
Abstract
© 2010 American Academy of Otolaryngology-Head and Neck Surgery Foundation. All rights reserved.
Videofluoroscopic swallowing study (VFSS) and fiberoptic endoscopic evaluation of swallowing (FEES) are the most widely used methods for diagnosing dysphagia and assessing its management in an effort to reduce the incidence of pneumonia. Limitations of VFSS have been widely described in the literature. 2 – 4 There is a lack of quantitative diagnostic evidence regarding FEES in children, which is not true for adults.
The aim of the present study is to determine the accuracy of FEES in the diagnosis of swallowing disorders in children.
Materials and Methods
Patients
Thirty children with different diseases (Table 1) were prospectively evaluated using VFSS and FEES between October 2004 and November 2006. All patients were referred from the outpatient clinic and hospital admission desk of Hospital da Criança Santo Antônio (HCSA) due to suspected dysphagia.
Ethical Aspects
This study was submitted to and approved by the Committee of Ethics in Research of Complexo Hospitalar Santa Casa, under number 193/02. Parents or guardians of children were informed about the study and signed a consent form.
Equipment and Materials
VFSS was performed with a Siemens Tridoros 1000 device (Siemens, New York, NY) with an image intensifier, connected to a Panasonic AG1320 videocassette recorder (Panasonic, Los Angeles, CA) and to a Siemens M44-2 video monitor, with the use of a collimator focused on the area of interest.
Sample characteristics
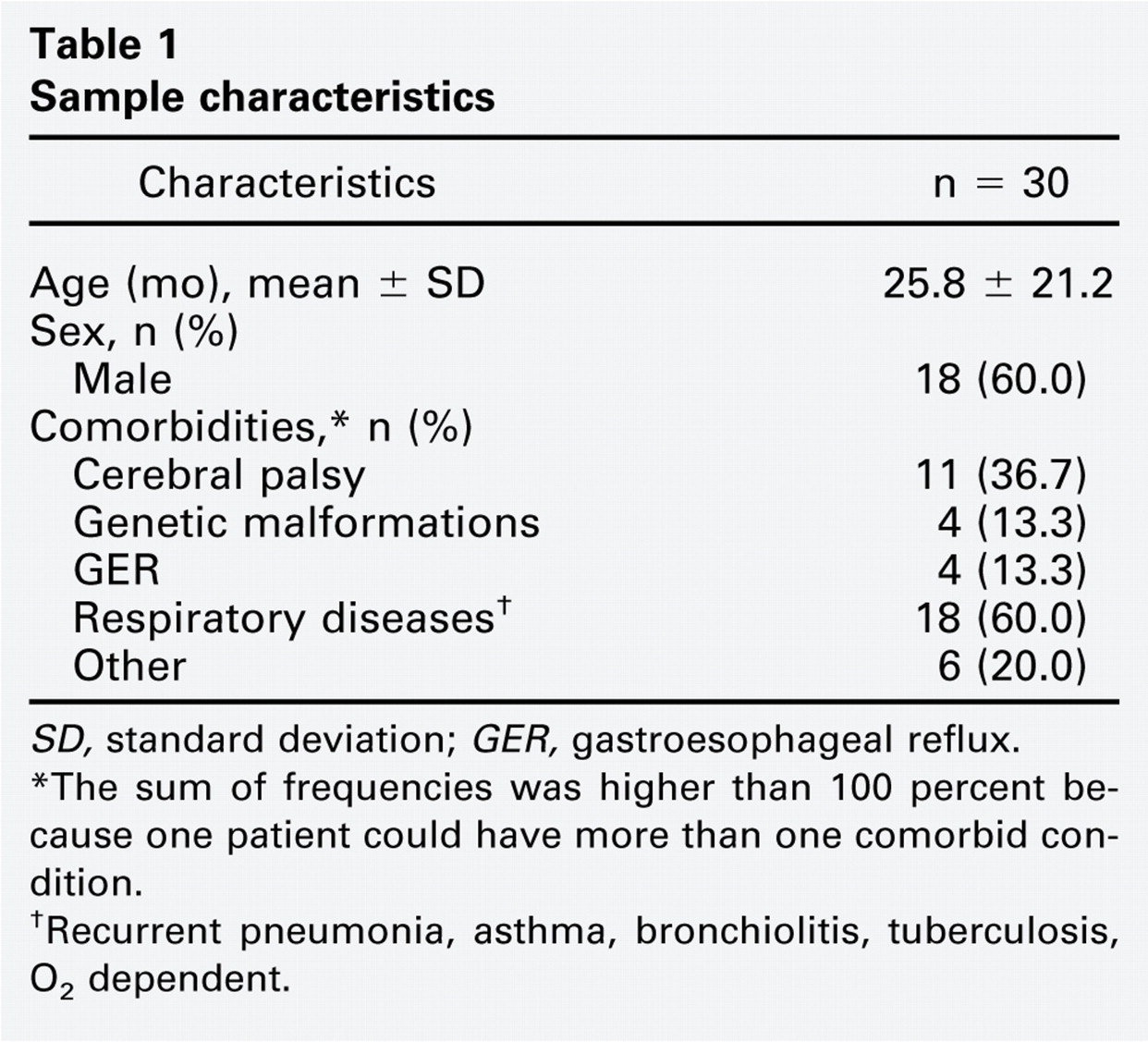
SD, standard deviation; GER, gastroesophageal reflux.
∗ The sum of frequencies was higher than 100 percent because one patient could have more than one comorbid condition.
† Recurrent pneumonia, asthma, bronchiolitis, tuberculosis, O2 dependent.
FEES was performed with a 3.2-mm Machida fiberoptic nasopharyngolaryngoscope (Machida Endoscope Co., Ltd., Tokyo, Japan). The captured images were transferred to a Sony video monitor and recorded onto a Sony SVO-1330 videocassette (Sony Corp., Tokyo, Japan). A Storz halogen light source (Karl Storz GmbH & Co., Tuttlingen, Germany) was used.
Procedures
All the procedures were carried out by an otolaryngologist (J.F.L.N.) from the Division of Pediatric Otolaryngology (FEES) in the surgical center, due to operational reasons, and by a radiologist from the Division of Radiology (VFSS) of HCSA, Porto Alegre, Brazil. The speech therapist (A.P.S.) participated in all the procedures. The diagnostic procedures were carried out without any preset order, following the most convenient sequence.
After the procedures, the examiners immediately issued a report of their assessments. Both procedures were videotaped. Another otolaryngologist (P.S.), who was blinded to the examination results and to patient histories, assessed the FEES recordings in order to determine the interobserver agreement.
All patients who were analyzed were given food and liquids with the same consistency in both procedures. For preparation of the puree consistency, a modified instant cornstarch product, Nutilis (Support, São Paulo, Brazil), was used as thickener.
Only these two consistencies were chosen in order to have a single evaluation protocol, because patients had different disorders and were of different ages. The puree consistency was always offered first because the liquid consistency was progressively more difficult to swallow. 4
The thickener (1&1/2; measuring spoon) was added to MID (Ajinomoto, São Paulo, Brazil) apple juice powder diluted in 100 mL of water in order to obtain a puree honey consistency. The liquid consistency included apple juice without the thickening component.
In VFSS, the preparations were mixed with Bariogel (Cristália, Belo Horizonte, Brazil) apple-flavored barium sulfate suspension at the concentration of 100 percent for better endoscopic visualization of bolus transit.
In FEES, the preparations were mixed with a food dye. A liquid yolk-colored food dye (Mix, São Paulo, Brazil) was used for the puree consistency and a liquid indigo blue food dye (Mix) was used for the liquid consistency. The aim of adding food dyes to the preparations was to obtain better visualization of the food bolus during swallowing. The patients were evaluated in the sitting position in both procedures.
Four parameters were assessed for the diagnosis of dysphagia: 1) early pharyngeal spillover—when food escapes into the pharynx from the back of the mouth before the swallowing reflex is triggered; 2) pharyngeal residues—presence of saliva, secretions, or swallowed materials, either contrast-enhanced or not, accumulated in the valleculae, on the lateral or posterior pharyngeal walls, or in the piriform sinuses, after deglutition; 3) laryngeal penetration—presence of contrast or food residues encroached on the airway, above the vocal folds with or without coughing; and 4) laryngotracheal aspiration—presence of contrast-enhanced or noncontrast materials below the vocal folds. 2 , 5
Data Analysis
The results were typed into an Excel (Microsoft Corporation, Redmond, WA) spreadsheet, version 2000, and then analyzed by SPSS (Statistical Package for the Social Sciences; SPSS Inc., Chicago, IL), version 13.0.
The continuous variables were described as mean, standard deviation, median, and interquartile range. The categorical variables were described as absolute and relative frequencies. The kappa coefficient was used to assess interobserver agreement and the diagnostic methods. Sensitivity, specificity, and positive and negative predictive values were calculated for the diagnostic evaluation of FEES, using the VFFS as the gold standard. P values ≤0.05 were regarded as statistically significant.
Results
Most of the 30 children were male (60%). The mean age was 25.8 months ± 21.2 months, and the median was 21.5 months (range: 10.5–37.3 months). The major reasons for the referral of these infants to FEES were the presence of respiratory disease and cerebral palsy (Table 1).
Table 2 shows the absolute and percentage frequency of abnormal findings in the study population for VFSS and Observers 1 and 2 of FEES.
In FEES, the kappa coefficient showed good interobserver agreement for laryngeal penetration of puree residues (κ = 0.712, P < 0.001), laryngeal penetration of the liquid residues (κ = 0.733, P < 0.001), and laryngeal aspiration of liquid residues (κ = 0.667, P < 0.001). Pharyngeal residue with liquid consistency (κ = 0.923, P < 0.001) and aspiration with puree consistency (κ = 1.00) yielded very good agreement rates. Early spillover of liquid residues (κ = 0.450, P = 0.007) showed moderate agreement. Early spillover of puree residues (κ = 0.323, P = 0.065) and pharyngeal residue of puree consistency (κ = 0.296, P = 0.091) showed weak agreement 6 (Table 3).
Frequency of abnormal findings (n X 30)
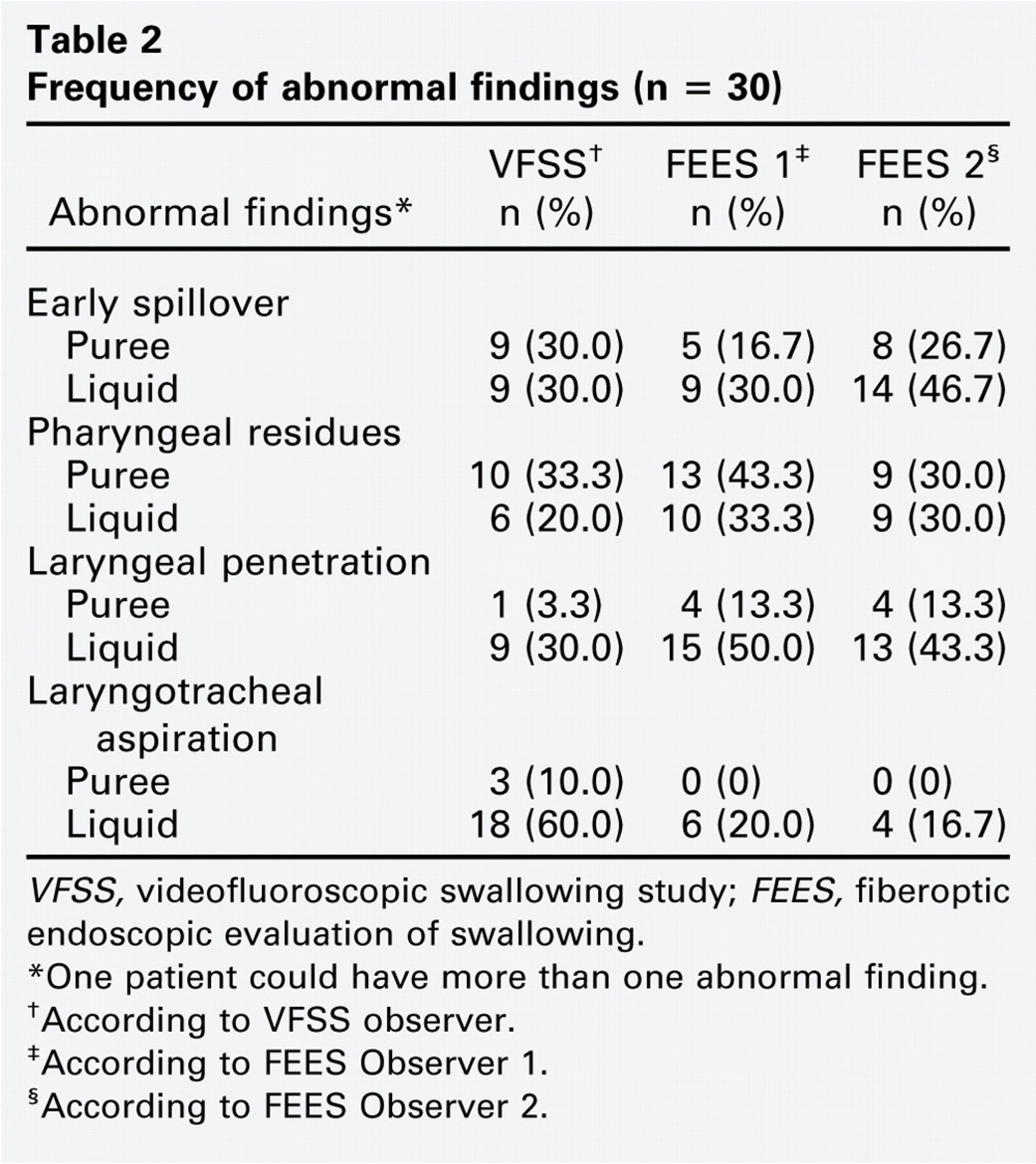
VFSS, videofluoroscopic swallowing study; FEES, fiberoptic endoscopic evaluation of swallowing.
∗One patient could have more than one abnormal finding.
†According to VFSS observer.
‡According to FEES Observer 1.
§According to FEES Observer 2.
Table 4 shows the agreement regarding the diagnostic results of FEES obtained by Observers 1 and 2 when compared with VFSS. Kappa coefficients yielded poor values, except for pharyngeal residues, which showed moderate agreement, with a statistically significant P value, as well as higher agreement for Observer 1.
Tables 5 and 6 show the diagnostic assessment of FEES according to Observers 1 and 2. The specificity of several parameters was often higher than their sensitivity. Tracheal aspiration had the highest specificity, with the largest positive predictive value across the four parameters assessed by both observers.
Discussion
VFSS has been regarded as the standard diagnostic method by several authors. 5 , 7 The main advantages of VFSS in relation to other methods that assess swallowing are the integrated observation of all the swallowing phases, that is, observation of the oral preparatory phase and oral transit phase; of the elevation and anterior displacement of the hyoid-larynx complex; of the upper esophageal sphincter opening; and of esophageal transit.
Jones, 8 however, points out four technical limitations concerning VFSS: 1) limited radiation exposure; 2) uncooperative patients with postural or emotional limitations; 3) preparation of the physical structure and materials, in addition to patient transportation; and 4) inadequate examination for an in-depth investigation of anatomical anomalies.
Studies have demonstrated that VFSS is a method that relies on subjective visual judgment, with a learning curve for its interpretation. 9 , 10 Scott et al 9 conducted an inter-rater reliability study using VFSS as the evaluation method. They used a protocol in which they assessed 11 aspects of swallowing, with a five-point rating scale. Observations were made by nine speech pathologists with different levels of expertise in VFSS, as follows: Condition 1: individually after careful reading; Condition 2: together with other speech pathologists in group discussion; and Condition 3: individually after group discussion. The levels of agreement were higher and statistically significant regarding the swallowing of puree foods (t32 = 2.21, P < 0.05). The levels of agreement were lower for Condition 1. Higher levels were obtained for Condition 2, with the swallowing of puree and liquid consistencies, with a significance of 0.05 or higher. The level of agreement was higher in Condition 3 than in Condition 1. This study shows the complexity in the assessment of VFSS. Despite its broader use, clinicians and raters should be aware of the limitations related to the reliability and validity of this method. Nevertheless, as it was the first method to be developed, and as it is of great utility when used by experienced professionals, VFSS continues to be the gold-standard diagnostic method.
Logemann et al10 analyzed the effect of four hours of education on the interpretation of radiographic studies (identification of head and neck anatomy and VFSS). Results indicate that a short (four hours) interactive and dynamic learning experience may remarkably improve the training in the accurate identification of head and neck anatomy and of swallowing disorders.
Interobserver∗ agreement for fiberoptic endoscopic evaluation of swallowing
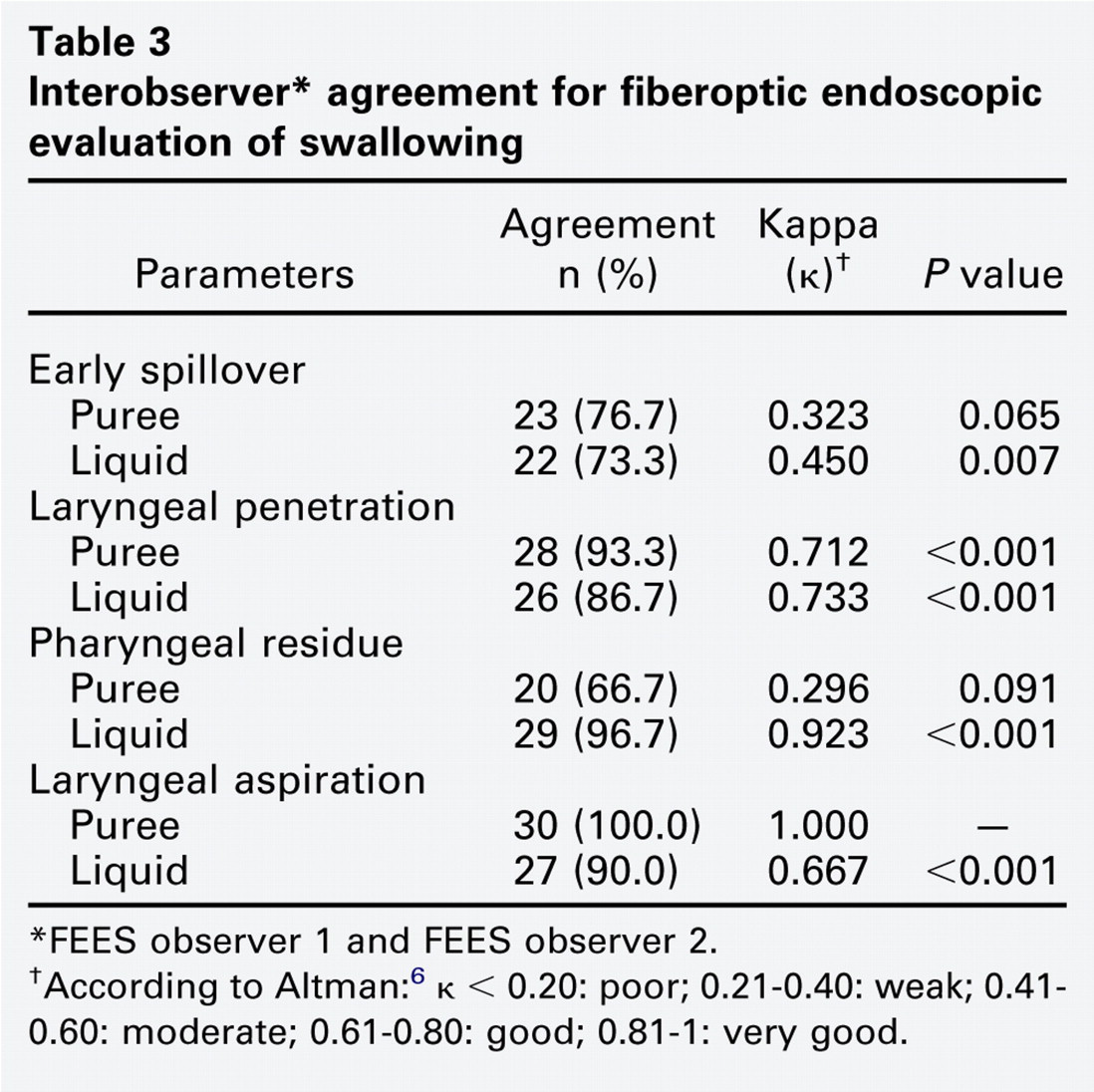
∗FEES observer 1 and FEES observer 2.
†According to Altman: 6 κ < 0.20: poor; 0.21–0.40: weak; 0.41–0.60: moderate; 0.61–0.80: good; 0.81–1: very good.
Diagnostic agreement between fiberoptic endoscopic evaluation of swallowing and videofluoroscopic swallowing study
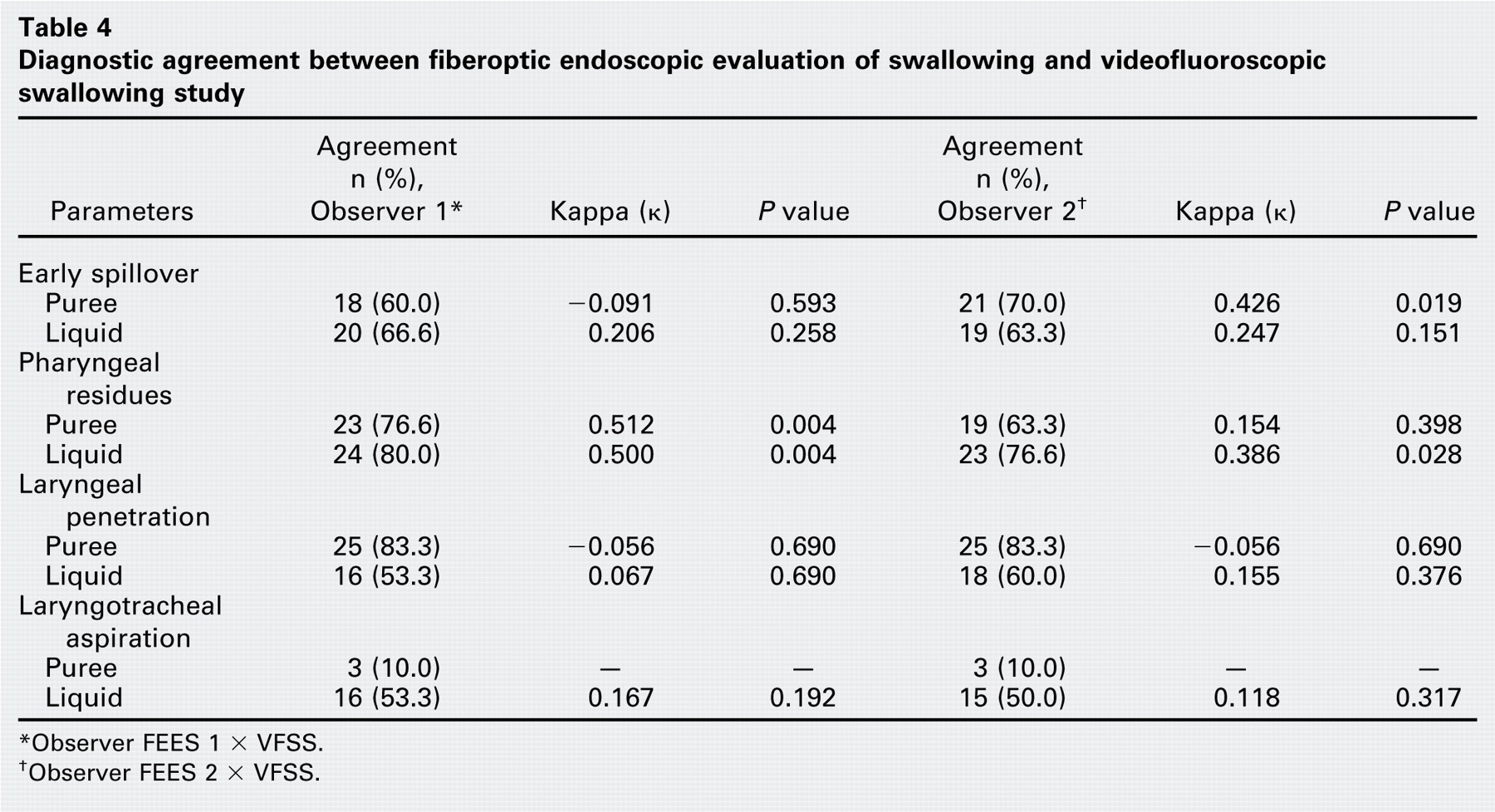
∗Observer FEES 1 x VFSS.
†Observer FEES 2 x VFSS.
Langmore et al 11 brought a new perspective to the assessment of oropharyngeal dysphagia with the description of FEES. The advantages of this new diagnostic tool are its potential use in cases with limited assessment by VFSS (assessment outside the radiology suite; assessment of patients with limiting postural problems; and of patients at great risk for laryngotracheal aspiration during VFSS).
The first study comparing FEES with the gold standard (VFSS) was carried out in adult patients in 1991, as reported by Langmore et al. 12 The results confirmed high levels of agreement, sensitivity, specificity, and positive and negative predictive values. Previous comparative studies in adult patients after cerebrovascular accidents, head and neck surgeries, and neurological diseases, among others, also revealed high levels of agreement between the methods.
In the literature, there is only one study including infants and children, conducted by Leder and Karas 4 in 2000, which showed complete agreement in the case of laryngeal penetration and aspiration in 30 individuals aged 11 days to 20 years. Only seven of them were randomized into the comparative study. The remaining 23 individuals were submitted to FEES only. The other parameters were not assessed.
Diagnostic assessment of fiberoptic endoscopic evaluation of swallowing according to Observer 1
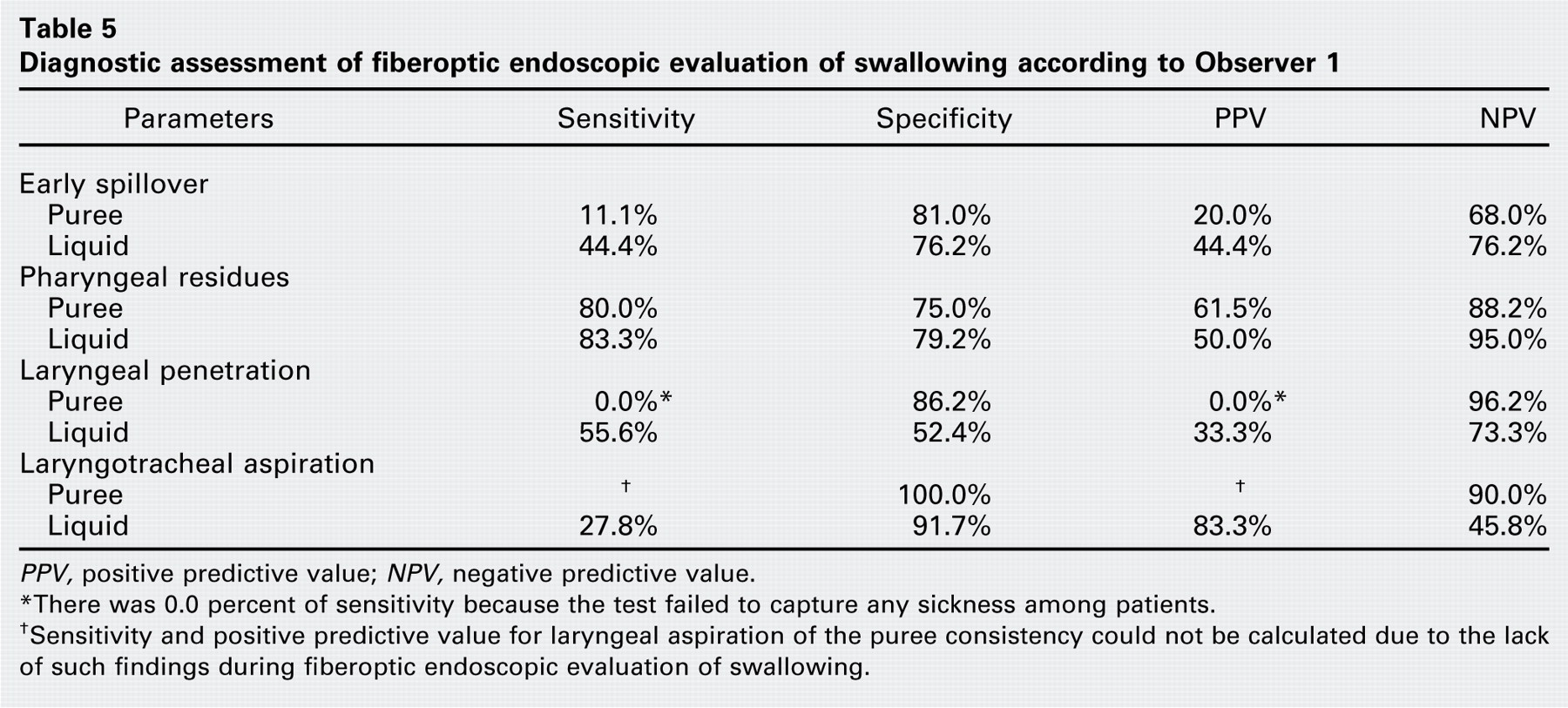
PPV, positive predictive value; NPV, negative predictive value.
∗There was 0.0 percent of sensitivity because the test failed to capture any sickness among patients.
†Sensitivity and positive predictive value for laryngeal aspiration of the puree consistency could not be calculated due to the lack of such findings during fiberoptic endoscopic evaluation of swallowing.
Diagnostic assessment of fiberoptic endoscopic evaluation of swallowing according to Observer 2
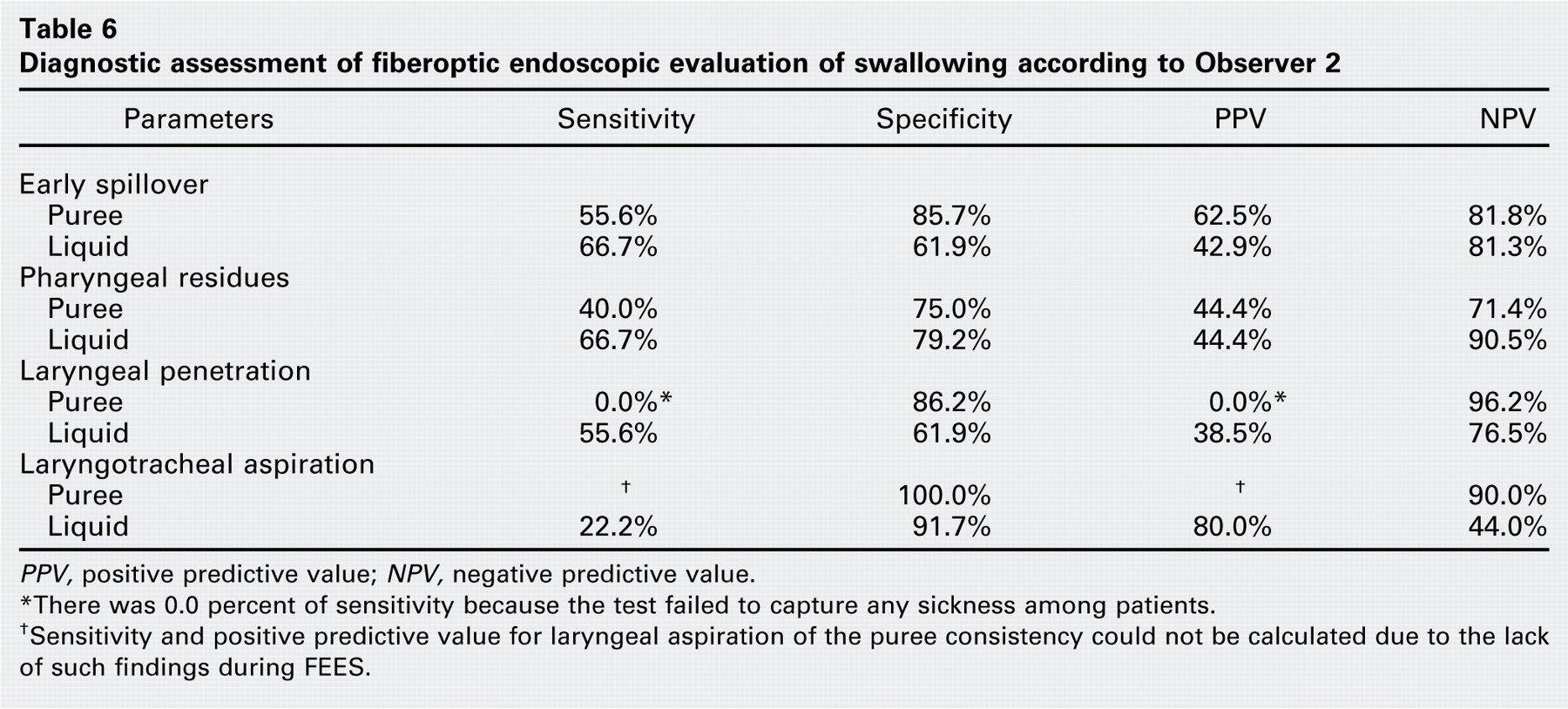
PPV, positive predictive value; NPV, negative predictive value.
∗There was 0.0 percent of sensitivity because the test failed to capture any sickness among patients.
†Sensitivity and positive predictive value for laryngeal aspiration of the puree consistency could not be calculated due to the lack of such findings during FEES.
Our study compared the assessment results, based on four functional parameters (early spillover, pharyngeal residues, laryngeal penetration, and laryngotracheal aspiration), obtained by VFSS and FEES in infants with suspected dysphagia.
FEES yielded good interobserver agreement for all parameters, especially for laryngeal penetration and aspiration. This information is important because, according to Friedman and Frazier, 13 85 percent of 125 pediatric patients with deep laryngeal penetration experienced aspiration, suggesting a strong correlation between these events. This interobserver agreement demonstrates that FEES is a method with reproducible results.
Weak agreement was found between Observers 1 and 2 regarding the VFSS diagnostic method. Perhaps the fact that infants were crying almost all the time during the FEES, which shows that it is difficult to make them cooperate, might have hindered the assessment. It was noted that crying increases the latency to trigger the swallowing reflex, favoring the occurrence of early spillover, laryngeal penetration, pharyngeal residues, and laryngotracheal aspiration to liquid consistency. The management of the puree consistency resulted in better cooperation by the children. Despite this improvement, sensitivity must be maintained during FEES. The diagnostic assessment between methods revealed that laryngeal aspiration of liquids had high specificity and a good positive predictive value, which means that this test can diagnose true negatives and predict whether or not an infant will actually aspirate. The sensitivity and positive predictive values for laryngeal aspiration of the puree consistency could not be calculated due to the lack of such findings during FEES.
The pharyngeal residue parameter showed good sensitivity and negative predictive value for Observer 1. This finding is an important predictor of laryngeal penetration and aspiration. According to the diagnostic assessment results, specificity was much higher than sensitivity, as described in the literature.
It is common knowledge that due to the small number of patients assessed, the results for predictive values should be viewed with caution. The accuracy of predictive value estimates depends on the prevalence of the disease and should take the small sample size (n = 30) into account.
Most studies were performed in adult patients with cerebrovascular accident sequelae, head and neck surgeries, and degenerative diseases, among others. FEES is known to be more easily performed in adults than in pediatric patients, because the latter are less tolerant of discomfort and more frequently haunted by fear during the examination.
We believe that by increasing the patient population of this study, possible misinterpretations could be overcome.
Conclusions
Despite different literature findings and although only one study has been performed in infants, FEES may be used as a complement to VFSS or as an alternative when the latter is not possible, because it can provide reproducible predictive results concerning tracheobronchial aspiration and pneumonia, that is, laryngeal penetration and aspiration. A further study with a larger sample is needed to confirm the results and to solve the remaining doubts concerning the validity of FEES in the pediatric population.