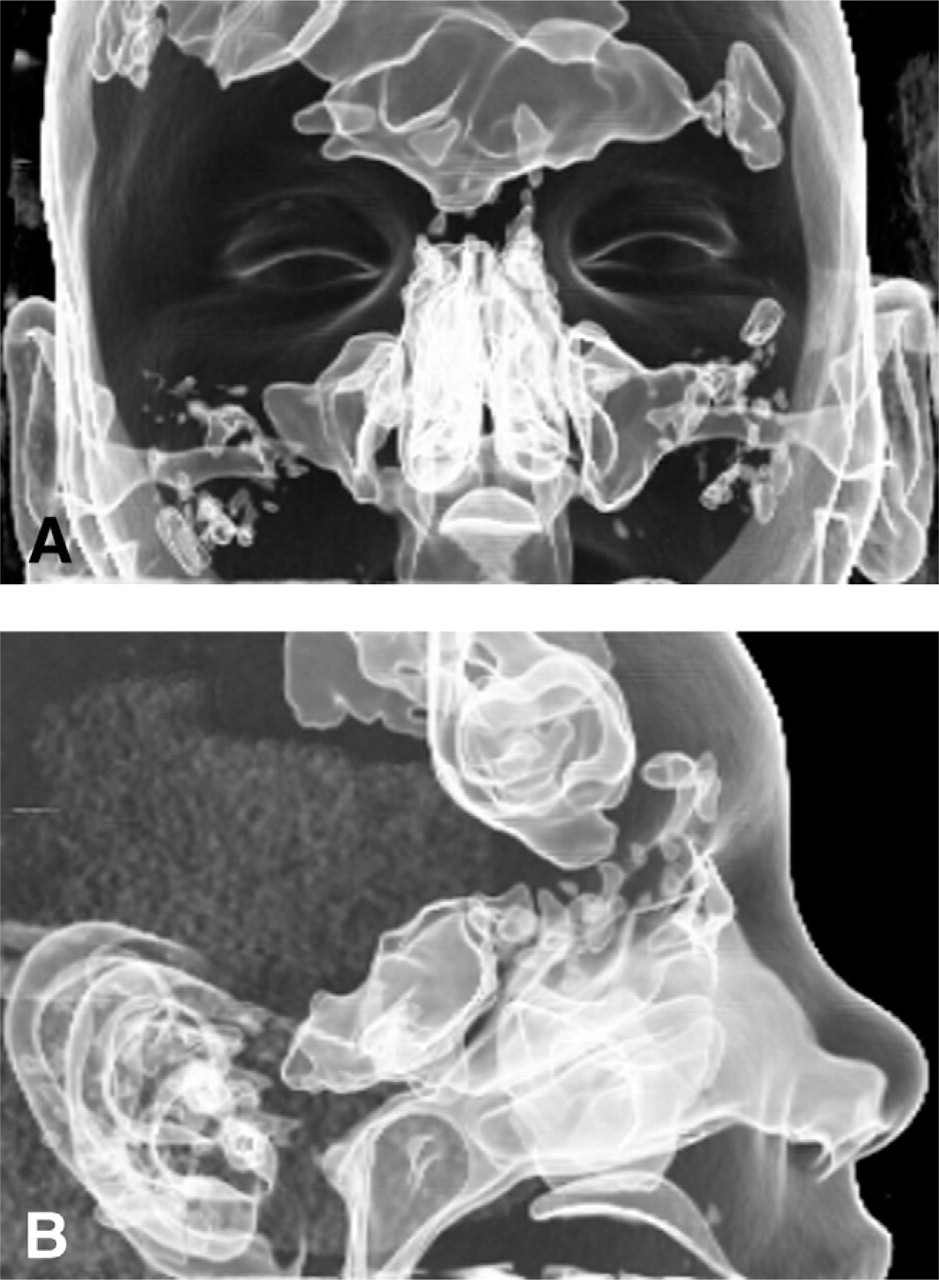
Three-dimensional reconstruction from CT in Figure 1: (
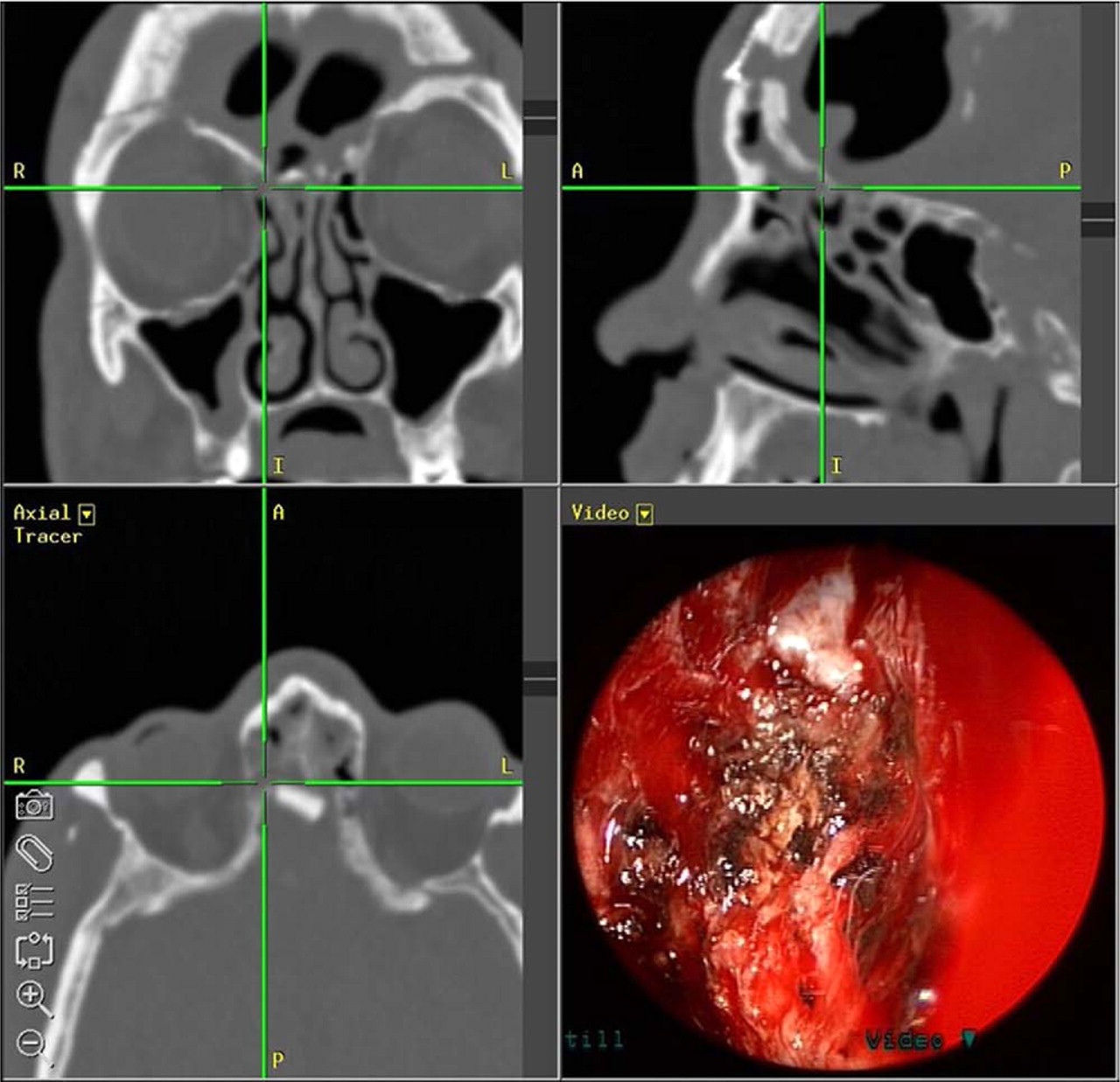
Intraoperative view of a defect in the right ethmoid roof. Note the intracranial bone graft placed during previous open intervention.
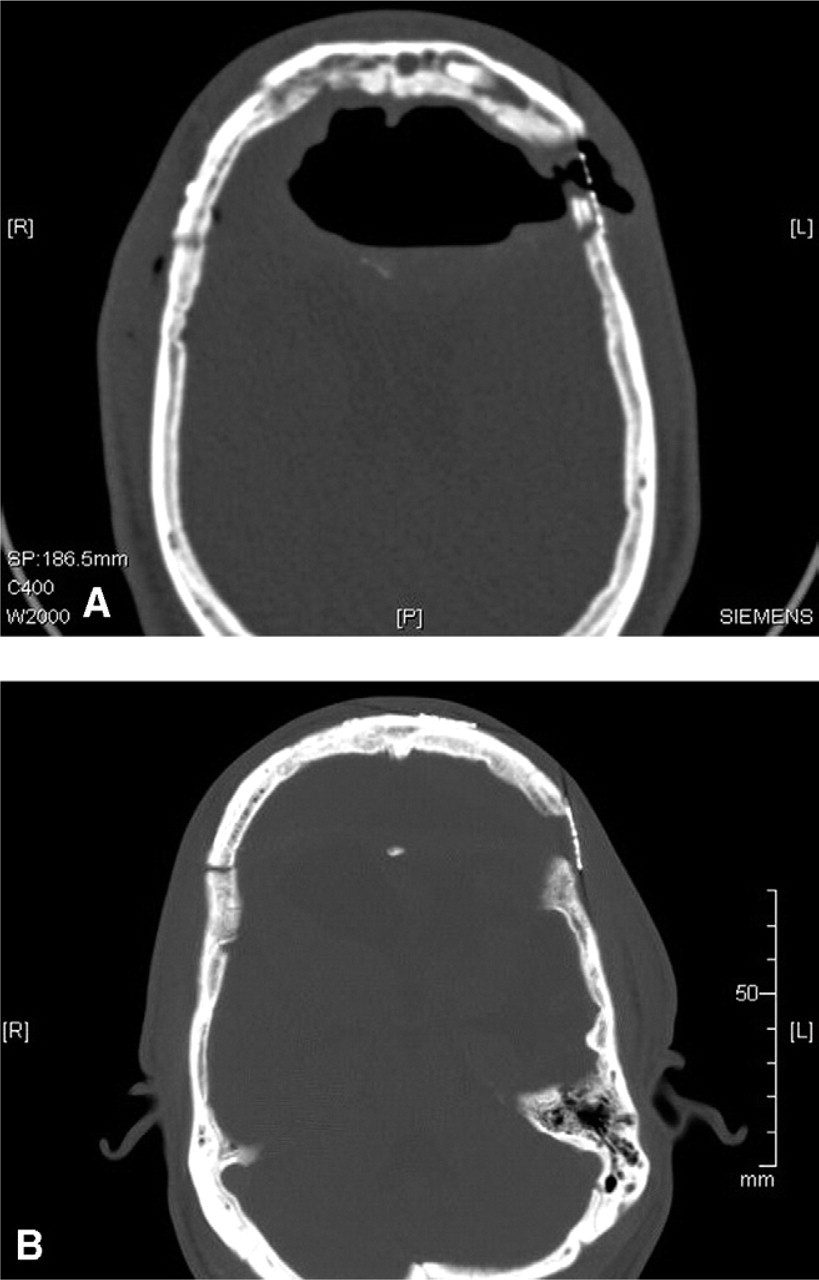
CT brain, axial view: (
In all patients the skull base defects were successfully closed via an endonasal endoscopic approach (Table 2). Layered reconstruction with underlay grafts was performed in two patients. The remaining four patients were treated with a free mucosal graft placement. Two patients were noted to have multiple skull base defects. One of them had three separate defects, two of which received layered reconstruction with underlay grafts, and the third defect received a free mucosal graft. The second patient had two defects, one of which received layered underlay reconstruction, and the other a free mucosal graft. One patient was noted to have an encephalocele that was managed by fulguration with bipolar cautery.
Imaging, operative findings, and surgical outcomes
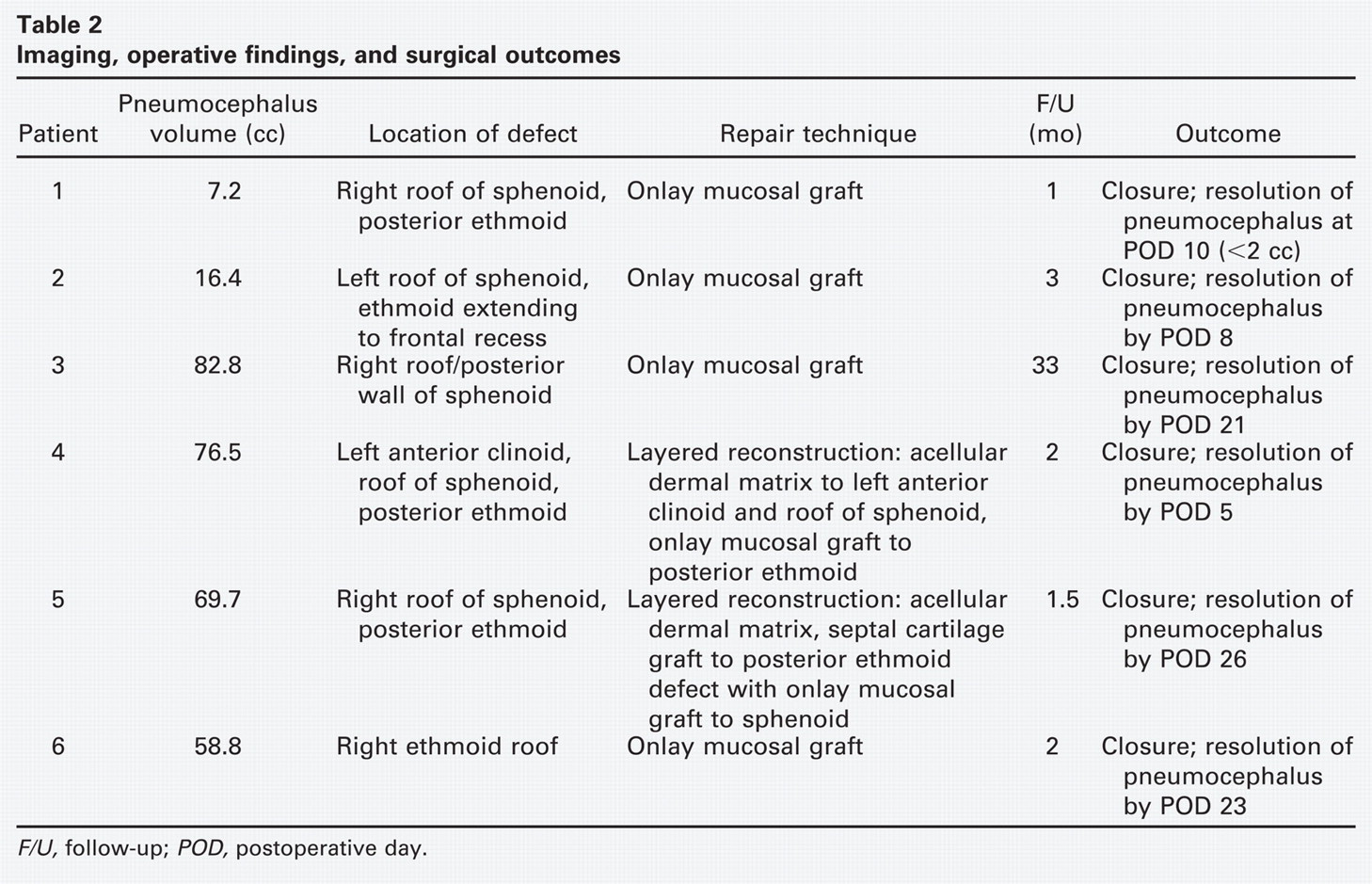
F/U, follow-up; POD, postoperative day.
Closure of defects was achieved in all six patients with complete resolution of the pneumocephalus in five patients after an average of 17 days (Fig 1B); one patient had a trace amount of pneumocephalus (< 2 cc as calculated from CT imaging) at 10 days. Three patients had ventriculoperitoneal shunts (VPS) in this study, all for hydrocephalus. Two patients had them preoperatively. Of these, the first required a revision postoperatively on day three after having had a lumbar drain placed by neurosurgery nine days prior to consulting our service. A second patient had a lumbar drain place intraoperatively for intrathecal fluorescein injection. The third patient had a VPS placed postoperatively for hydrocephalus. None had recurrence of their pneumocephalus (Table 3). In total, lumbar drains were placed in five patients for an average duration of five days (range 1-12 days) with no complications. Intrathecal fluorescein was utilized in each case, but was identified at the site of the defect in only one patient. One other patient did have CSF identified at the skull base defect, but no fluorescein. Opening pressure for this patient was < 5 mm Hg. Opening pressures on the other four patients were not recorded.
CSF shunt and lumbar drain management
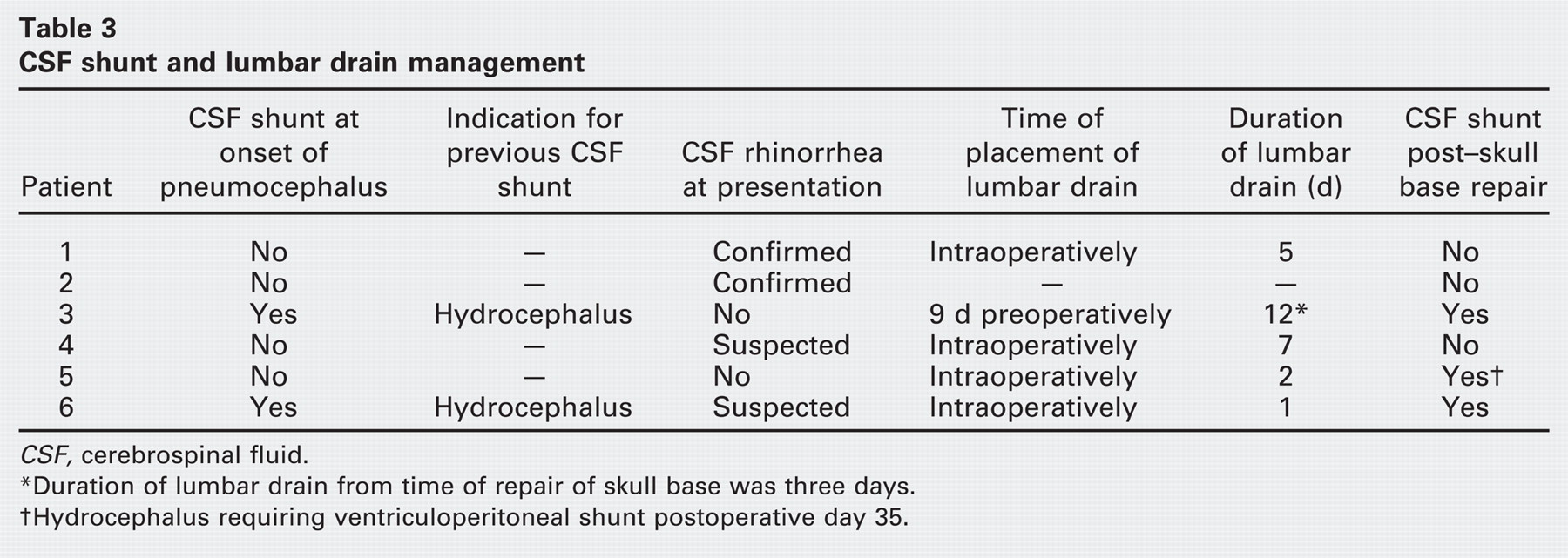
CSF, cerebrospinal fluid.
Duration of lumbar drain from time of repair of skull base was three days.
Hydrocephalus requiring ventriculoperitoneal shunt postoperative day 35.
Mean follow-up was seven months (range 1-33 months). Follow-up was limited in that two deaths occurred. One patient died 1.5 months after surgery from septicemia. Preoperatively, the patient was on multiple antibiotics for resolving nosocomial pneumonia. The source of the septicemia was unavailable. Another patient expired after exsanguination from a massive gastrointestinal bleed one month after closure of her defect. At the time of death, the patient was on a regimen of therapeutic anticoagulation. This patient had resolving pneumocephalus at postoperative day 10, but there was no further imaging prior to time of death to assess resolution. Another patient developed an asymptomatic posterior septal perforation at the donor site of a mucosal graft. The patient had a previous history of radiation to the area. Finally, one patient required a revision endoscopic sinus procedure for CSF rhinorrhea on postoperative day 14 and was found to have an additional sphenoid defect not observed in the first procedure. The patient had no recurrence of pneumocephalus over the interim between procedures. The second defect was repaired with a mucosal graft without recurrence of CSF rhinorrhea. The initial repair was noted to be intact and healing well at the time of the second operation.
Discussion
Several large series report that the incidence of clinically significant pneumocephalus in patients undergoing anterior skull base procedures is 0 to 12 percent. 3 , 6 , 10 - 12 Symptomatology may present acutely and progress rapidly, with a spectrum of findings from headache to mental status changes to frank coma or death. 1 , 12 - 13 Management of acute symptomatic pneumocephalus has classically involved urgent decompression and aspiration of intracranial air and/or placement of a drain with or without airway diversion or nasal packing. This is often followed by surgical re-exploration and repair of the skull base defect. 1 , 11 In our series, two patients had CSF shunts at the onset of pneumocephalus, potentially creating a negative pressure gradient across the skull base favorable to drawing air intracranially. A similar scenario may arise with use of lumbar drains.
There are two scenarios to consider with use of a lumbar drain in the perioperative management of pneumocephalus. The first represents pneumocephalus without a CSF leak. Conceptually, there is no benefit to placing a lumbar drain in this scenario other than providing access for the intrathecal use of fluorescein to aid in defect localization. This was employed in two of our patients. The second scenario represents patients with combined CSF rhinorrhea and pneumocephalus. In this context, the additional benefit of lumbar drain placement in the postoperative period rests on the suspected pressure gradient across the skull base. This is often difficult to evaluate and could potentially require continuous pressure monitoring. In our series, presence of the lumbar drain in the postoperative period did not appear to exacerbate or delay the resolution of intracranial air in patients with combined pneumocephalus and CSF rhinorrhea (Tables 2 and 3). Clearly, close patient surveillance is needed, as well as coordination with neurosurgical colleagues for placement and management of lumbar drains.
Repair techniques have traditionally involved neurosurgical intervention through an external transcranial approach and included the use of fascia and bone grafts as well as pericranial and microvascular free flaps. 5 - 7 , 14 These approaches, however, are associated with significant morbidity and variable success rates. 3 , 4 , 10
Over the last three decades, endoscopic techniques have become the approach of choice for repairing anterior skull base defects associated with CSF fistulas, with high rates of reported closure on first attempt. 9 This approach affords excellent exposure to the skull base and readily available graft donor sites. Data on the endoscopic management of pneumocephalus, however, are lacking and limited to isolated case reports. 15 - 17 There is also a paucity of information in the literature on the usefulness and outcome of the endoscopic management of persistent skull base defects following prior open repair. To our knowledge, this is the first series on the outcomes of the endoscopic management of skull base defects associated with symptomatic pneumocephalus following failed open neurosurgical repair.
In the current series, all six patients, including four who had received pericranial flaps, failed open repair and presented with clinically significant persistent pneumocephalus. An endoscopic technique, similar to what is employed in the repair of CSF fistulas was highly effective and achieved defect closure and resolution of pneumocephalus in five patients and near resolution in one patient at last follow-up. However, technical considerations differ in the repair of CSF leaks versus those associated with pneumocephalus. Absence of CSF extravasations led to higher uncertainty in confirming the location of defects. Therefore, thorough preoperative planning with careful review of the triplanar anatomy and 3D reconstructed models and characterization of surgical targets using computer-aided surgery technology were critical to maximize the diagnostic accuracy and outcome of the intervention. In most patients the skull base was significantly distorted because of the extent of original pathology and/or nature of previous repair. Large deficiencies in the bone of the skull base, as well multiple and bilateral defects through the soft tissues previously used to support intracranial structures, mandated a focused and tailored surgical approach. Postoperative imaging demonstrated quick resolution of pneumocephalus after skull base repair (Fig 3). This is consistent with a study performed by Reasoner et al, 2 which demonstrated resolution of approximately 75 percent of pneumocephalus by the third week following transcranial repair. Additional follow-up is clearly required, and the patients in this study will be closely monitored for surgical failures over the ensuing years.
Fluorescein was not readily visualized in any patient, even when CSF was preoperatively confirmed with beta-2 transferrin. This may be due to a number of factors including unfavorable transcranial pressure gradient, limited dispersion in the subarachnoid space, or insufficient dosage of fluorescein to achieve meaningful intracranial levels. Thus, intrathecal fluorescein may not be useful in this particular clinical setting, making the localization of the defect(s) more challenging, especially in the setting of a previously operated field. Preoperative planning is essential in these cases because the defects may involve contiguous sinuses and/or may be multiple in nature. With the use of CT navigation protocols, special attention is given to defects, allowing continuity of air between the sinonasal cavity and the cranial vault. Intraoperatively, meticulous exposure of these “high-yield” surgical targets is critical to facilitate grafting as well as to indentify defects. Even so, this does not guarantee that all defects will be found, as in the case of the patient who required a second procedure. This defect was identified in the clivus, low on the posterior wall of the sphenoid. Preoperative planning did not reveal an air column across that anatomical area. Also, there was no visible CSF leak from that area during the initial surgical intervention. It is possible that this defect was missed because of its low orientation along the skull base. The remaining defects in this series were all superiorly located in the sphenoid and ethmoid sinuses.
The details of graft placement and selection have generated controversy in the literature. 18 In our series, four patients received a simple mucosal graft placed in an overlay fashion. The remaining two patients had multiple skull base defects, some of which received a simple mucosal graft, whereas others were repaired in a multilayered underlay fashion with acellular dermis with or without cartilage (Table 2). The graft placement technique and material used for grafting, therefore, did not seem to influence the outcome of the procedure. Nonetheless, a layered technique offers the advantage of reconstituting the layers of the skull base and thus may reduce the long-term failure rate. 8 In certain instances, anatomical factors preclude placement of a multilayer reconstruction. These include linear defects (cracks), small defects (< 3-4 mm diameter), and defects in areas where dural elevation is not safe, such as the lateral wall of the sphenoid sinus. Additionally, in a distorted surgical field, bony ledges to support an intracranial cartilage or soft tissue graft may be missing because of large deficiencies in the bone of the skull base that were previously covered with pericranial flap and other soft tissue material. In these instances, a free mucosal graft applied extradurally is appropriate. Most of our patients (5 of 6) had defects involving the sphenoid sinus, with the remaining patient having an ethmoid defect. The general principles of defect repair outlined here may be applied to ethmoid and sphenoid defects, as well as other areas of the skull base.
This series suffers from all of the limitations associated with small retrospective reviews. The number of patients is low, and the follow-up is quite short. In addition, the two mortalities, although they occurred several weeks after surgery, highlight the importance of a multidisciplinary approach to patients with multiple medical comorbidities. Overall, further clinical follow-up is needed to fully elucidate optimal treatment time frames, utility of fluorescein in patients with pneumocephalus, and long-term results.
Conclusion
Endoscopic techniques employed in this preliminary report demonstrate promising results in managing skull base defects associated with clinically significant pneumocephalus following failed prior open neurosurgical repair. The small population size in this study, however, precludes definitive conclusions regarding efficacy.
Author Contributions
Disclosures