
Abstract
Histopathological studies on temporal bone specimens show that cochlear implantation (CI) may damage the peripheral vestibular organ in the inner ear morphologically. 1 , 2 Because of its close topographic vicinity, the sacculus is especially at risk, followed by the utriculus and the semicircular canals. 1 In case of an undesired electrode insertion into the scala vestibuli, Tien et al 2 found an especially high proportion of accompanying vestibular lesions in 75 percent of cases. Besides the direct trauma from insertion caused by the electrode, further mechanisms, such as intraoperative perilymph loss, labyrinthitis, endolymphatic hydrops, or electrical stimulation, can act detrimentally on the peripheral vestibular receptors in the inner ear.
The aim of our study was to examine to what extent these undesired side effects of CI actually influence the function of the peripheral vestibular organ. To address this question, we assessed the function of the semicircular canals and the otolith function. Furthermore, we analyzed whether measurable changes in function correlated with vertigo and imbalance subjectively experienced by the patients.
Materials and Methods
This prospective clinical study was carried out at our CI center at the University of Munich between 2006 and 2009. The study protocol was approved by the local ethics committee of the University of Munich. Informed consent was obtained from all patients included.
Patient Selection
A total of 32 patients with postlingual deafness, aged 15 to 83 years (mean 55 yrs), who underwent unilateral CI for the first time at our institution were included. The patient collective comprised 19 female and 13 male patients. All patients underwent preoperative cranial MRI and high-resolution temporal bone CT, from which a cochlear sclerosis was identified in two patients. One patient had regular findings consistent with a mastoidectomy performed many years earlier on the implant side. The remaining patients had normal anatomy of the middle and inner ear. The indication for CI was based on a severe to profound bilateral deafness, recalcitrant to hearing aid use. The causes of deafness were heterogenous: progressive hereditary-degenerative sensorineural hearing loss (12 patients), acute idiopathic sensorineural hearing loss (7), drug induced/toxic (4), trauma (1), noise (1), and meningitis (1). In six patients, the cause of deafness was not clearly identifiable.
CI
In all patients, the CI was performed by two experienced surgeons (distribution 26:6) using the same standardized technique. Via a retroauricular transmastoidal approach with posterior tympanotomy, a cochleostomy anterior to the round window was performed into the basal cochlear turn. After irrigation of the cochlea with hyaluronic acid, the probe was inserted according to the manufacturer's instructions; then the cochleostomy was sealed with connective tissue. Perioperatively, 500 mg prednisolone and 2 g cefotaxime were administered intravenously. Fifteen patients were implanted on the right side, 17 on the left side. Twenty-six implants of the type Nucleus 24 from the company Cochlear (Sydney, Australia) and six implants (four Pulsars, two Sonatas) from the company MEDEL (Innsbruck, Austria) were used.
Neurotologic Test Battery
The patients were examined directly before and two months after the cochlear implantation in our vestibular laboratory.
Horizontal semicircular canal (hSCC)
For hSCC function test, the vestibule-ocular reflex (VOR) was measured by video-oculography (SensoMotoricInstruments, Teltow-Berlin, Germany). To assess responses to a stimulus presented to each side separately, and to compare the implant side against the nonimplant side, we measured horizontal spontaneous nystagmus (sitting position, 30-degree head anteflexion, eyes open in darkness) and the caloric response to bi-thermal stimulation after Hallpike with 100 mL of 30°C and 44°C warm water over 30 seconds, respectively. Spontaneous nystagmus was recorded for 60 seconds and was rated as positive if the maximal slow phase velocity (SPV) was greater than one degree per second. During caloric testing, patients were supine with 30-degree elevation of the upper body (resulting in vertical position of horizontal canals). Nystagmus was recorded over 80 seconds. From a 20-second interval, the mean maximal SPV was determined, and the caloric VOR was evaluated according to Jongkees' formula.
Sacculus
The sacculus function was tested by vestibular-evoked myogenic potentials (VEMP), according to the method described by Basta et al. 3 The stimulus was a 500-Hz tone burst (105 dB SPL, 7 ms duration, 5 per second) applied via air conduction. The electromyographic response of the ipsilateral sternocleidomastoid muscle was recorded by means of surface electrodes (impedance < 3 kμ). The active electrode was placed at the half-way point of the muscle, with the reference electrode on the sternum. The ground electrode was placed on the forehead. The patient was seated with his or her head turned 45 degrees, which created a steady tonic activity in the sternocleidomastoid muscle (according to 50-200 μV in the EMG). At least 130 measurements were averaged (gain 5000×; filter 20-1500 Hz). The amplitude was determined as the average of two measurements of the difference between the first positive peak and the first negative peak (P1-N1, in μV).
Vertigo Symptoms
The subjective vertigo complaints of the patients after CI surgery were assessed by means of a questionnaire. This questionnaire was developed at our institution specifically for the documentation of vertigo and imbalance symptoms in patients undergoing CI, and has been described in detail elsewhere. 4
Data Analysis
The pre- and postoperative results of the VOG and VEMP examinations in the implanted patients were compared. Implant and nonimplant ears were both assessed. The caloric responses were classified as normal, canal paresis (SPV ≤ 10 degrees per second after warm and cold irrigation), and caloric loss. An absolute value of VEMP amplitude ratio of < 0.5 was considered a decreased VEMP after CI.
The group of patients with postoperative vertigo symptoms was compared with the asymptomatic group with regard to the findings on caloric testing of the hSCC and VEMP responses of the sacculus.
For statistic analysis, the t test or Mann-Whitney test was used (P < 0.05) (SPSS version 15.0; SPSS Inc., Chicago, IL).
Results
The VOG could be performed in all 32 patients pre- and postoperatively. However, one patient did not tolerate the bi-thermal stimulation postoperatively. In another patient, a congenital pendular nystagmus prevented a useful analysis. Therefore, the complete VOG examinations could be analyzed in 30 of the 32 patients. The VEMP examinations were performed in 30 of 32 patients preoperatively and in all patients postoperatively.
Preoperative Peripheral Vestibular Function
hSCC
Thirteen (41%) patients had a normal VOG examination result on both sides, without spontaneous nystagmus and with approximately symmetric (side difference < 20%) caloric response of the hSCC. In the majority (59%) of the patients, however, abnormal findings were present even preoperatively. Five patients had a horizontal spontaneous nystagmus, with a side difference of > 20 percent of the VOR. The VOR of the implant side was normal in 16 (52%) patients, reduced in five (16%) patients, and lost in 10 (32%) patients. Five patients had bilateral loss.
Sacculus
The VEMP examination yielded normal responses in 14 of 30 (47%) patients on the implant side. In 11 of these patients, the sacculus response was also present on the contralateral side. Twelve (40%) patients had a preoperative loss of sacculus function bilaterally.
Correlation of VOR and VEMP Results
About one third of the patients (9 of 30) showed a normal test result in VOG and VEMP—that is, a regular function of the hSCC and the sacculus. In about a quarter of the patients (7 of 30), both VOR and VEMP were lost.
Postoperative Peripheral Vestibular Function
hSCC
After the CI surgery, eight (27%) patients still had normal hSCC function. In a further eight patients, the VOR function deteriorated (from normal to canal paresis, n = 6; from normal to caloric loss, n = 2). After exclusion of the 10 patients with preoperative loss of hSCC function, this results in a risk of functional impairment for the hSCC after CI of 50 percent. In the patients with preexisting canal paresis or caloric loss, there was no measurable change in function postoperatively.
In the 16 patients with preoperative regular hSCC function, a significant decrease of SPV was noted on the implant side in the caloric testing (P < 0.001; t test). The SPV fell from 39.2 degrees per second (SD = 17.7) to 23.9 degrees per second (SD = 15.4) postoperatively.
Sacculus
CI led to a loss of sacculus function on the implant side in six patients. In the remaining eight patients, the VEMP on the implant side was still detectable postoperatively, albeit reduced in amplitude by more than 50 percent in six cases. Therefore, the risk of functional damage to the sacculus on the implant side was 86 percent. In one case, the potential was unchanged, and in another case, the amplitude was increased. In all patients with preoperative absent VEMP, this was unchanged after the CI surgery.
Upon analysis of the VEMP amplitude values of the 14 patients with preoperatively regular sacculus function, there was a significant deterioration (P = 0.047; t test), from 19.3 µV (SD = 20.8) preoperatively to 6.9 µV (SD = 11.7) postoperatively.
Correlation of VOR and VEMP Results
Of the nine patients with preoperatively regular hSCC and sacculus function, only one patient (male, 69 yrs) still had normal findings postoperatively. In all of the other eight patients, there was a deterioration of function in the peripheral vestibular receptors. In four patients, both hSCC function and sacculus function were diminished. In three cases, the VOR was unchanged but the VEMP was reduced or lost. In one case, the VOR was reduced but the VEMP amplitude increased. A complete caloric loss did not occur in any of these patients. These findings are summarized in Table 1.
Test findings of horizontal canal function (VOR) and sacculus function (VEMP) of the implanted ear before and after cochlear implant surgery as well as incidence of postoperative vertigo symptoms of the nine patients with preexisting regular peripheral vestibular receptor function
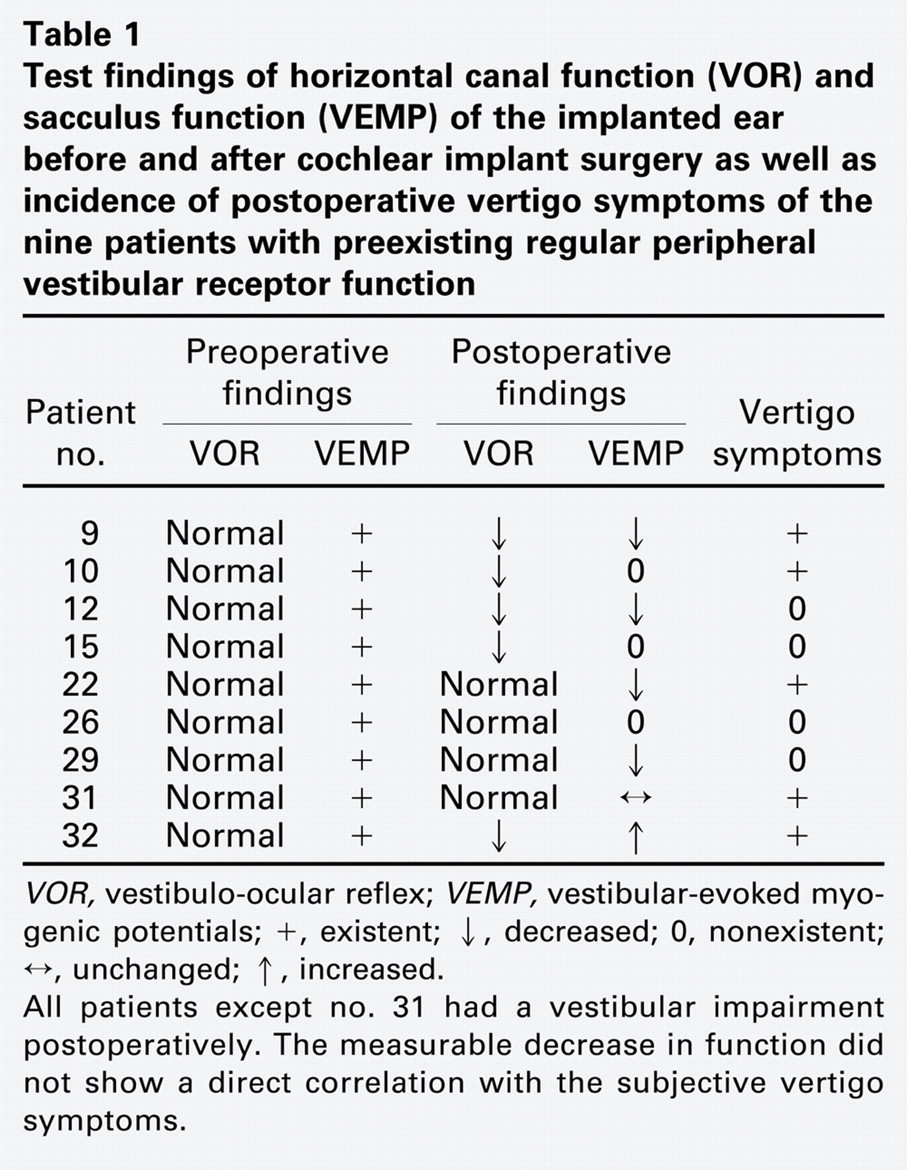
VOR, vestibulo-ocular reflex; VEMP, vestibular-evoked myogenic potentials; +, existent; ↓, decreased; 0, nonexistent; ↔, unchanged; ↑, increased.
All patients except no. 31 had a vestibular impairment postoperatively. The measurable decrease in function did not show a direct correlation with the subjective vertigo symptoms.
Peripheral Vestibular Function on the Nonimplant Side
On the nonimplant side, as expected, there was no significant change of vestibular function (P > 0.05; t test). The mean SPV was 26.4 degrees per second preoperatively (SD = 22.1) versus 25.2 degrees per second postoperatively (SD = 22.3); the mean VEMP amplitude was 15.0 µV (SD = 20.0) before CI versus 14.1 µV (SD = 12.3) after CI.
Subjective Vertigo Symptoms
Thirteen (41%) of the 32 patients reported vertigo or balance problems after CI. With the exception of one case, the vertigo appeared within the first four weeks—that is, before activation of the CI device. Patients commonly complained of motion-induced rotatory or to-and-fro vertigo, which, in most cases, resolved within one week. In six patients, the vertigo symptoms persisted. Two of them showed a loss of sacculus function and canal paresis.
The results of the vestibular function tests did not correlate with the subjective complaints. The incidence of postoperatively worsened test results in VOR and VEMP examinations among the patients with postoperative vertigo was not significantly different from the incidence of worsened results among the asymptomatic patients (P > 0.05). For example, the only patient with completely normal vestibular test results before and after the CI surgery was still experiencing short attacks of to-and-fro vertigo, which first appeared on the first postoperative day. His vertigo was accompanied by tinnitus and nausea, and resolved within four weeks under homeopathic medication.
Discussion
Our results show clearly that CI can damage the function of peripheral vestibular receptors in the inner ear. In the case of preoperatively normal findings, the risk of impairment of hSCC and of the sacculus is 50 percent and 86 percent, respectively. The function of the nonimplant side is preserved. The higher incidence of saccular dysfunction is consistent with the above-mentioned temporal bone studies, in which the sacculus also was the most frequently damaged organ. 1
Other groups have reported similar results. Buchman et al 5 analyzed 22 publications on vestibular function before and after CI between 1995 and 2004 and found an average change in VOR after CI in 71 of 186 (38%) patients. The reported rates vary from 23 to 100 percent, in a wide spectrum. More recent reports show a comparatively higher risk of vestibular function damage. This is probably due to the better (prospective) study design and more sensitive examination methods using VOG and computerized analysis. Only a few of the more recent studies also analyzed the otolith function before and after CI. This resulted in an impaired sacculus function in 21 percent 6 to 100 percent. 7 Table 2 provides an overview of the published reports on this subject, enabling a comparison with our own data. In summary, it can be stated that CI represents a relevant risk of functional damage to the hSCC and the sacculus. In light of the ever growing spectrum of indications for CI (patients with partially preserved hearing, unilateral deafness, severe persistent tinnitus), the widespread use of CI in infants and young children, and the increasing number of bilateral implantations, the potential damage to the peripheral vestibular receptor function is of great importance. For example, a bilateral CI could lead to an iatrogenic bilateral vestibulopathy with a persistent balance dysfunction. In the case of CI in infants, an impairment of motor development is conceivable. On this subject, there is still a lack of conclusive clinical studies. In any case, the trauma to the inner ear during an implantation should be kept to a minimum. It is already possible, by means of technological advances and new soft-surgery techniques, to minimize cochlear damage and conserve preexisting residual hearing function. As Todt et al 6 have shown, the surgical technique also influences the rate of vestibular side effects. The comparison of two different surgical approaches showed that, in patients with round window insertion, a deterioration of otolith function (13% vs 50%), hSCC function (9% vs 43%), and vertigo symptom scores (13% vs 23%) occurred significantly less frequently than in patients with anterior cochleostomy.
Overview of clinical studies on the function of peripheral vestibular receptors of the implant ear before and after cochlear implantation
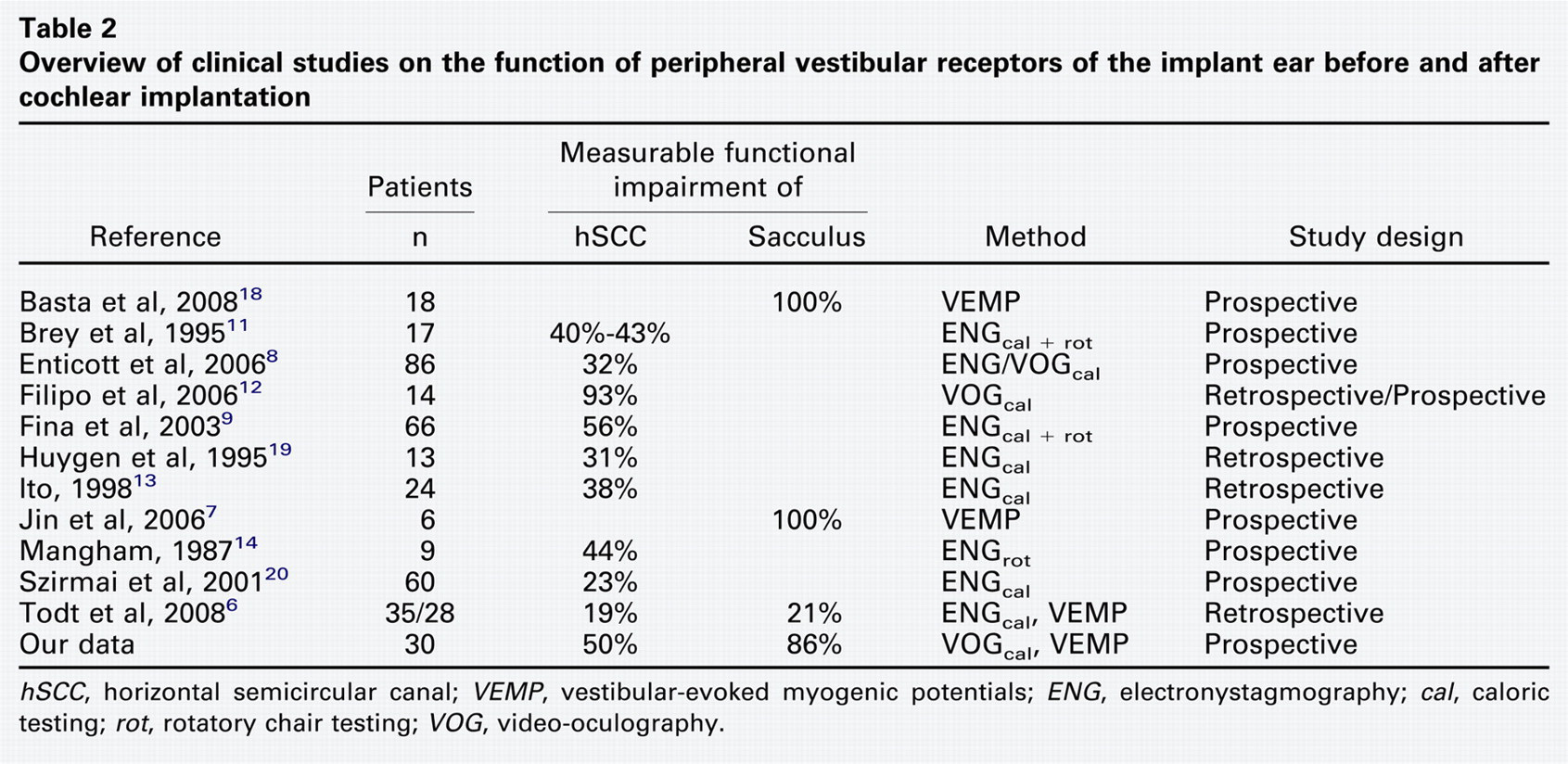
hSCC, horizontal semicircular canal; VEMP, vestibular-evoked myogenic potentials; ENG, electronystagmography; cal, caloric testing; rot, rotatory chair testing; VOG, video-oculography.
The cause of deafness was manifold in our patient collective, corresponding to the usual spectrum of CI candidates, which is comparable to the spectrum noted in other reports. 5 , 8 , 9 In the majority of patients, the inner ear disease, irrespective of its etiology, also leads to a vestibular impairment. Even before CI surgery, 70 percent of our patients showed abnormal VOR and/or VEMP test results. In about one quarter (23%) of the patients, both functions were lost. Many of these patients already had vertigo and balance disturbances before the implantation, as previously reported. 10 Of the 47 surveyed adult patients, 53 percent reported symptoms even before the CI. In 84 percent of these cases, the history suggests an otogenic origin of the vertigo symptoms.
In patients with vertigo or imbalance after CI, there is no difference in asymptomatic patients with respect to neurotologic function tests pre- and postoperatively. This is in accordance with previous reports. 5 , 8 , 9 , 11 - 16 Factors like gender, implant type, implant side, surgeon, cause of deafness, petrous bone CT findings, and preexisting preoperative vertigo did not influence the occurrence of balance problems. 4 However, advanced age constituted a risk factor in some studies. 4 , 8 , 11 Central vestibular compensatory mechanisms may suppress peripheral vestibular dysfunctions. In CI patients with conserved ability of visual fixation suppression, vertigo symptoms were found significantly less often. 17 The poor correlation between the patients' subjective complaints and the objectively measurable changes in neurotologic tests may be explained by the wide array of possible causes of balance disorders after CI. Benign paroxysmal positioning vertigo, Tullio phenomenon, electric stimulation, or psychosomatic causes cannot be quantified by caloric testing, rotatory chair testing, or VEMP testing. 4 Therefore, when the history is suggestive, further testing should be initiated.
Limitations of the present study are the lack of examination of the utriculus function (e.g., by excentric rotatory chair testing), and the relatively short follow-up period of two months. Further studies are necessary to gather information on the long-term clinical course of those patients who experienced postoperative vertigo.
In conclusion, the following points can be deduced from our study. CI harbors a relevant risk of functional damage to the vestibular receptors of the implanted ear. The patient must be made aware of this possibility. One goal of the operation should be the sparing of cochlear and vestibular structures, by means of minimal trauma to the inner ear. When incapacitating or persisting vertigo symptoms occur in CI patients, a focused history, diagnosis, and therapy are necessary because the etiology of the balance disturbance can be manifold.
Author Contributions
Disclosures