
Abstract
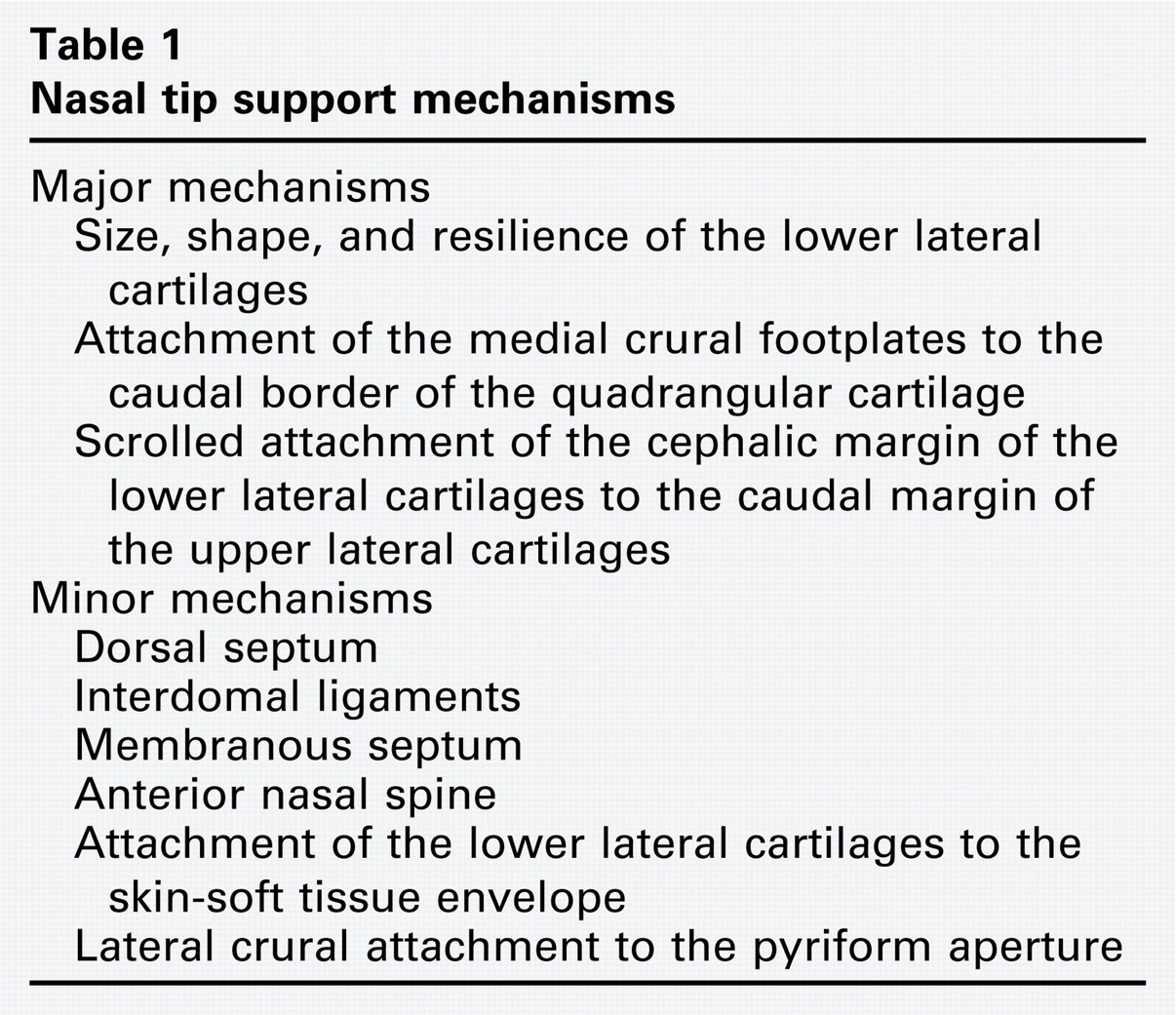
The support of the nasal tip is dependent on the interaction between cartilage, ligaments/fibrous junctions, and other tissues of the nose. According to Tardy, 1 the support of the nasal tip is provided by major and minor mechanisms (Table 1). These theoretical concepts were determined by clinical experience and are currently accepted by many rhinoplastic surgeons. 2 , 3 However, there are doubts about the existence of the medial crural footplate attachment to the caudal border of the quadrangular cartilage (one of the major mechanisms) because its anatomical description is not consistent, 4 and its sectioning on cadavers did not produce loosening of the nasal tip. 5 Furthermore, its histological existence was not proven in Asian cadavers. 6 As the result of these facts, some authors have considered that this mechanism does not exist or is of minor importance. 5 - 7
Nasal tip support mechanisms
Through a series of procedures in septoplasty surgery, the quadrangular cartilage undergoes straightening to achieve nasal permeability. 8 , 9 In some anterior septal deviations, an approach to the nasal septum requires a transfixion incision; 9 however, this incision interrupts the attachment of the medial crural footplates to the quadrangular cartilage and, if this attachment is a major mechanism of the nasal tip support, we could expect a loosening of the nasal tip in the postoperative period. To determine whether surgical section of attachment of the medial crural footplates to the quadrangular cartilage produces loosening of the nasal tip, we conducted a prospective observational study.
Methods
Study Design and Setting
A prospective, observational before-and-after study was conducted at the Hospital Universitario Clínica San Rafael, a tertiary referral center in Bogotá, Colombia. The study began on February 1, 2007, and ended on January 31, 2009.
Subjects
Patients undergoing septoplasty who required a transfixion incision because of anterior septal deviation with luxation/subluxation of the caudal septum were included. Patients without luxation/subluxation of the caudal septum, those undergoing septorhinoplasty, those with previous nasal surgery, and subjects who declined to participate in the study were excluded. Subjects were first briefed regarding the study's purpose and were then invited to participate in the study. Institutional approval by the Clinical Research Committee of the Hospital Universitario Clínica San Rafael was granted before beginning the study.
Outcome Measures
Preoperative and sixth-month postoperative assessment of the nasal tip support was performed. Measures of support of the nasal tip included a subjective evaluation, two measures of tip projection, and two measures of tip rotation. The subjective evaluation was performed through an ordinal scale (one to five, greater to lesser) by the use of fingertip depression to test tip recoil. 2
The nasofacial angle (NFaA) and the Goode ratio (GR) were used to evaluate the nasal tip projection, 10 and nasal tip rotation was evaluated by use of the nasolabial angle (NLA) and the tip rotation angle (TRA). 10 , 11 These measures were calculated on right lateral view digital photographs that were taken with a standardized photography protocol 12 and aided by utilities found in Corel Draw Software (Corel Graphics Suite v. 13, Inc., Ottawa, Ontario, Canada) (Fig 1).
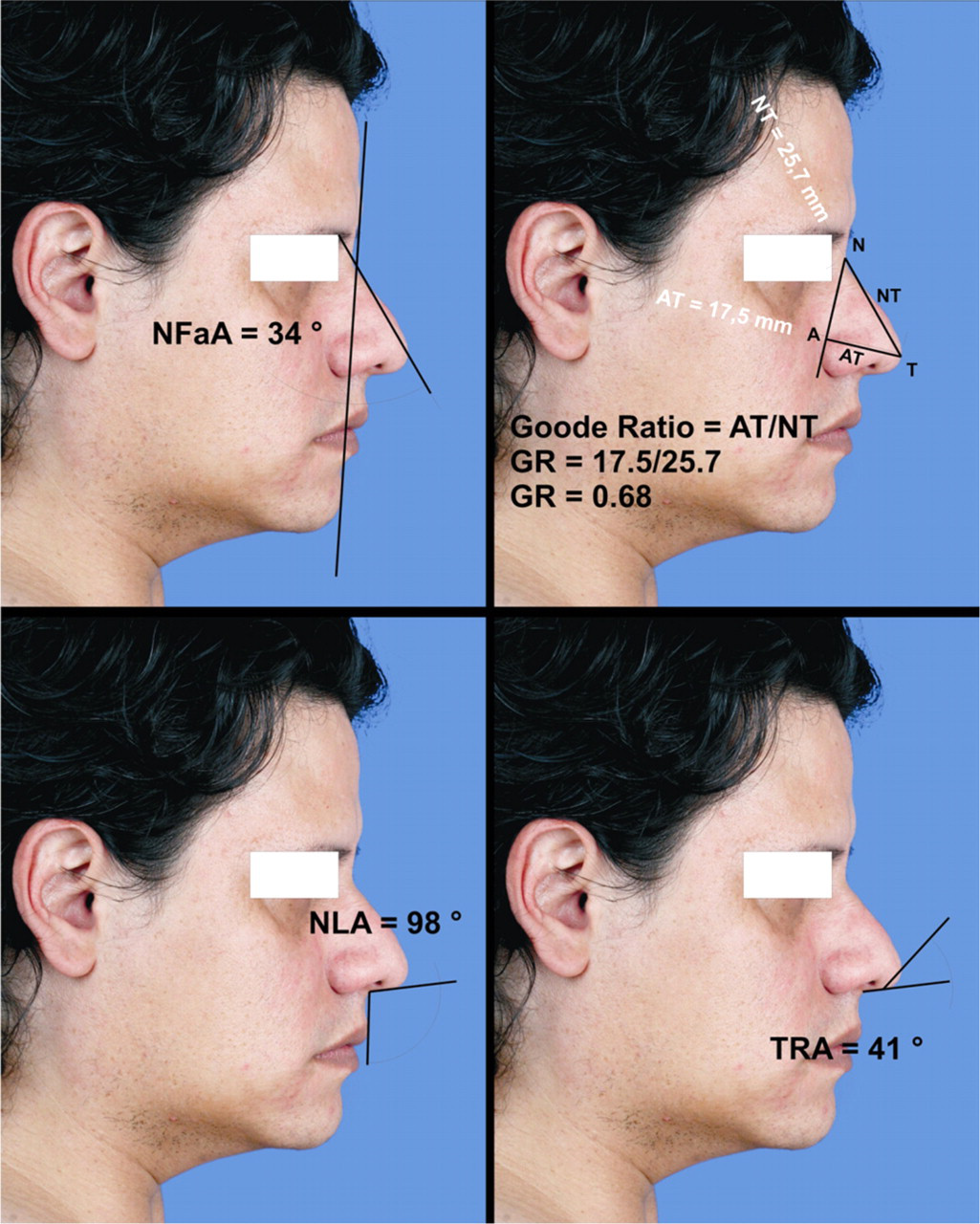
Measures of the nasal tip support. The NFaA was measured at the intercept of the glabella to the pogonion line with the nasion-to-tip line. The GR was calculated by dividing the distance from the alar point to the tip by the distance from the nasion to the tip. The NLA was measured at the intercept of the columellar point to the subnasale line with the subnasale to the labrale superius line. The TRA was measured at the intercept of the tip to the columellar point line with a line tangent to the columella. A, alar groove; T, nasal tip; N, nasion; NFaA, nasofacial angle; GR, Goode ratio; NLA, nasolabial angle; TRA, tip rotation angle.
The measures were performed in the preoperative period and six months postoperatively (±1 month) by the first author (L.E.O.). Two copies of the database were created, one for preoperative and one for postoperative measures, so as to not be biased by the preoperative results during the postoperative evaluation. Once the study finished, we joined the two databases to analyze the information.
Additionally, intraoperative photographs were taken with the patient anesthetized, the surgical field dressed, and the patient in supine position, leaving free the upper lip of the endotracheal tube fixation. The photographs were taken in the right lateral view, the camera 1 meter away but without the recommended standard lighting conditions. 12 In this situation, two photographs were taken, one before the transfixion incision and another after it, and GR and TRA were measured. Additionally, the tip recoil test was performed before and after the transfixion incision. In these patients, an infiltration with lidocaine 1 percent with 1:100.000 epinephrine was made after making the incision so as not to distort the nasolabial junction. The NFaA was not measured in this situation because the glabella and pogonion were not visible, as they were hidden by surgical drapes. The NLA also was not measured because the upper lip is not in a standard position. Two copies of the database were also created, one for preincision and one for postincision measures. For a racial description of patients included in this study, an assessment of the skin phototype was made. 13
Surgical Procedure
The surgical procedures were performed by the first author by use of the same surgical principles in all cases. 2 In brief, a full transfixion incision was made, and the mucoperichondrial/mucoperiosteal flap was elevated on the side of anterior concavity (Fig 2). An inferior 2- to 3-mm strip of quadrangular cartilage was excised above the maxillary crest, producing a “swinging door.” After crossing the bony cartilaginous junction, contralateral tunnels were elevated, and posterior deviations were removed. The caudal septum was released from the anterior nasal spine, and a progressive resection of its inferior border was made until it fit into the space of the nose. The caudal septum was then sutured to the periosteum of the anterior nasal spine with chromic catgut 4-0. After that, on the side of the anterior concavity, parallel vertical and horizontal full-thickness incisions were made to the cartilage in the area II of Cottle, producing a cross-hatching of the caudal septum. 2 , 14 The transfixion incision was closed by the use of two interrupted 4-0 chromic catgut sutures on each side. Nasal splints, secured with a single 2-0 silk mattress suture, and anterior nasal packing (gauze pad coated with antibiotic ointment) were used in all patients. Nasal packing was removed three to five days postoperatively and nasal splints between five and 14 days.
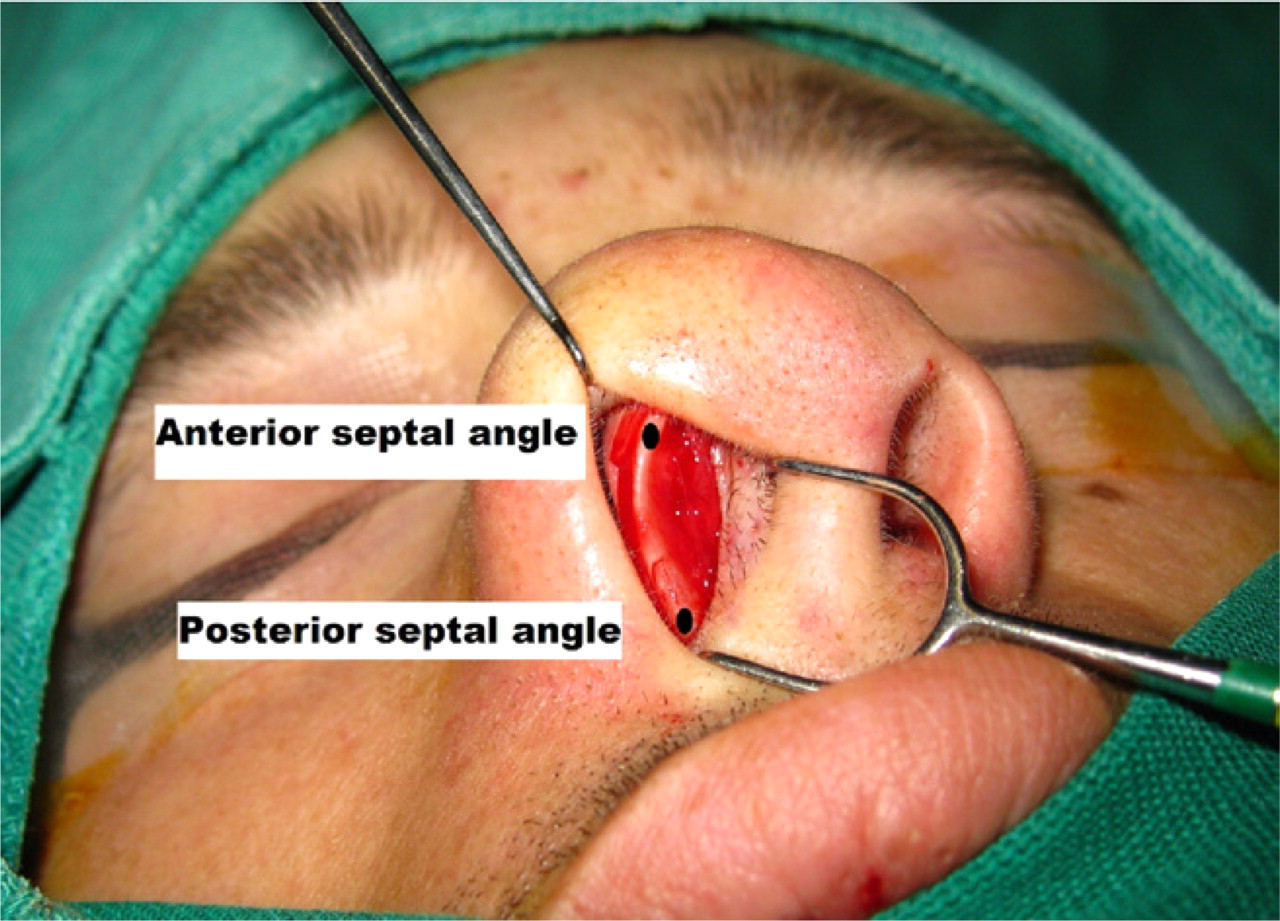
Transfixion incision. This incision extends from the anterior septal angle to the posterior septal angle, allowing an adequate approach to correct anterior septal deviations with luxation/subluxation of the caudal septum.
Power Analysis
The power of this study to determine whether the differences found really do exist for each variable was determined to be: NFaA = 0.45, GR = 0.37, NLA = 0.23, and TRA = 0.38. For this analysis of the power, the values of the difference in means (δ) and the standard deviation of difference (σ) were taken from the results of this study, Type I error (α) was set at 0.05, and the number of pairs (n) was 27. Power analyses were performed by the use of PS software (v.3.0; DuPont WD, Plummer WD, Vanderbilt University, Nashville, TN).
Statistics
The Kolmogorov-Smirnov test of normality was performed, and for normally distributed variables, parametric tests were used. Otherwise, nonparametric tests were applied with the assumption of ordinal variables. Differences among groups were searched for and considered to be statistically significant if P < 0.05. The main results were postoperative versus preoperative comparative analysis of measures of nasal tip support. Statistical analyses were performed with the use of SPSS version 11.5 (SPSS, Inc., Chicago, IL).
Results
This study took place in the otolaryngology department of the Hospital Universitario Clínica San Rafael between February 1, 2007, and January 31, 2009. Of the 39 cases included, 27 cases completed the follow-up, and their results are presented as main analysis. Of the remaining 12 cases, two were excluded because they did not want to participate in the study and 10 because they did not complete follow-up evaluations.
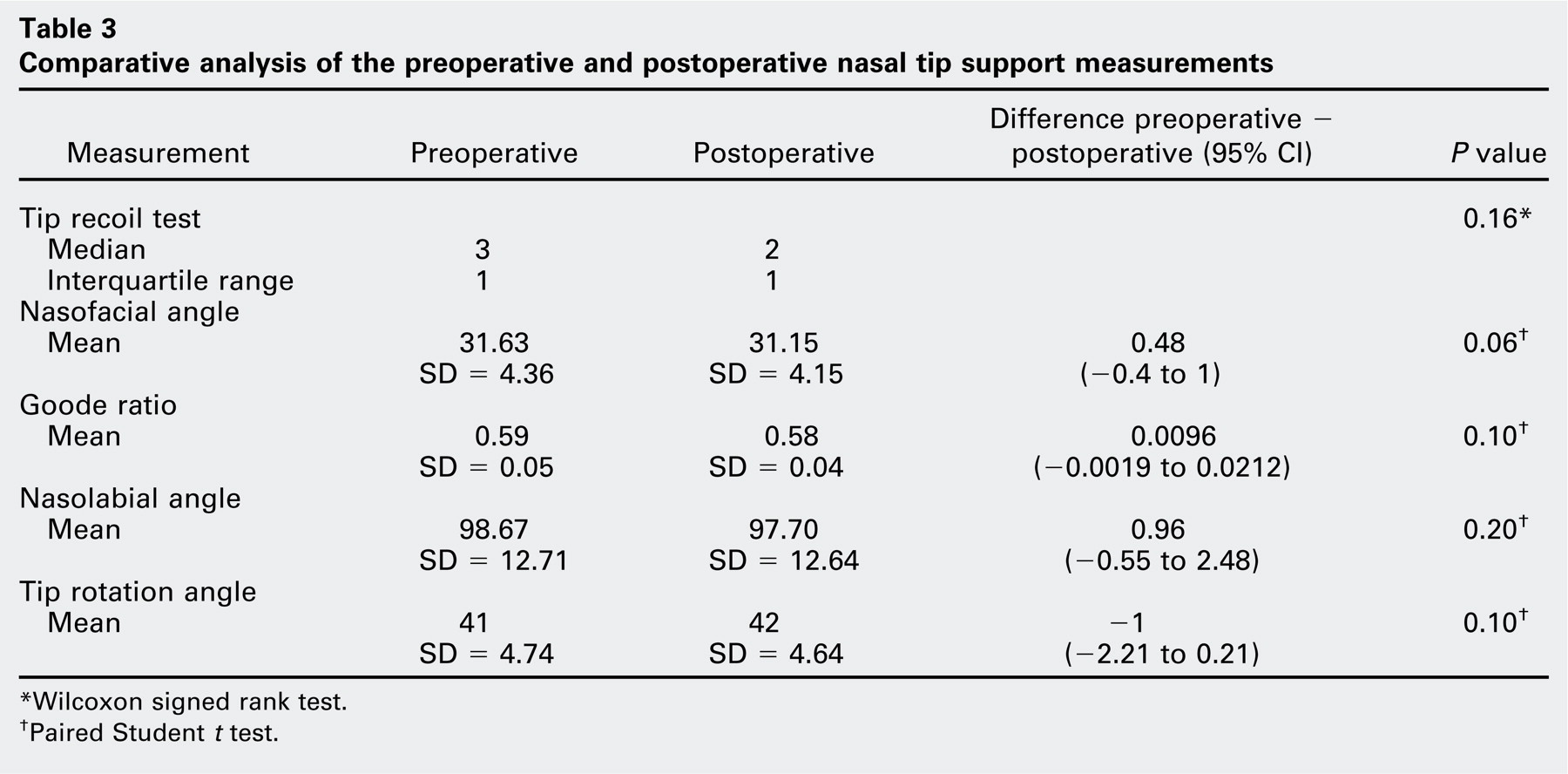
Table 2 shows the general characteristics of the study subjects, demonstrating an even distribution by sex, as well as most patients having skin phototype III or IV (96%), which is characteristic of the Hispanic population. The results of the preoperative and postoperative measurements are presented in Table 3. Because the preoperative and postoperative measurements of the NLA, TRA, GR, and NFaA were normally distributed (Kolmogorov-Smirnov test, P > 0.05), these were assumed to be proportional variables. Postoperative values for the NFaA, GR, and NLA were less than those for the preoperative ones, whereas the postoperative value for TRA was greater. None of these differences were statistically significant.
Comparative analysis of the preoperative and postoperative nasal tip support measurements
Wilcoxon signed rank test.
Paired Student t test.
Baseline of study population
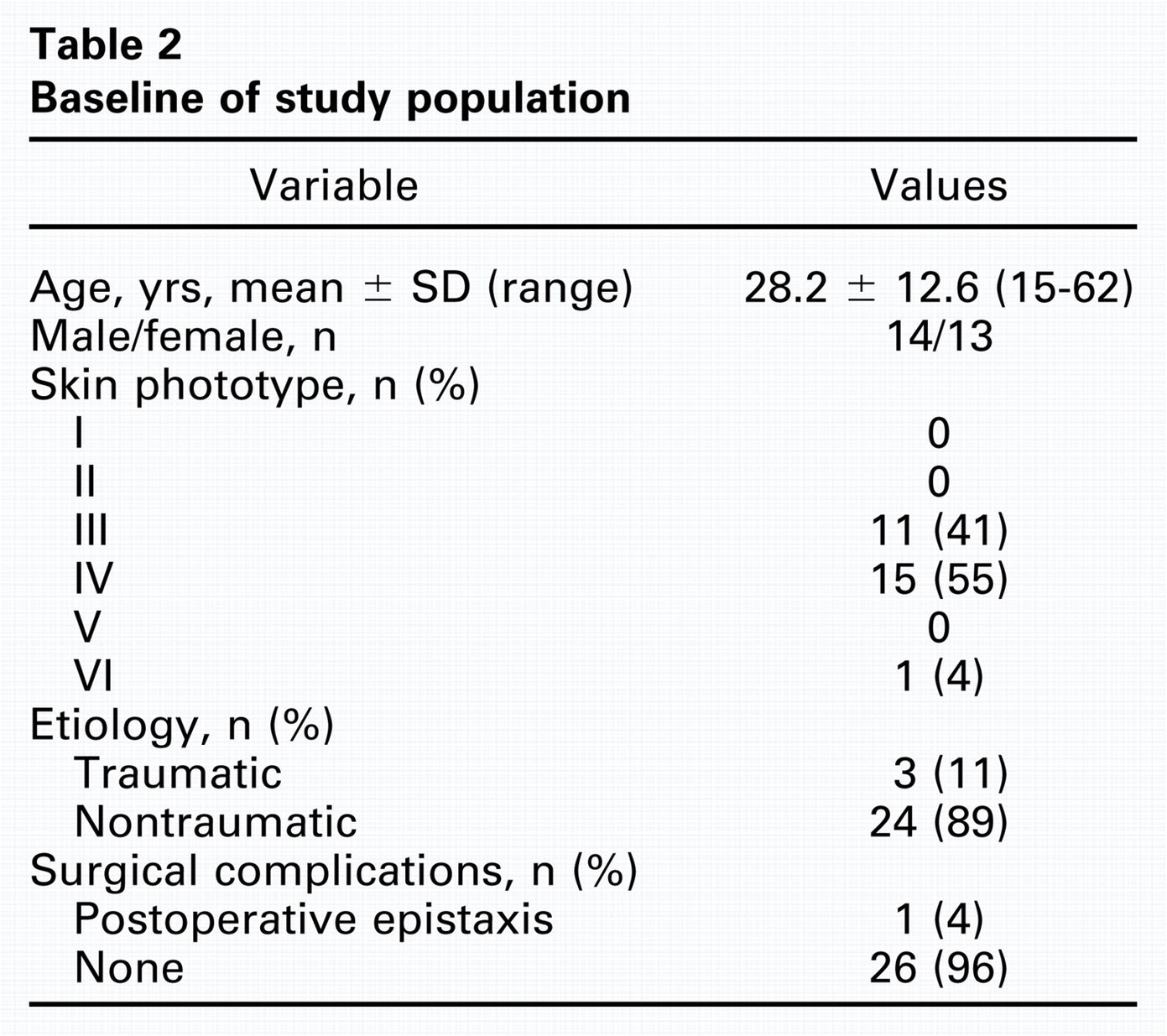
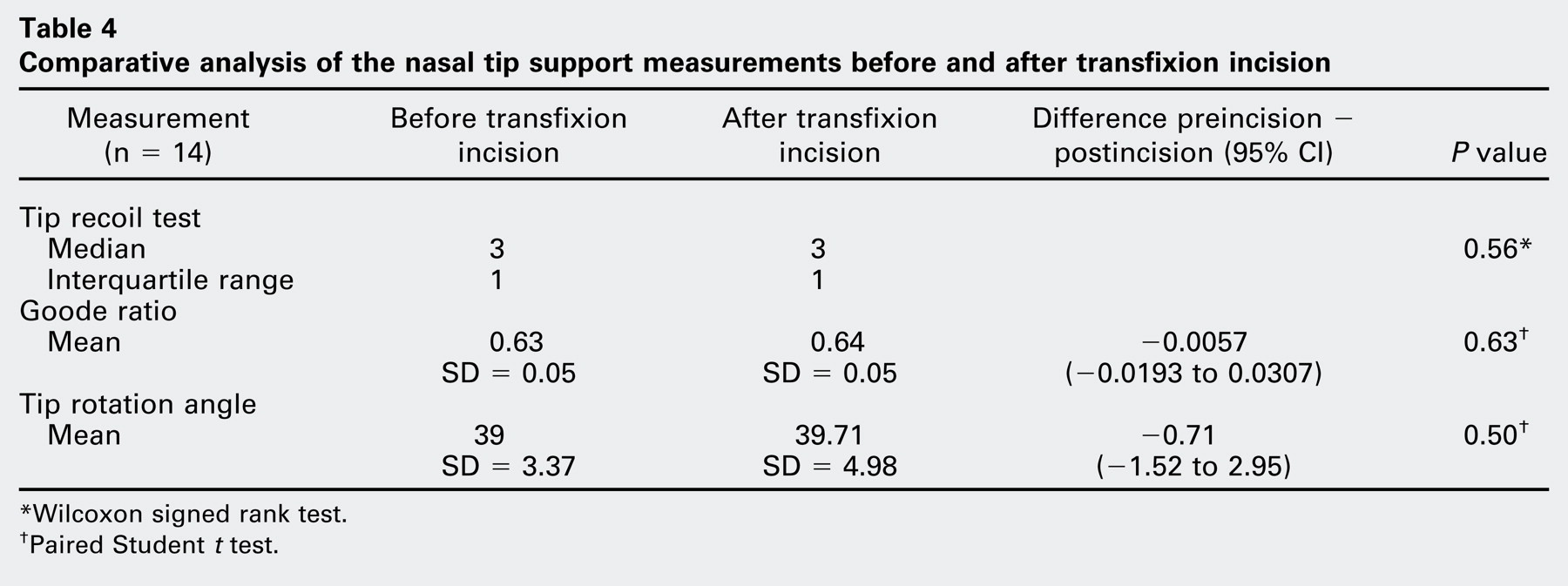
Table 4 presents the measurements before and after the transfixion incision. This comparison was made among the 14 patients for whom this information was available. There were seven men and seven women with average age of 29 years (SD = 14.3 years). Seven patients had skin phototype III, and seven had skin phototype IV. There were no statistically significant differences between measurements before and after the transfixion incision (P > 0.05).
Comparative analysis of the nasal tip support measurements before and after transfixion incision
Wilcoxon signed rank test.
Paired Student t test.
Discussion
The nasal tip is held in position by a complex set of anatomical structures and relationships. Tardy classified these mechanisms into major and minor (Table 1), and many surgeons embrace this theoretical concept and take it into account when performing nasal surgery. 1 - 3 For example, technical changes have been proposed in rhinoplasty surgery to avoid surgical disruption of the nasal septum to columella attachment by the use of an incision that has been called the “transseptal transfixion incision.” 15
One of the major mechanisms of the tip support is the attachment of the medial crural footplates to the caudal border of the quadrangular cartilage; however, several concepts argue against this concept. First, the nasal septum to columella attachment is not referred to as a ligament or other fibrous union in contemporary anatomy textbooks 4 because the septocolumellar ligament was not found in a cadaver dissection study of white origin, 16 or it was found only as a loose union. 17 Second, in a study aimed to characterize histologically the mechanisms of the nasal tip support, Han et al 6 describe that “no such remarkable supporting structures were found at this point.” Although this study was performed on Korean cadavers, their results are consistent with some descriptions made for white people. 16 , 17 Moreover, in this study, they confirmed the presence of ligamentous attachments between the upper lateral cartilage (ULC) and the lateral crus and fibromuscular attachments between the lateral crus and the pyriform aperture. 6 Third, in a study that objectively evaluated the nasal tip support, Beaty et al 5 found no effect after the transfixion incision in fresh cadavers. The authors of this study used a device specifically designed to objectively measure the support of the nasal tip (Beaty Tensegrometer; G.M. Tooling, Chamblee, GA), and on the basis of intraoperative and cadaver measurements they reported other interesting findings, including: 1) The open approach to rhinoplasty is less damaging to nasal tip support than the closed approach. 2) Marginal and transfixion incisions have no significant effect on nasal tip support. 3) Placement of an intercartilaginous incision produces a 25 percent loss in tip support. 4) Delivery of the lower lateral cartilage (LLC) completes the division of the ligamentous binding between the domes and medial crura and further weakens the nasal tip, for a total of 35 percent loss in tip support. 5) Resection of portions of the LLCs has no significant effect on nasal tip support until 80 percent of the cartilage has been excised.
Before discussing our results, we must mention some important limitations at the time of interpretation. First, our sample is one of convenience, and its size (n = 27) has a low power to determine whether the absence of differences in the present study is caused by a type II error or whether there is unquestionably no differences between the preoperative and postoperative measurements (power < 0.50 for all variables). The loss of 12 of the 39 patients in the initial cohort reduced the size of our sample considerably, with a subsequent negative impact on the statistical power. The sample sizes needed to establish whether the differences found are statistically significant or not (which are differences of around 1%-2%), with a power = 0.8, should be NFaA = 60, GR = 74, NLA = 115, and TRA = 77. Therefore, the present study should be considered preliminary, and its results should be confirmed by larger studies.
Another limitation is that all assessments were made by the surgeon. Although this makes the study completely nonblind (it was made with two separate databases for measuring preoperative and postoperative values, which helps to partially control this potential bias), it is also true that it can increase stability in the measurements and thereby strengthen the internal validity of the study. Finally, we made a short-term follow-up study and additional studies are necessary, with a longer follow-up period to determine whether long-term changes occur in the nasal tip support that may be attributable to transfixion incision.
Our study evaluated the effects of surgical section of the nasal septum to columella attachment, performed through a transfixion incision during conventional septal surgery. This is a situation in which we can see “in vivo” the specific effect of this incision on the nasal tip support because other relevant structures remain unchanged (maybe with the exception of quadrangular cartilage, which was resected at its inferior border and was cross-hatched at its caudal portion). To assess the nasal tip support, we chose measurements that are widely accepted by facial plastic surgeons (tip recoil test, NLA, TRA, GR, and NFaA). 1 , 2 , 10 , 11 One might expect that if the nasal septum to columella attachment is a major mechanism for nasal tip support, its surgical section would cause measurable changes. However, this preliminary study showed that such changes do not occur in measurements taken six months after surgery (tip recoil test, GR, NFaA, NSL, TRA) nor in those made in surgery after a transfixion incision (tip recoil test, GR, TRA). These results are consistent with the absence of a strong union, such as a ligament or similar structure, between the caudal nasal septum to footplates of the medial crura, and it coincides with the results of previous studies. 5 , 6 , 16 , 17
An arguable point is whether the results of this study can be generalized to other racial groups because patients in this study are Hispanic (Table 1). As we mentioned previously, for the white population, there are macroscopic studies that failed to demonstrate a strong bond between the caudal nasal septum to footplates of the medial crura, 16 , 17 and a study in which it was sectioned and there were no measurable changes in the support of the nasal tip. 5 Even more clearly, for Asian subjects, in a histological study the authors found that this attachment is not a ligament or other strong bond. 6 In analyzing the results of previous studies 5 , 6 , 16 , 17 and ours, it is reasonable to suggest that the attachment of the caudal nasal septum to footplates of the medial crura is not an important support mechanism for the nasal tip, and is, at best, a minor tip support mechanism. This observation seems to be multiracial.
The question is, what are the major support mechanisms of the nasal tip? As shown by anatomical studies, 16 , 17 a histological one, 6 as well as by objective measures of nasal tip support, 5 the scrolled attachment of the LLCs and upper lateral cartilages is certainly one of them. Similarly, the size, shape, and resilience of the LLCs are integral aspects to the nasal tip support. 5 A structure that has been called the “intercrural ligament” (ligamentous attachments among the lateral, dome, and medial crura) appears to play an important role in this regard. This was the structure whose disruption caused the greatest loss of nasal tip support and whose reconstruction led to a significant gain above baseline. 5 With this argument, Dyer 7 offers a conception of nasal surgery that emphasizes the reconstruction of the “intercrural ligament” through sutures that bind together LLC, as the main mechanism to achieve “architectural stability to resist postoperative scar contracture,” thereby achieving stable results over the long term.
In conclusion, in this preliminary cohort of Hispanic patients, we find that the surgical section of the attachment of the medial crural footplates to the caudal margin of the quadrangular cartilage does not produce significant changes in nasal tip support, supporting the hypothesis that this is not a major mechanism for nasal tip support. However, additional studies are needed, with larger sample sizes and different racial groups, in order to corroborate these findings.
Author Contributions
Disclosures
Acknowledgments
The authors thank Dr. Robert Samuels Halphen, otolaryngologist, for his valuable review of the English version of the manuscript; Dr. Jorge Espinosa-Reyes, otolaryngologist-facial plastic surgeon, for his comments on the manuscript; and Dr. Piedad Peñaranda, dermatologist, for her help in classifying the skin phototype of the patients.