
Abstract
In this evidence-based case report we studied the clinical question: Does intranasal corticosteroid (INCS) monotherapy reduce time to recovery in adults with acute noncomplicated rhinosinusitis? The search yielded 490 papers, of which only two were relevant and had a high validity regarding our clinical question.
Williamson et al, 1 who used a factorial-designed randomized controlled trial, showed no difference in either the proportion of clinically cured patients at day 10 (aRD: 0% [95% CI: –12.6% to 12.7%]) or the total symptom score at day 10. Another large randomized controlled trial, performed by Meltzer et al, 2 reported a statistically significant difference in mean major symptom scores (MSS) over the 15-day treatment period within both intranasal corticosteroid (INCS) groups (once and twice daily) as compared to the placebo group. However, the clinical relevance of mean MSS as primary endpoint is debatable and the size of the reported effect in this study is modest. In conclusion, current evidence shows that the clinical beneficial effect of INCS monotherapy compared to placebo has not been established in patients with acute rhinosinusitis.
Clinical Case
A 33-year-old female patient visits your practice. She is complaining of fatigue, nasal discharge and obstruction, hyposmia, and facial (maxillary) pain. These symptoms started some 10 days ago and during the first days she had mild fever. Unable to work, she is now wondering whether she could benefit from INCS because she read on the Internet that INCS are beneficial in acute rhinosinusitis. Since you are not sure about the evidence of prescribing these agents, you decide to evaluate the existing literature.
Background
Acute rhinosinusitis is a common reason to consult a doctor and is accompanied with high direct and indirect health care costs. 3 - 5 Although acute rhinosinusitis is self-limiting in the majority of adults within two to four weeks, its unpleasant symptoms can considerably impair daily functioning and do have a negative influence on quality of life. 6 As most episodes of acute rhinosinusitis are caused by viruses, the vast majority of patients do not benefit from antibiotics. 7 Despite overwhelming evidence, physicians continue to prescribe oral antibiotics very frequently, 3 , 4 , 8 which may lead to unnecessary side effects and enhancement of antimicrobial resistance. 9 - 11 In order to accelerate recovery and reduce antimicrobial resistance, treatment targets for acute rhinosinusitis should shift away from antibiotics.
Currently, it is thought that nasal mucosal inflammation is a more important target for treatment than possible microbiological pathogens. 12 - 14 Consequently, anti-inflammatory drugs could be effective by reducing the inflammatory response and enhancing clearance of the sinuses. INCS have proved to be effective in controlling seasonal and perennial allergic rhinitis symptoms by reducing sinonasal mucosal inflammation 15 , 16 and are well tolerated and safe. 17 , 18 INCS monotherapy might therefore be a potential treatment option for reducing time to recovery from acute rhinosinusitis.
Clinical Question
Does treatment with INCS alone reduce time to recovery in adults with acute noncomplicated rhinosinusitis?
Searching for Evidence
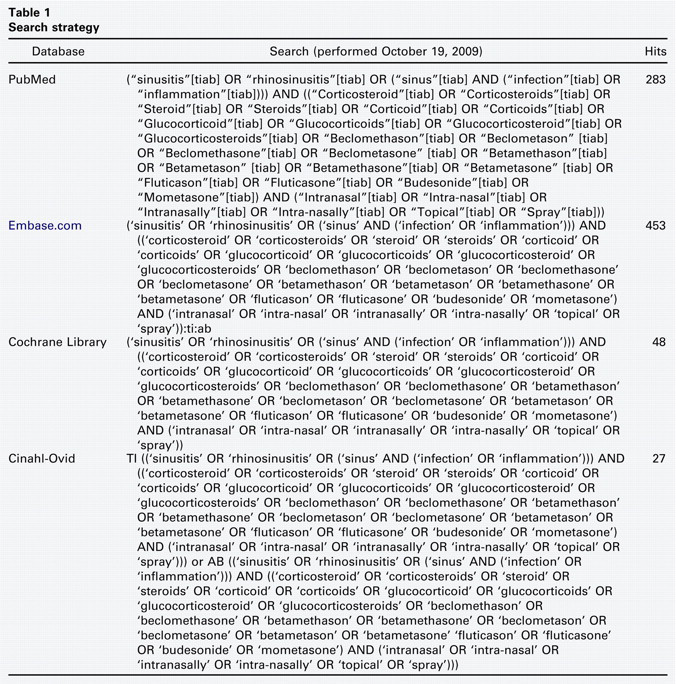
We designed a search filter using relevant synonyms for the domain, being adults with acute rhinosinusitis, and the determinant, which is INCS treatment. Acute rhinosinusitis was defined as inflammation of the nasal mucosa and the paranasal sinuses characterized by both nasal (e.g., obstruction, discharge) and sinus (facial pain/pressure, tooth pain) complaints lasting for a maximum of 12 weeks. 19 We retrieved relevant publications in PubMed, Embase.com, Cochrane Library, and Cinahl-Ovid using search terms in title and abstract fields. Our search yielded 283 records in PubMed, 453 articles in Embase.com, 48 in Cochrane Library, and 27 in Cinahl-Ovid (Table 1). Title and abstract of all retrieved records were screened using the following inclusion criteria: “adult patients (aged ≥ 18 years) with acute rhinosinusitis,” “INCS monotherapy,” and “therapeutic study.” The exclusion criteria are shown in the flowchart (Fig 1). Upon screening, four publications remained for further analysis.
Search strategy
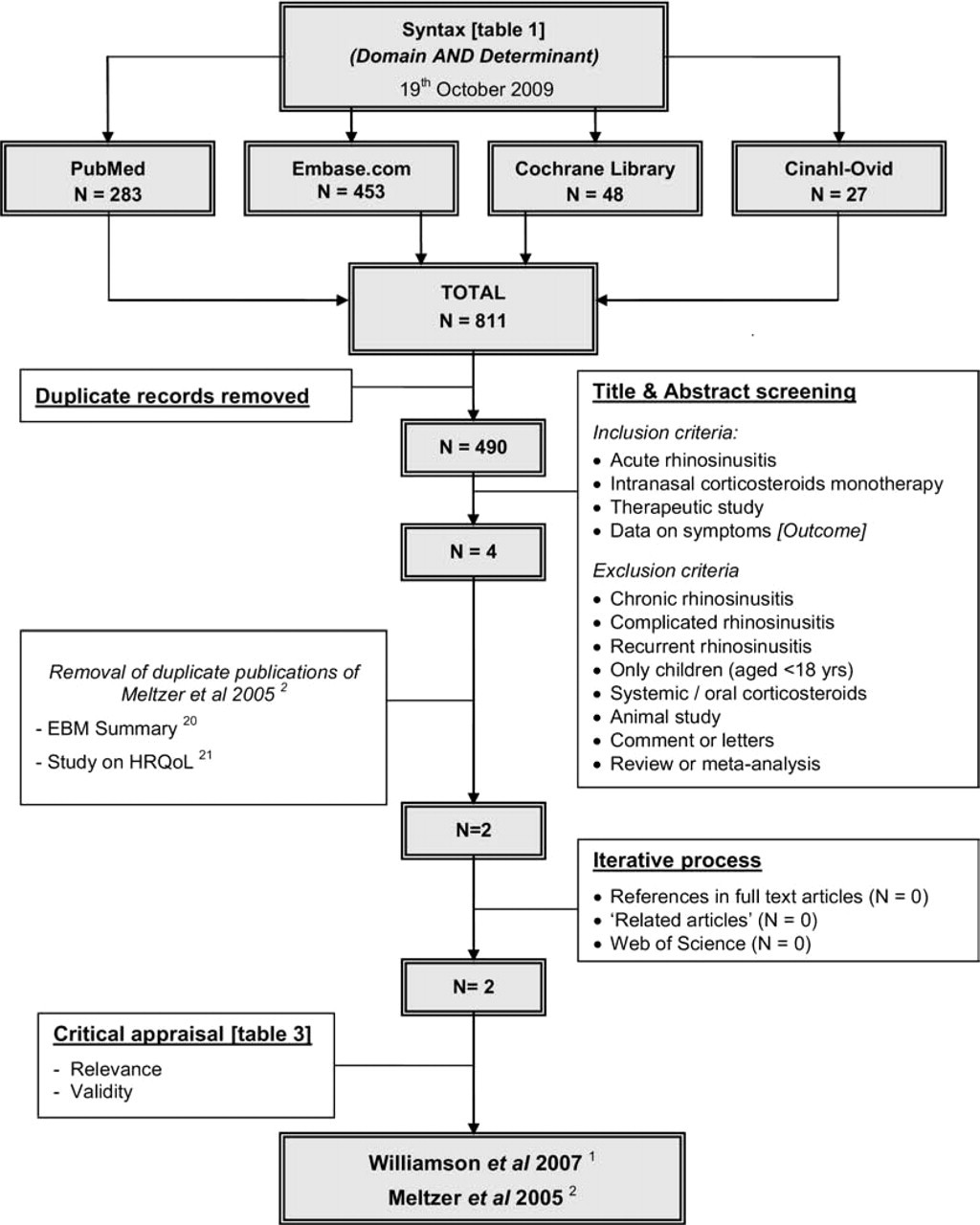
Literature search and exclusion criteria.
The full text of the four selected publications was studied in more detail for their relevance in terms of our domain, determinant, and outcome. As a result, two publications were excluded (Fig 1). These studies appeared to be duplicate publications of the main study by Meltzer et al, 2 i.e., one 20 was an EBM summary and the other 21 reported the effects on health-related quality of life (HRQoL).
The quality of methods and reporting of results of the remaining two articles were critically appraised, using the criteria shown in Table 2. The publications of Williamson et al 1 and Meltzer et al 2 were of adequate quality. Williamson et al 1 provided numerical data on symptom resolution over time that allowed us to calculate the absolute risk difference (aRD) and corresponding confidence interval. Unfortunately, Meltzer et al 2 provided neither numerical data on symptom resolution over time nor standard deviations. Therefore, confidence intervals for the mean differences in their major symptom scores (MSS) could not be calculated.
Critical appraisal of relevant studies
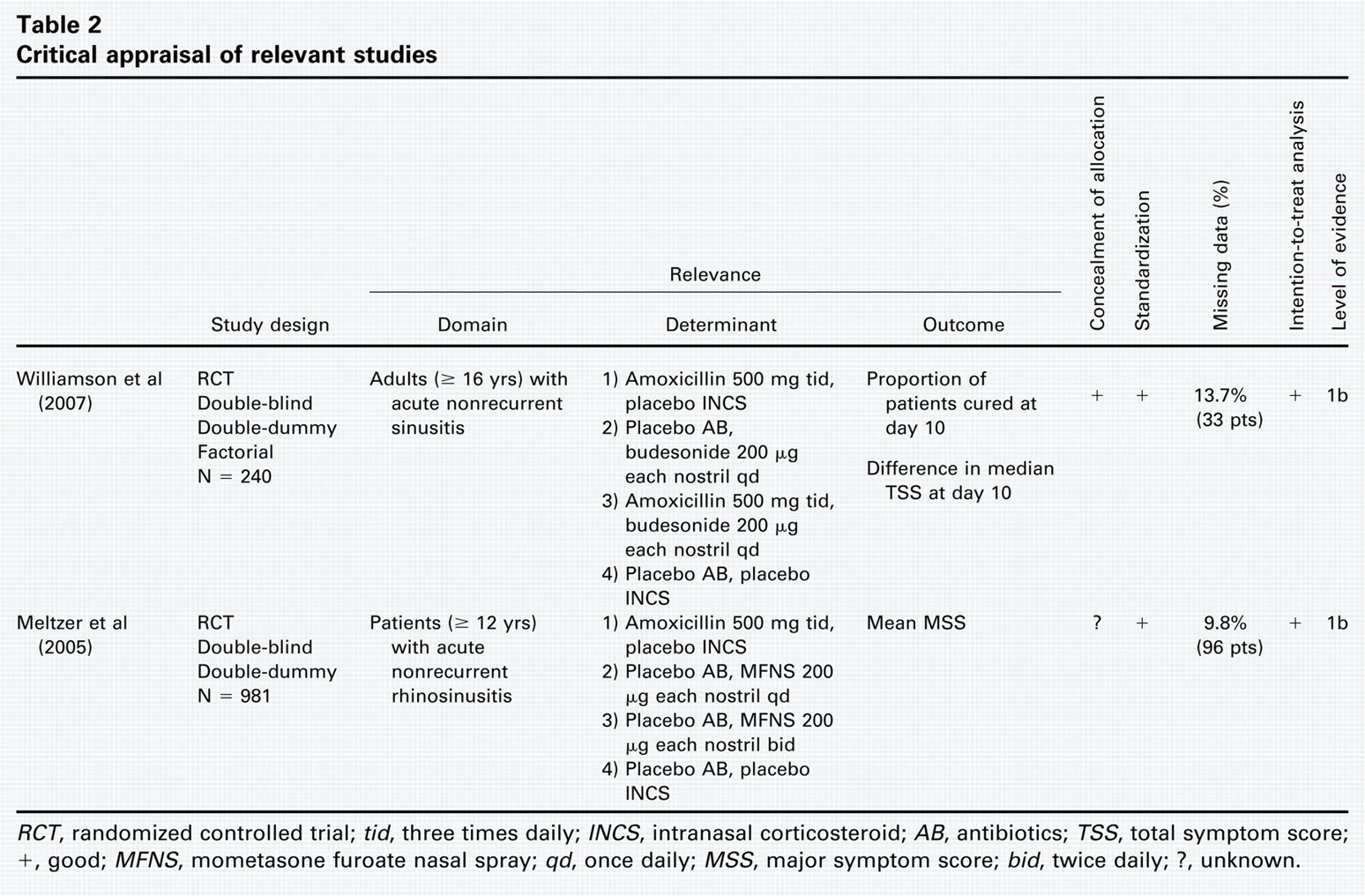
RCT, randomized controlled trial; tid, three times daily; INCS, intranasal corticosteroid; AB, antibiotics; TSS, total symptom score; +, good; MFNS, mometasone furoate nasal spray; qd, once daily; MSS, major symptom score; bid, twice daily; ?, unknown.
Results
Williamson et al 1 performed a double-blind, double-dummy, randomized, placebo-controlled factorial trial to assess the effectiveness of amoxicillin and budesonide (200 μg once daily) in 240 patients aged 16 years or older with acute maxillary sinusitis. Acute maxillary sinusitis was defined as nonrecurrent illness (< 28 days) meeting a minimum of two of the criteria defined by Berg and Carenfelt. 22 They showed that the proportion of patients with resolution of symptoms at day 10 did not differ between budesonide and no budesonide (both 68.6%, aRD: 0% [95% CI: –12.6% to 12.7%]) (Table 3). Besides, there was no difference in median total symptom score (TSS) at day 10 between both groups.
Results of relevant studies
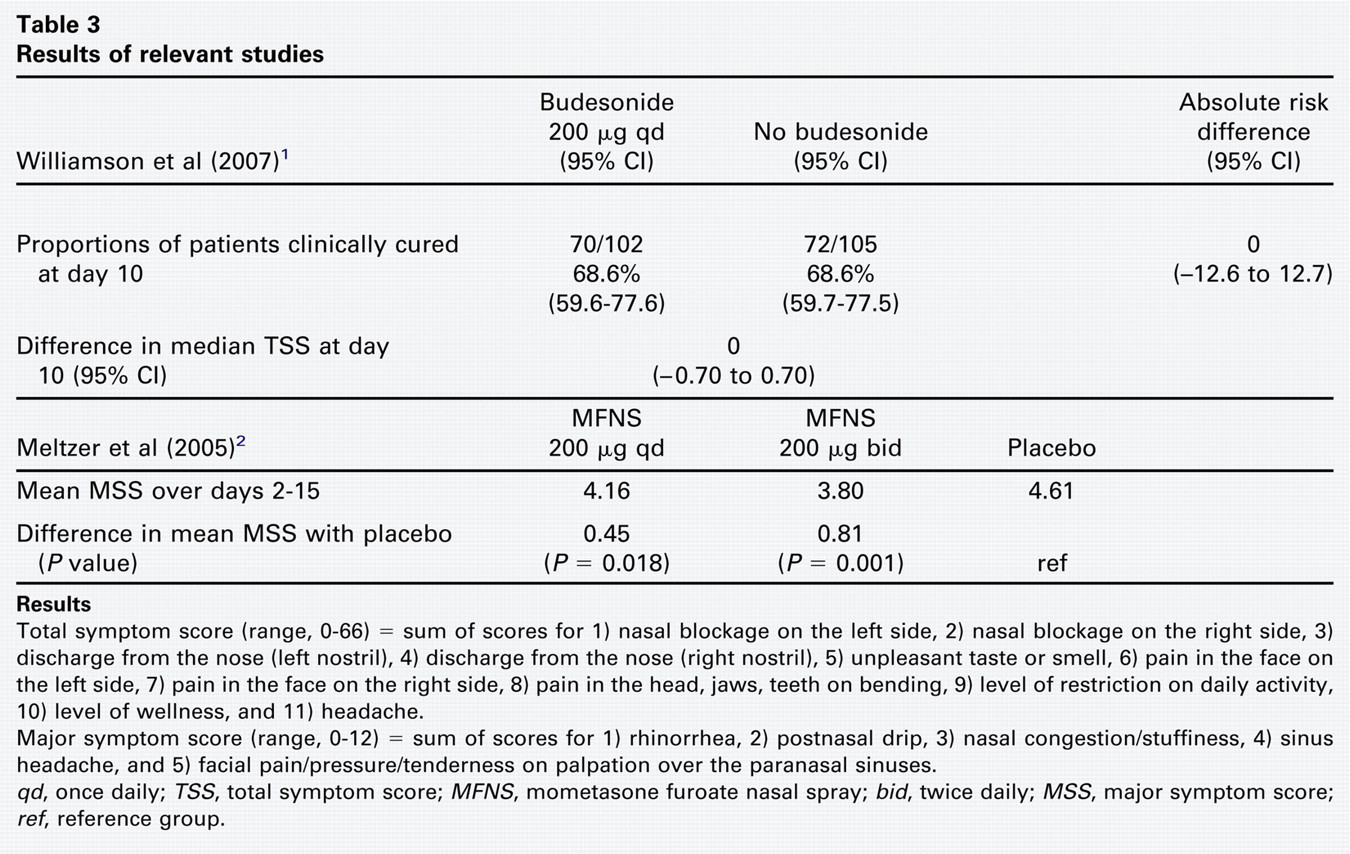
Total symptom score (range, 0-66) = sum of scores for 1) nasal blockage on the left side, 2) nasal blockage on the right side, 3) discharge from the nose (left nostril), 4) discharge from the nose (right nostril), 5) unpleasant taste or smell, 6) pain in the face on the left side, 7) pain in the face on the right side, 8) pain in the head, jaws, teeth on bending, 9) level of restriction on daily activity, 10) level of wellness, and 11) headache.
Major symptom score (range, 0-12) = sum of scores for 1) rhinorrhea, 2) postnasal drip, 3) nasal congestion/stuffiness, 4) sinus headache, and 5) facial pain/pressure/tenderness on palpation over the paranasal sinuses.
qd, once daily; TSS, total symptom score; MFNS, mometasone furoate nasal spray; bid, twice daily; MSS, major symptom score; ref, reference group.
Meltzer et al 2 performed a double-blind, double-dummy, randomized, placebo-controlled trial to evaluate the efficacy of mometasone furoate nasal spray (MFNS) monotherapy (200 μg once daily and 200 μg twice daily) versus amoxicillin and placebo in 981 patients (≤ 12 years) with signs and symptoms of acute rhinosinusitis. Acute rhinosinusitis was defined as uncomplicated illness (≥ 7 days but ≤ 28 days) with a low MSS (MSS ≥ 5 but ≤ 12) and no more than three of the five symptoms rated as severe. Moreover, patients were excluded if they had signs and symptoms of fulminant bacterial rhinosinusitis. The study showed that MFNS 200 μg twice daily led to a 9 percent relative improvement in mean MSS over days 2 to 15 compared to placebo (3.80 vs 4.61; absolute difference in mean MSS: 0.81, P < 0.001) (Table 3). MFNS 200 μg once daily was also statistically significantly superior to placebo, but the effect was smaller than MFNS 200 μg twice daily (absolute difference in mean MSS: 0.45, P = 0.018).
Translating Evidence into Practice?
Before translating the evidence into practice, there are several potential limitations that deserve further discussion. First, Williamson et al 1 used a factorial design, which is the most efficient design for testing more than one hypothesis. Such a design requires, however, a specific data-analysis method with assessment for treatment interactions, which results in loss of statistical power to detect differences between treatment groups. Since the confidence intervals around the reported association measures are relatively small, we do not consider this a drawback.
Second, Meltzer et al 2 did not report concealment of allocation. Consequently, the risk of bias cannot be entirely excluded. Moreover, the primary endpoint (i.e., mean MSS over days 2-15) used by Meltzer et al 2 can be criticized from a clinical point of view. Although methodologically correct, the presented outcome does not provide information on the absolute effect of INCS. It therefore would have been clinically more informative if the absolute numbers of patients with symptom resolution at day 15 for the treatment groups were presented. Furthermore, the size of the reported effect in this study is too modest to exceed the threshold for clinical importance.
Third, the differences in study population between the two critically appraised studies may have had an important impact on the results. Williamson et al 1 included patients with a minimum of two Berg and Carenfelt criteria 22 (purulent nasal discharge with unilateral predominance, local pain with unilateral predominance, purulent nasal discharge bilaterally, and pus on inspection inside the nose). These criteria have been suggested to increase the likelihood of an underlying bacterial infection, and antibiotics might therefore be more effective than INCS. However, neither antibiotic nor INCS treatment was found to be effective. As opposed to Williamson et al, 1 patients included by Meltzer et al 2 had less severe symptoms and a reduced likelihood of a bacterial infection. As a consequence, these patients were more likely to benefit from INCS rather than antibiotic treatment. However, the differences between both INCS groups and the placebo group reported by Meltzer et al 2 are modest.
Finally, one can argue about the dosage of INCS used in both trials. Williamson et al 1 used INCS 200 μg once daily in both nostrils, while Meltzer et al 2 showed that INCS 200 μg twice daily had a larger treatment effect. Moreover, patients in both studies did not use decongestant nose drops before application of INCS; this might have led to a suboptimal treatment effect. Therefore, additional large randomized, placebo-controlled trials on the efficacy of higher-dosage (intranasal) corticosteroids, in addition to decongestant nose drops, are warranted to provide a more definite answer on the use of this therapy in patients with acute rhinosinusitis.
Conclusion and Recommendation
As the clinical beneficial effect of INCS monotherapy compared to placebo has not been established in patients with acute rhinosinusitis, watchful waiting in our female patient appears to be justified.
Author Contributions
Disclosures