
Abstract
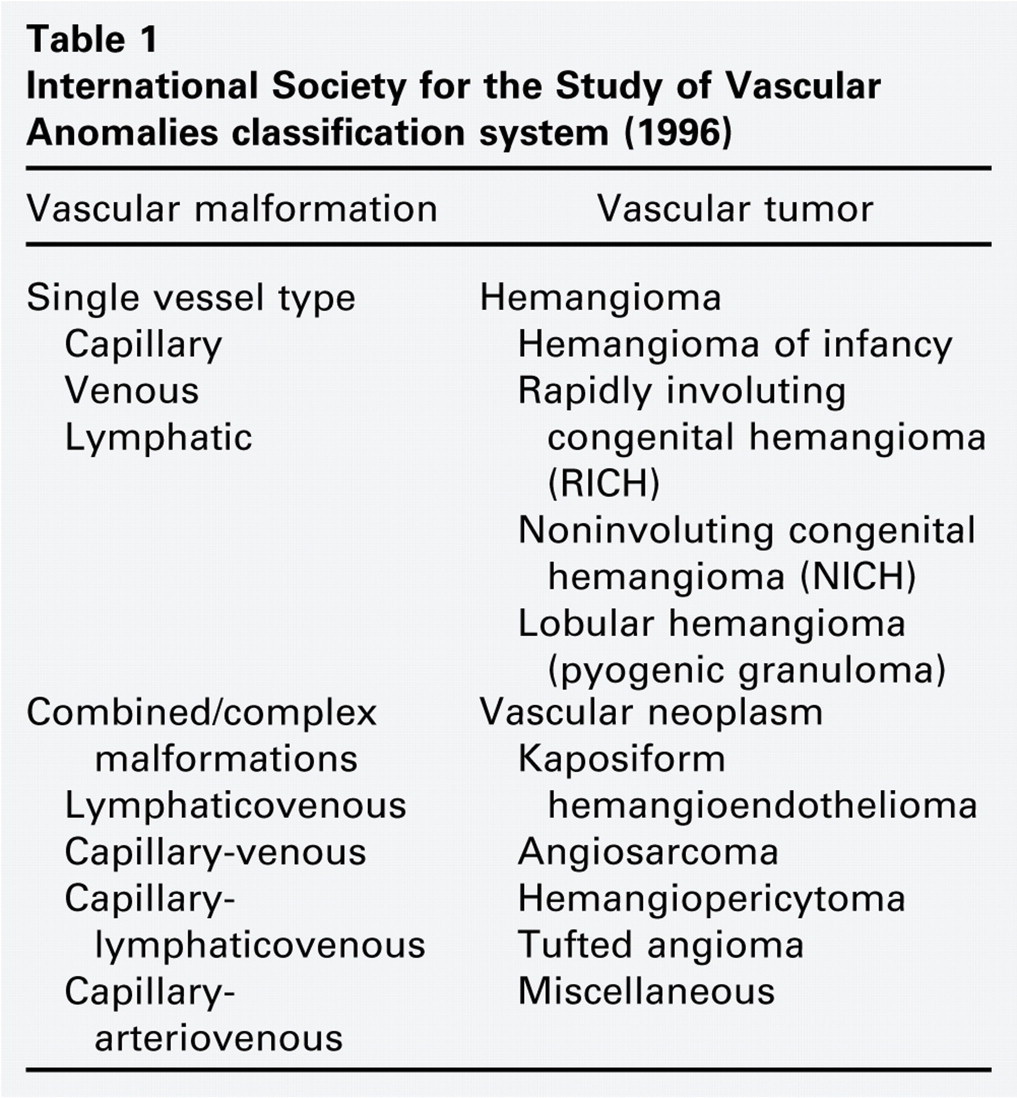
In recent years, much has changed in our understanding of vascular anomalies. These lesions are now categorized as either “vascular tumors” or “vascular malformations,” based upon clinical, histologic, and biochemical differences (Table 1). For example, Mulliken and Glowacki described differences between hemangiomas of infancy and other vascular anomalies. 1 Subsequently, North et al described the hemangioma endothelial marker glucose 1 transporter (GLUT1) as a histologic way to differentiate these lesions from other vascular anomalies. 2 A better understanding of the biochemical makeup and clinical differences between these lesions has changed prognostication and enabled treatment innovation. Insufficient studies have been conducted to determine if lymphatic malformation (LM) treatment innovation has improved treatment outcomes.
International Society for the Study of Vascular Anomalies classification system (1996)
This document summarizes current knowledge of LM development, LM biology, and measurement of LM treatment outcomes.
The Lymphatic System and the Pathogenesis of Lymphatic Malformation
LMs, previously known as cystic hygromas or lymphangiomas, are classified as low-flow vascular malformations. Seventy-five percent of all LMs occur in the head and neck region. Generally, the symptoms are related to the size of the malformation and to the perturbation of the adjacent tissues altering structure and function. The etiology of LM is unknown. It is generally considered a nonmalignant primary disorder of the lymphatic system, although this has not been formally demonstrated.
The lymphatic system is an arborized hierarchy of vessels designed to unidirectionally drain extravasated fluid from the peripheral tissue, localize antigen to draining regional lymph nodes, and absorb intestinal fat. 3 A great deal of recent progress has provided the tools to study the lymphatic system at the cellular and molecular level. Unlike several lymphatic disorders, such as lymphedema distichiasis 4 and Milroy disease, 5 our knowledge of the pathogenesis of LM is modest. The goal of this section is to review the development of the lymphatic system, understand the published findings related to LM biology, and outline important basic science questions that need to be addressed to provide improved patient care.
Development of the Lymphatic System
Lymphatic vessels develop from mesodermally derived vascular endothelial cells. In 1902, Florence Sabin proposed the most well accepted model of developmental lymphangiogenesis in which cervical lymph sacs budded from the cardinal veins and spread by endothelial sprouting and remodeling, ultimately establishing a functional lymphatic system. 6 In contrast to blood capillaries, lymphatic capillaries are thin-walled vessels with loose intercellular connections, few smooth muscle cells and pericytes, and little basement membrane. These characteristics are thought to make lymphatic capillaries highly permeable to fluid, pathogens, and tumor cells.
In the last decade, some molecular details of embryologic lymphangiogenesis have been described. After the cardinal veins have formed, a polarized subset of venous endothelial cells express propero-related homeobox 1 (Prox1). Expression of Prox1 is required and sufficient to confer a lymphatic developmental pathway. 7 It has become well appreciated that the family of vascular endothelial growth factors and receptors, particularly vascular endothelial growth factor C (VEGF-C) and its primary receptor vascular endothelial growth factor receptor-3 (VEGFR-3), are important—if not essential—for developmental lymphangiogenesis. 8 Table 2 is a partial list of gene products thought to be critical during embryologic lymphangiogenesis.
Gene products critical to embryologic lymphangiogenesis
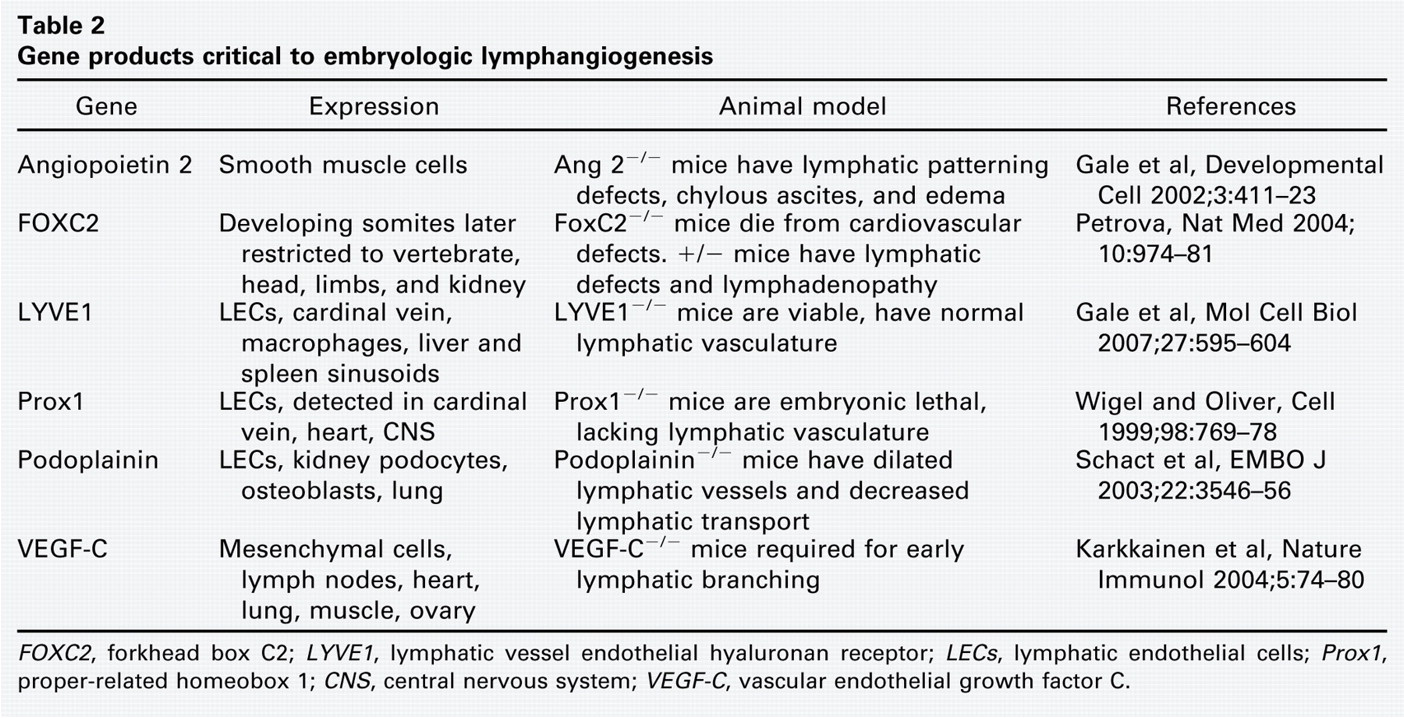
FOXC2, forkhead box C2; LYVE1, lymphatic vessel endothelial hyaluronan receptor; LECs, lymphatic endothelial cells; Prox1, proper-related homeobox 1; CNS, central nervous system; VEGF-C, vascular endothelial growth factor C.
Several preclinical models have demonstrated postembryologic lymphangiogenesis to occur in cancer progression and inflammatory conditions. 9 , 10 Signals mediated by VEGFR-3 and the Tie2 receptor appear to be critical for lymphatic remodeling and growth in the tumor and inflamed microenvironment. Indeed, certain tumors induce lymphatic growth, thus enabling lymphatogenous tumor metastasis. 11
Pathogenesis of Lymphatic Malformation
Lymphatic malformations are generally regarded as benign growths of the lymphatic system, although the data supporting this classification are based upon histological characteristics. Although the etiology of LM is unknown, it is instructive to consider that LM may result from disorders that are intrinsic or extrinsic to the lymphatic system. One in 250 fetuses are diagnosed with nuchal lucency, an ultrasound finding of early LM. 12 However, a significant degree of remodeling must occur, as the incidence of LM at birth is 1 in 5000. This observation suggests that lymphatic overgrowth and remodeling occurs frequently and in certain cases is dysregulated, resulting in the clinical presentation of LM at birth. A genetic etiology is suggested by the observation that up to 40 percent of LMs detected in utero occur in individuals with chromosomal anomalies, such as trisomy 21 and Turner's syndrome. 13
Conditions that result in the inappropriate expression of lymphatic-specific molecules may cause or contribute to embryologic or postembryonic LM development. Although it has not been studied in a comprehensive manner, aberrant expression of the molecules outlined in Table 2 could increase the density and complexity of the lymphatic system. Several groups have demonstrated that the lymphatic endothelial cells derived from individuals with LM express the anticipated array of lymphatic-specific markers with the exception of increased expression of vascular endothelial growth factor receptor-3 (VEGFR-3). 14 - 16 The significance of this finding is unknown, but it suggests an autocrine regulation of LM. In vitro analysis of LM endothelium showed no functional differences when compared to normal lymphatic endothelium. 17
Alternatively, cells or factors extrinsic to the lymphatic system (i.e., the microenvironment) could potentiate the growth of the lymphatic system. Simple histological evaluation of LM tissue stained with hematoxylin-eosin and immunohistochemistry demonstrates that this tissue is complex (Fig 1). The radiographic characterization of LM (i.e., macrocystic, microcystic) is not apparent histologically. 17 In all LM, the lymphatic vessels are thin-walled, irregularly shaped, and heterogenous in size. The stroma or extralymphatic tissue is complex, with abundant fibroblasts, foci of leukocytes, collections of adipocytes, and muscle cells. Recently, the presence of increased numbers of interferon-producing cells in LM has been described, emphasizing that many factors could contribute toward LM persistence. 18 Immune or other cells that secrete lymphangiogenic factors may stimulate the growth of otherwise normal lymphatic vessels.
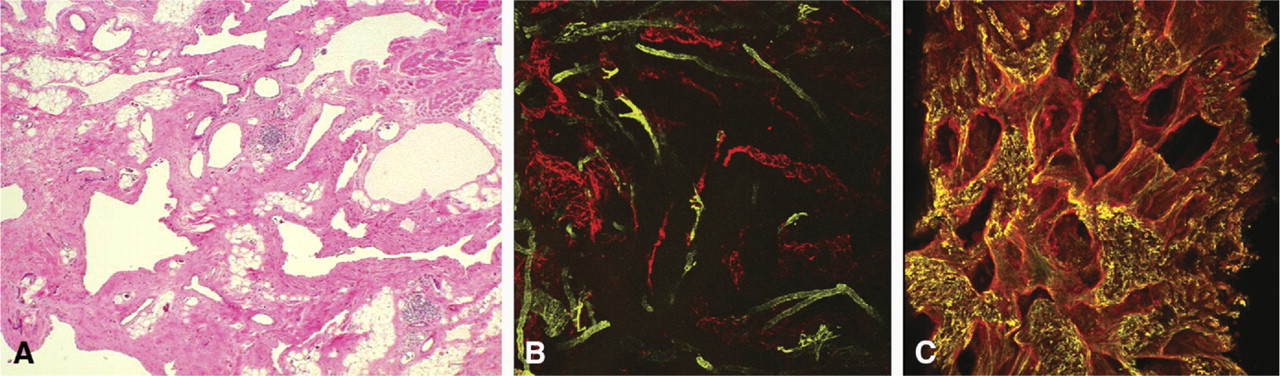
Lymphatic malformation histology. (
Future Directions in Lymphatic Malformation Basic Science Research
An orderly approach addressing specific questions related to intrinsic or extrinsic factors that promote embryologic or postembryologic LM development is needed to advance this field of study. Understanding these basic science principles may allow the development of lymphatic-specific therapeutic strategies that alter the clinical course of patients with LM.
Evaluation of Treatment Outcomes in Lymphatic Malformation Treatment
Head and neck LM assessment and treatment have changed and improved over the past 15 years based on systematic and standardized evaluations. Factors that allowed this change include simplified LM nomenclature, an LM staging system, refined imaging allowing structural macrocystic and microcystic differentiation, and treatment innovations in both sclerotherapy and surgery (Fig 2). 19 - 23 Most of these factors arose from astute clinical observation and experience. 24 Development of an evidence base for LM can be aided through standardized questions directed to the patient and/or the patient's caregiver that measure how treatment affects normal functions such as breathing, speaking, and eating. Currently, there is no way to measure these malformations' impact on function before or after treatment because the only current measure of treatment success is lesion ablation. This is inadequate, as the majority of higher-stage LMs cause continued morbidity and are never completely “cured.” Understanding the perspective of the patient or caregiver is a critical adjunct to clinical assessment. Further refinement in LM therapy will require systematic standardized data collection to develop decision factors that extend beyond mere clinical observation and are instead based on objective clinical markers of disease severity and measures of specific treatment outcomes.
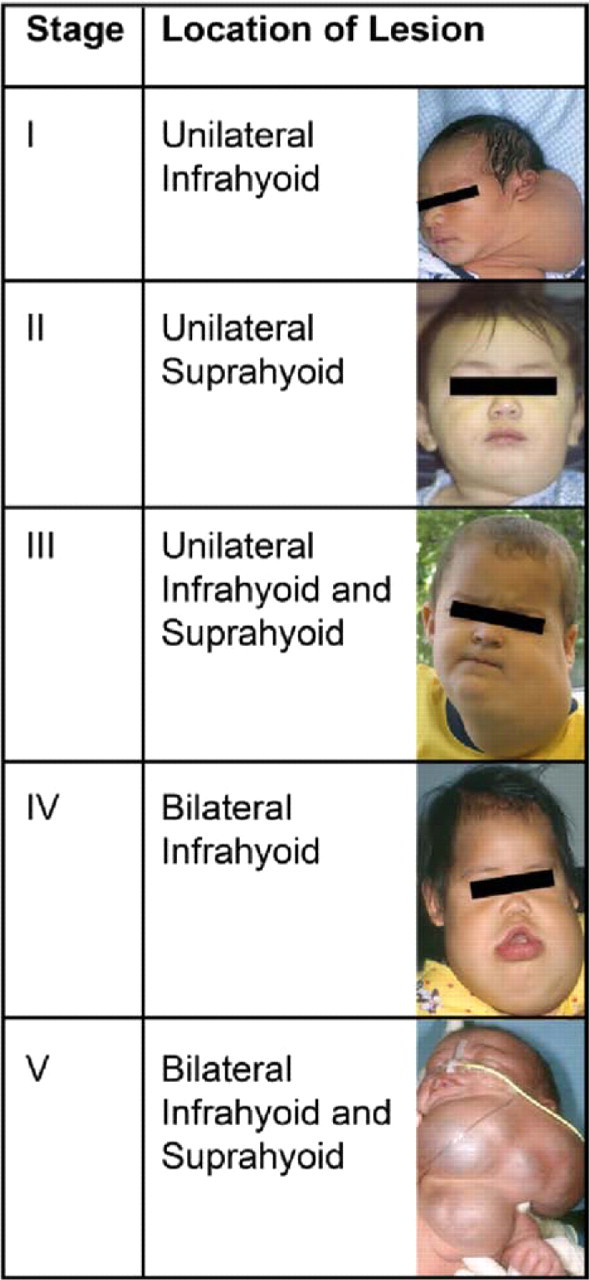
Staging of cervicofacial lymphatic vascular malformation [Reference 4].
In addition to expanding clinical knowledge of LM, LM treatment can be improved through better understanding LM development and biology. Refinement of invasive LM treatment should be possible by correlating an understanding of LM biology with LM structural characteristics and volume, determined with pretreatment imaging, with treatment outcome. Through longitudinal data collection of affected patients, a broader picture of the natural history of LM can be determined, furthering our understanding of the disease burden associated with LM (Figs 3-5).
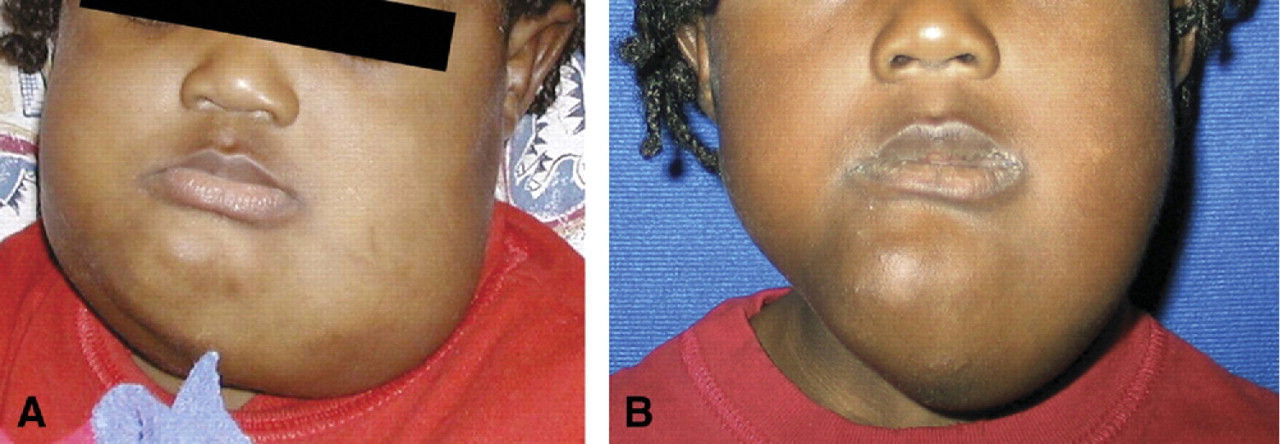
Before (

Enlarged, bleeding tongue in stage IV lymphovenous malformation in a patient with lymphocytopenia.

Lymphatic malformation regression. Stage I posterior cervical macrocystic malformation with spontaneous regression. (
Over the past decade, the science of treatment outcomes has been applied to surgery at the healthcare system level. 25 , 26 This has resulted in scrutiny of regional and institutional variation of care, which is also present in LM treatment. Cost of caring for a specific disease is now quantifiable. 27 LM treatment costs continue to rise, thus raising the question of how to measure LM treatment efficacy. 28 Longitudinal collection of data associated with clinical encounters can help determine treatment efficacy as judged by multiple clinically important variables. Careful consideration must be given to what is evaluated in LM treatment, since all the problems associated with accurately assessing cost of care in pediatric patients are present. 29
Along with the better “objective” biologic measures and cost-of-care analyses, the functional health status of an affected individual with a chronic disease, as well as the changes in this status associated with treatment, can now be determined through application of valid clinical health status measurement instruments. 30 Investigation is ongoing among the authors to develop a clinically relevant instrument to measure the impact of LM treatment on function. Additionally, a cost-of-care analysis is being conducted between institutions using primarily nonsurgical management as compared to surgical management. By assessing disease-specific patient-level data along with clinical cost data, findings from these trials become much more relevant. Because LMs are most often diagnosed in children, health status is difficult to determine, as proxy reporting is necessary and there are significant changes over time in affected individuals. 29 Despite this difficulty, use of serial visual analogue scales of LM-specific disease severity (i.e., recurrent LM inflammation, dysphagia, bleeding, disfigurement, etc.) could be applied in this population and will probably be sensitive to changes in health status. Additionally, use of retrospective proxy report transition instruments is helpful in assessing patient satisfaction with treatment in a manner that would be applicable to clinical practice, provided it is obtained in a validated manner. 31
In summary, LM treatment can be further improved through collection of longitudinal treatment and evaluation data. The tools to do this are available or are being developed. 32 This information can be used to develop further biologic measures to predict treatment efficacy. Additionally, this same information can be used to improve our understanding of the cost of LM treatment. Finally, with the addition of patient and proxy reports on health status and changes in response to treatment, a broad perspective of all types of LM treatment efficacy and refinement will be obtained.
Summary of LM Basic Science and Clinical Outcome Measures
The etiology and pathogenesis of head and neck LM are poorly understood. Future characterization of LM endothelial and stromal cells may lead to biologically based treatment. Current LM treatment planning is primarily determined by the presence of or possibility of functional compromise. Measuring treatment efficacy is in its infancy, but steps are being taken to improve this in a disease-specific manner.
Author Contributions
Disclosures