
Abstract
OBJECTIVE
The development of new techniques for transoral resection has led to a renewed interest in primary surgical treatment of oropharyngeal squamous cell cancer (SCCA). We reviewed our experience with primary surgery for oropharyngeal SCCA to identify factors associated with survival.
STUDY DESIGN
Case series with chart review.
SETTING
Tertiary medical center.
SUBJECTS AND METHODS
Patients who underwent primary surgical treatment of oropharyngeal SCCA from 1985 to 2002 were analyzed. Patients who failed nonoperative treatment or had distant metastases at presentation were excluded.
RESULTS
A total of 105 patients met study criteria. The majority of patients (91%) had advanced stage disease (III/IV). All patients received postoperative radiation; chemotherapy was used in eight patients. Five-year disease-free survival was 83 percent for stage I, 67 percent for stage II, 56 percent for stage III, and 43 percent for stage IV disease. Crude local control rates were 94 percent for T1 disease, 90 percent for T2 disease, 81 percent for T3 disease, and 80 percent for T4 disease; crude regional control rates were 100 percent for N0 disease, 90 percent for N1 disease, 84 percent for N2 disease, and 82 percent for N3 disease. Cox proportional hazards models revealed that nodal stage (hazard ratio [HR] 2.3, P = 0.02) and black race (HR 2.6, P = 0.004) were the only significant predictors of disease-free survival.
The traditional management of oropharyngeal squamous cell cancer (SCCA) has consisted of surgery, followed by postoperative radiation therapy for advanced primary site or nodal disease, which results in superior survival and locoregional disease control compared with radiotherapy alone, but results in poorer functional outcomes than a nonoperative approach.1 The success of organ preservation protocols in laryngeal SCCA has resulted in an increase in the use of primary chemoradiation (CRT) in oropharyngeal SCCA, despite a paucity of randomized controlled clinical trial data comparing primary surgical approaches to organ preservation. Many oropharyngeal tumors are increasingly recognized as being related to human papillomavirus (HPV) infection; these have a more favorable outcome and a more favorable response to nonoperative treatment.2 However, the high surgical salvage success rates described following failed organ preservation for laryngeal cancer are not applicable to oropharyngeal tumors, with salvage successful in fewer than one-third of patients. 3 – 7
The optimal choice of initial treatment for oropharyngeal SCCA is a source of renewed debate among head and neck surgeons, particularly with the development of new transoral techniques that allow primary resection of some tonsil and tongue base tumors with reduced surgical morbidity. CRT is associated with an increase in late toxicities from the addition of chemotherapy, and a primary surgical approach may allow deintensification of postoperative adjuvant therapy through the use of histologic information to guide the use of radiation and chemotherapy. 8 – 12 In light of the renewed interest in primary surgery for oropharyngeal tumors, we reviewed our experience with primary surgery for oropharyngeal SCCA to identify factors associated with survival.
Materials and Methods
The medical records of all patients evaluated for oropharyngeal SCCA at the Medical College of Georgia from 1985 to 2002 were reviewed in compliance with the Health Insurance Portability and Accountability Act. Patients with a history of prior treatment for head and neck cancer, known distant metastatic disease, nonsquamous neoplasms, those who did not complete treatment, and those without follow-up were excluded.
Primary surgical therapy included wide local excision; radical tonsillectomy; partial palatectomy; partial, subtotal, or total glossectomy; partial, total, or extended total laryngectomy; and composite resection including mandibulectomy. Elective neck dissection was performed for clinically node-negative patients at risk for nodal metastases with removal of levels I through IV on the ipsilateral side for advanced primary stage tumors and bilateral elective neck dissection for primary tumors involving the midline. Modified radical neck dissection was performed for clinically positive nodal disease. Postoperative radiation was administered for three or more pathologically involved nodes, involvement of multiple levels, extracapsular spread, adverse pathologic primary site features including perineural invasion or lymphovascular invasion, and advanced stage (III or IV) disease. Postoperative CRT, consisting of cisplatin with 5-fluorouracil, was used in selected patients with advanced stage disease (III/IV) and adverse histologic features (extracapsular spread or lymphovascular invasion).
Statistical analysis was performed with Kaplan-Meier survival analysis using Prism 5.0 (GraphPad Software, San Diego, CA) and Stata 10 (StataCorp, College Station, TX) for proportional hazards models. Cox proportional hazards models were used to analyze the effects of multiple risk factors that could influence disease-specific survival, including testing for significant interactions between variables. Variables that were hypothesized to have predictive value as well as those that were significant in bivariate analysis were entered into the regression models. Collinearity was checked by performing a Cox proportional hazards analysis, calculating the variance inflation factors (VIF), and removing variables with a VIF > 10.0, which suggests collinearity. Models were sequentially built in order to identify variables that were significantly associated with survival, and stepwise variable selection was used to determine which subset of variables was predictive of the outcome of interest. Akaike's information criterion was used to select models by goodness of fit. Significance was attributed to a P value ≤ 0.05. This protocol was reviewed and approved by the Medical College of Georgia Institutional Review Board.
Results
A total of 105 patients met inclusion criteria with a mean follow-up time of 34 months (Table 1). The majority of patients were white (69%), male (73%), smokers (80%), and had a history of alcohol abuse (69%). The mean age was 53 years (range, 28–81 years). The tonsil represented the most common primary site (55%), followed by the base of the tongue (35%). Advanced primary site disease (T3 or T4) was present in the majority of patients (64%), as was advanced (III/IV) tumor-nodes-metastasis (TNM) stage (91%) (Table 2). Advanced comorbidity was present in 38 percent, and only 18 percent of patients had private insurance. All patients received postoperative radiation, with a mean dose of 5019 Gy (range, 4500–7140 Gy). Postoperative CRT was used in eight (8%) patients.
Five-year disease-free survival (DFS) rates were 83 percent for stage I, 67 percent for stage II, 56 percent for stage III, and 43 percent for stage IV disease (Fig 1). Nodal status was significantly associated with five-year DFS (P = 0.02) (Fig 2). The presence or absence of extracapsular spread was commented on in 48 patients (46%), with extracapsular spread present in 50 percent. The presence of extracapsular spread was associated with a 33 percent five-year survival rate, while nodal disease without extracapsular spread was associated with a 64 percent five-year survival rate (Fig 3). Recurrent disease developed in 37 patients (35%), with local recurrence in 16 patients, regional recurrence in 12 patients, and distant failure in nine patients. Crude local control rates were 94 percent for T1 disease, 90 percent for T2 disease, 81 percent for T3 disease, and 80 percent for T4 disease. Crude regional control rates were 100 percent for N0 disease, 90 percent for N1 disease, 84 percent for N2 disease, and 82 percent for N3 disease. The five-year locoregional control rate was 60 percent (Fig 4).
Population characteristics
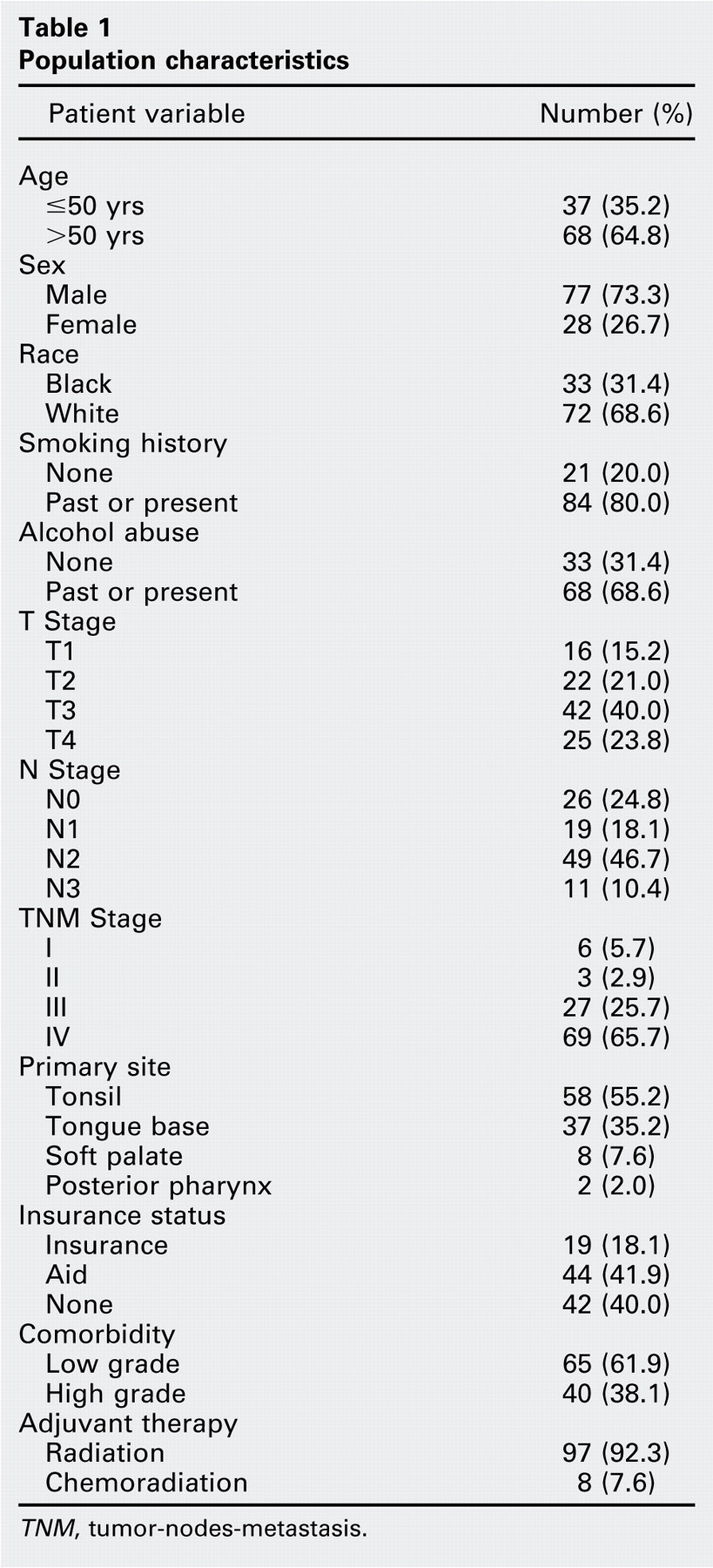
TNM, tumor-nodes-metastasis.
Stage distribution
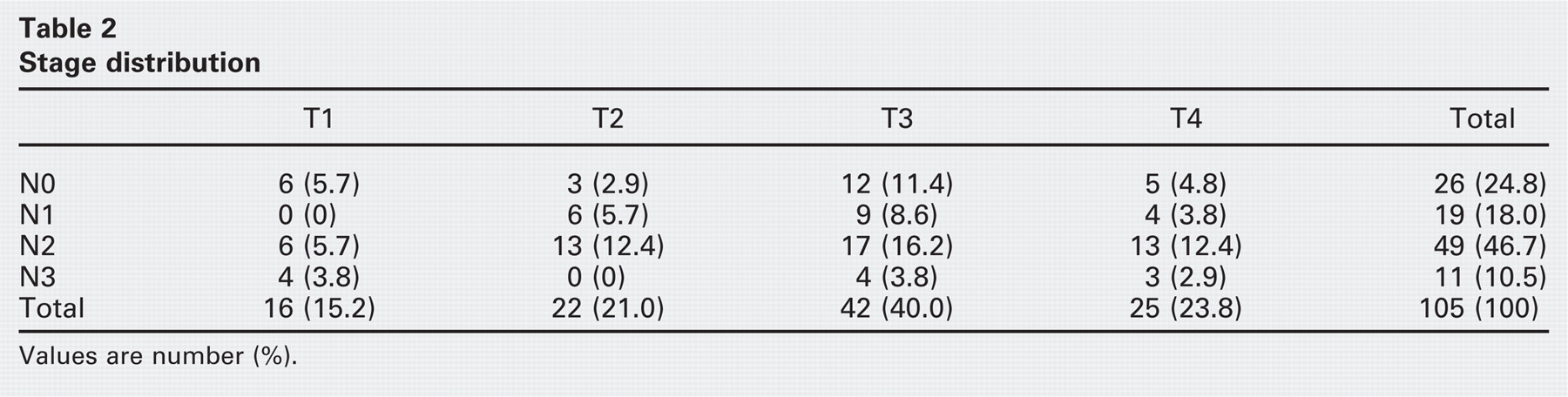
Values are number (%).
Cox proportional hazards models were used to analyze the effects of multiple risk factors that could influence disease-specific survival, including interactions between race and payor status. TNM stage, T stage, nodal stage, and comorbidity were modeled as categorical variables based on status as early or advanced stage (Table 3). The resulting hazard ratio (HR) indicates that advanced stage increased the hazard by the HR factor. On univariate analysis, nodal status and black race were associated with significantly decreased survival; insurance status showed an interaction with race, with significant differences in the HR between black and white patients without insurance. The effects of multiple simultaneous risk factors were further examined using multivariable logistic regression analysis after removing variables with high collinearity, using sequential model building and stepwise variable selection to identify variables that were significantly associated with DFS, after controlling for other variables. Only advanced nodal stage and black race were significant in the final model (Table 4).
Discussion
The results of this study show that primary surgical treatment of oropharyngeal SCCA is effective in achieving excellent locoregional control and permits deintensification of adjuvant therapy, even in patients with advanced stage disease. Nodal status and race were the primary determinants of disease-free survival. A major limitation to this work is the absence of information regarding functional outcomes and HPV status, which is unique to oropharyngeal SCCA and has been shown to impact the prognostic value of nodal disease and race.
The advantage of primary surgery in treating oropharyngeal SCCA is the potential to avoid radiation or CRT by identifying patients with favorable pathology who would not benefit from the addition of cytotoxic therapies. In patients with small (T1 or T2) primary site lesions and no nodal disease (N0), a surgical approach may permit withholding of postoperative radiation in 63 to 72 percent of patients 8 – 10 through identification of patients with favorable histology, and identifies a subset of patients who have improved salvage rates and improved survival.13 Primary surgery in patients with advanced stage disease allows deintensification of adjuvant therapy by identification of those patients who can be spared postoperative chemotherapy.8, 10 – 12 The advent of newer transoral resection techniques using the laser or surgical robot are associated with decreased rates of tracheostomy and feeding tube dependence, 12 – 16 although patients with advanced primary stage disease and preoperative swallowing dysfunction have a greater incidence of postoperative functional impairment.17
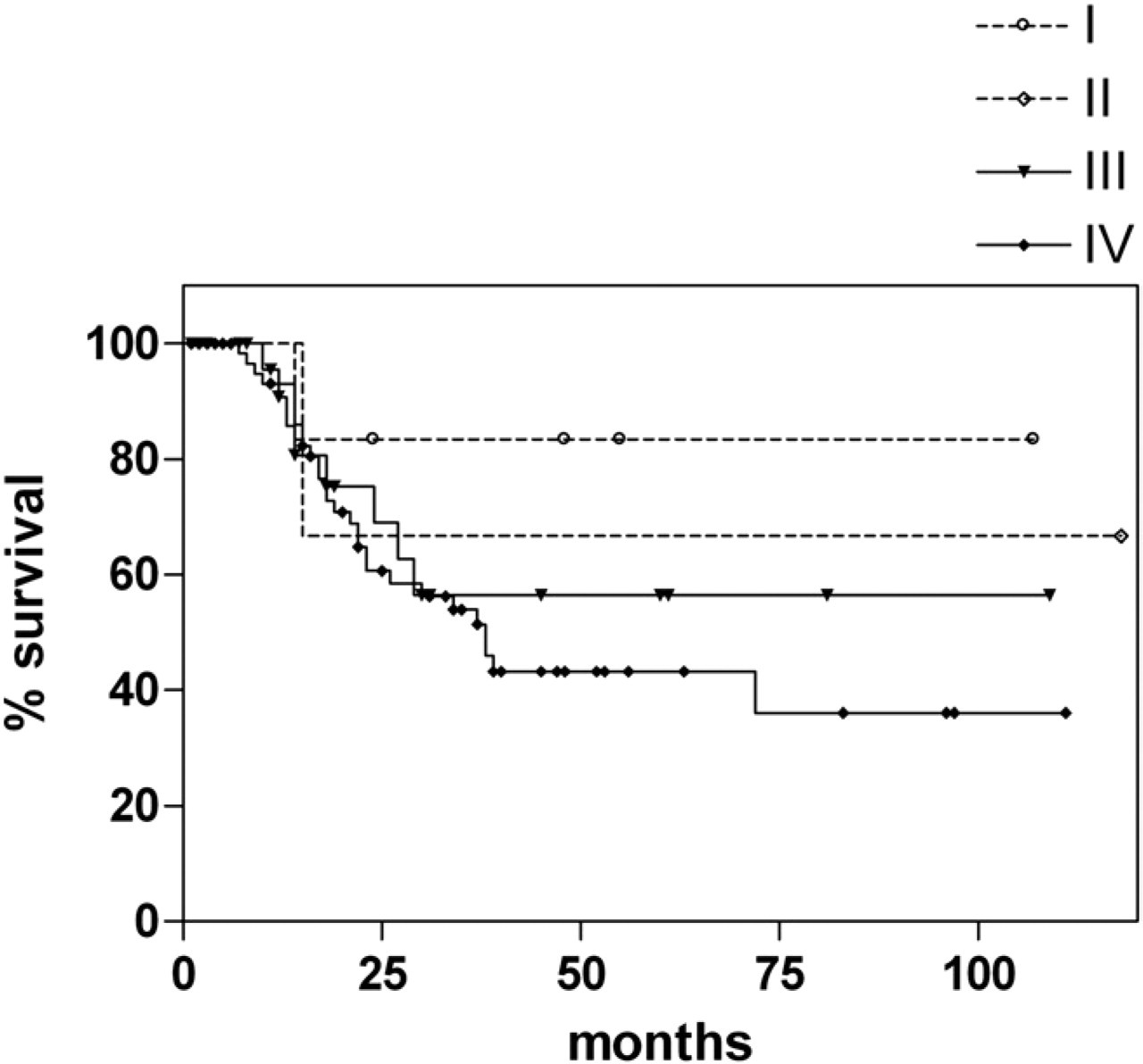
Disease-specific survival by stage.
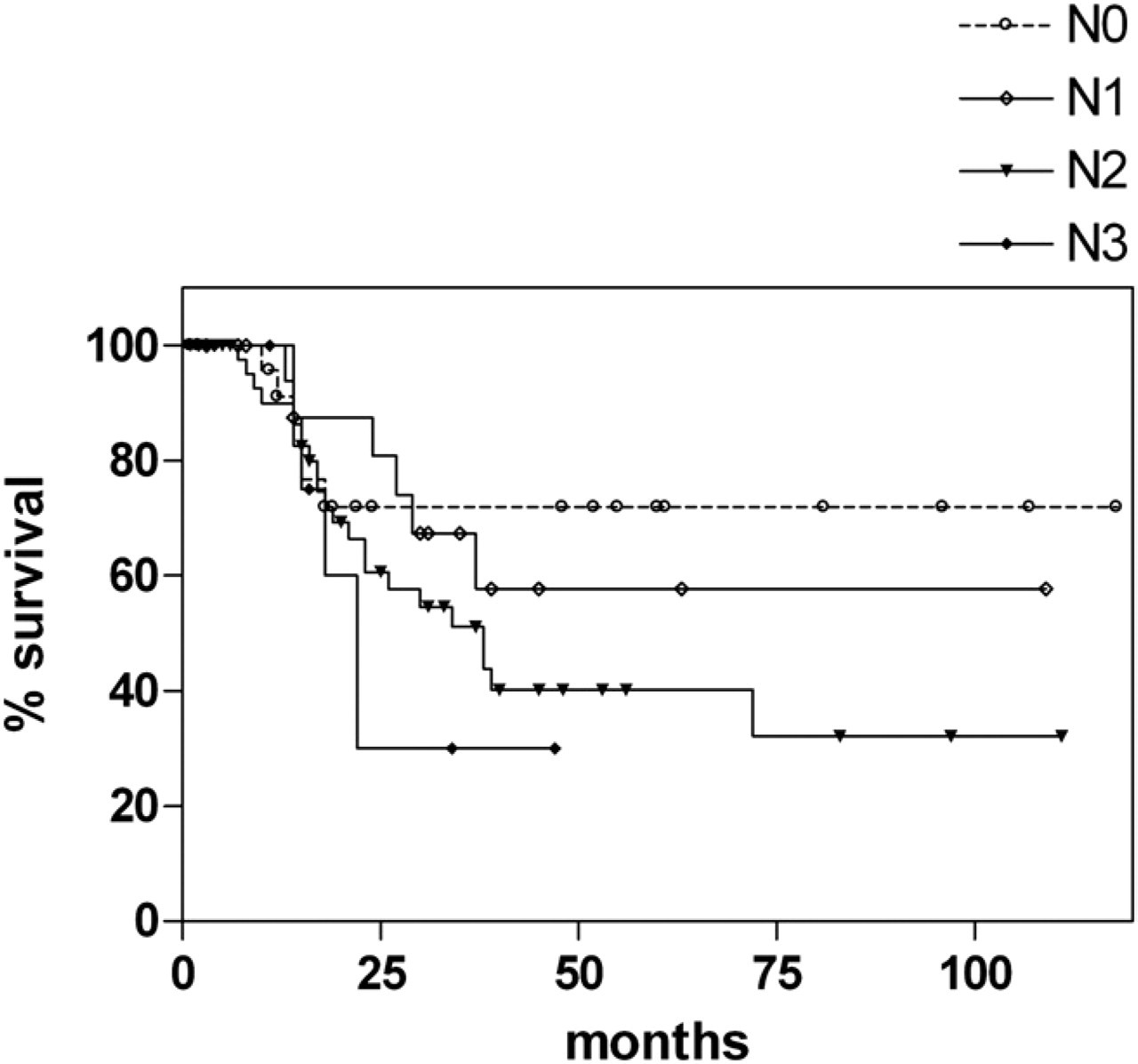
Disease-specific survival by nodal status.
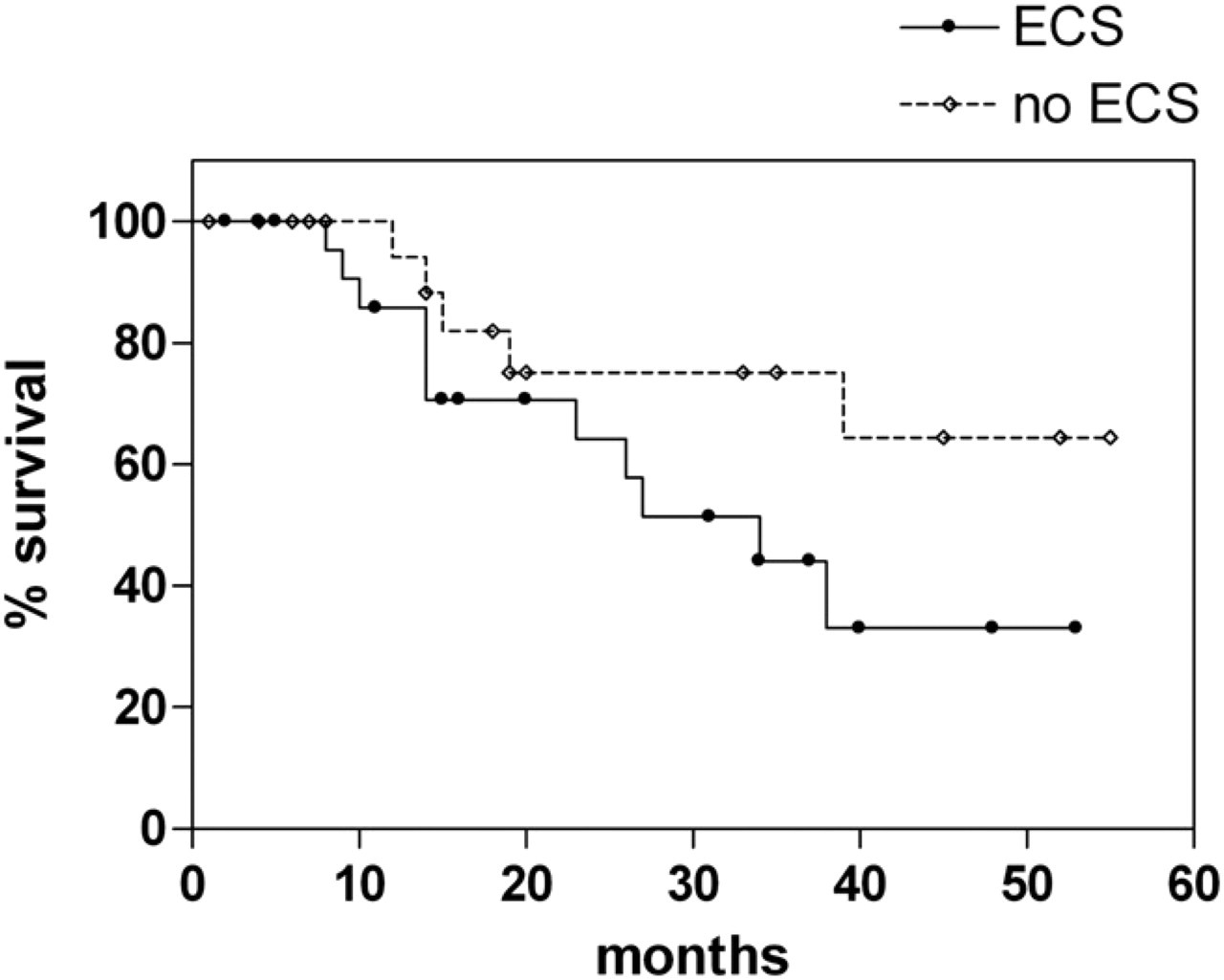
Effect of extracapsular spread (ECS) on disease-specific survival.
In the present study, advanced nodal disease and black race were associated with poorer survival. A significant limitation to this work is the absence of information regarding HPV status. HPV-positive tumors have been shown to have improved survival and disease control rates compared to HPV-negative tumors, and this survival benefit is independent of treatment modality.2, 18 – 21 Patients with HPV-positive tumors are more likely to present with smaller primary site disease and more advanced nodal disease.22, 23 Advanced nodal stage is a poor prognostic factor for HPV-negative tumors, but does not carry the same adverse prognosis in HPV-positive disease that it does for HPV-negative tumors.23, 24 The improved survival in HPV-positive disease has been attributed to increased radiosensitivity, but has been shown to be independent of treatment modality.2, 18, 20 Other factors such as a lower risk of distant disease and second primary cancers and an inverse correlation with adverse tumor biomarkers such as epidermal growth factor receptor, p53 mutations, and survivin, are equally plausible.2 Advanced primary site stage has been shown to be an independent risk factor for recurrence and survival after controlling for HPV status.25
The incidence of HPV positivity in oropharyngeal SCCA is ninefold greater for white patients than black patients.26 Racial differences in the outcome of oropharyngeal SCCA treatment have been attributed to racial differences in the prevalence of HPV-positive tumors. Black patients have been shown to have poorer survival following treatment for oropharyngeal cancer, and are significantly less likely to have HPV-positive tumors than white patients; in patients with HPV-negative tumors, survival is similar for black and white patients.26 We have previously shown that racial differences in head and neck SCCA outcomes were primarily related to differences in access to health care.27 However, in the present study, while racial differences existed between patients without insurance, only nodal status and race remained significant after controlling for all other variables. The current literature suggests that our results may be due to a low incidence of HPV-positive disease.
Future research must focus on delineating differences in patients with oropharyngeal cancer based on HPV status. The presence of a high proportion of HPV-positive patients confounds the interpretation of efficacy in novel regimens investigating both CRT and surgical treatment.12, 24, 28 The favorable impact of HPV on oropharyngeal SCCA outcomes is a relatively recent discovery and, to date, the majority of literature regarding oropharyngeal SCCA outcomes does not include HPV status in outcome analysis, including the present study. Patients with HPV-positive tumors appear to have a different disease, with improved locoregional control and survival despite a preponderance of advanced stage disease. This difference may be due to smaller primary site disease at presentation, or to differences in tumor biology conferred by HPV infection.
The success of surgical salvage following failure of non-operative treatment is poor. Recurrence is associated with reduced survival, and only a minority of patients are candidates for surgical salvage.5, 7 Following CRT, patients with advanced stage primary disease and those with regional recurrence have dismal salvage rates, and the majority of patients with recurrence develop a second recurrence in < 12 months.7, 29 Despite advances in surgical reconstruction, patients who require secondary free flap reconstruction in the setting of previous radiation have longer operative times, higher complication rates, and a greater requirement for postoperative tracheostomy.30 Patients with the greatest likelihood of salvage following CRT failure are those with early stage primary tumors and no recurrent nodal disease.7, 29 These data emphasize that successful locoregional control with initial therapy is a critical determinant of long-term survival. Patients with initial early stage disease who receive CRT have been shown to have an increased risk of second recurrences after salvage surgery,7 and CRT failure is associated with poorer survival even after controlling for other variables.5 These data suggest that chemotherapy may select for more aggressive tumor biology in a subset of patients.
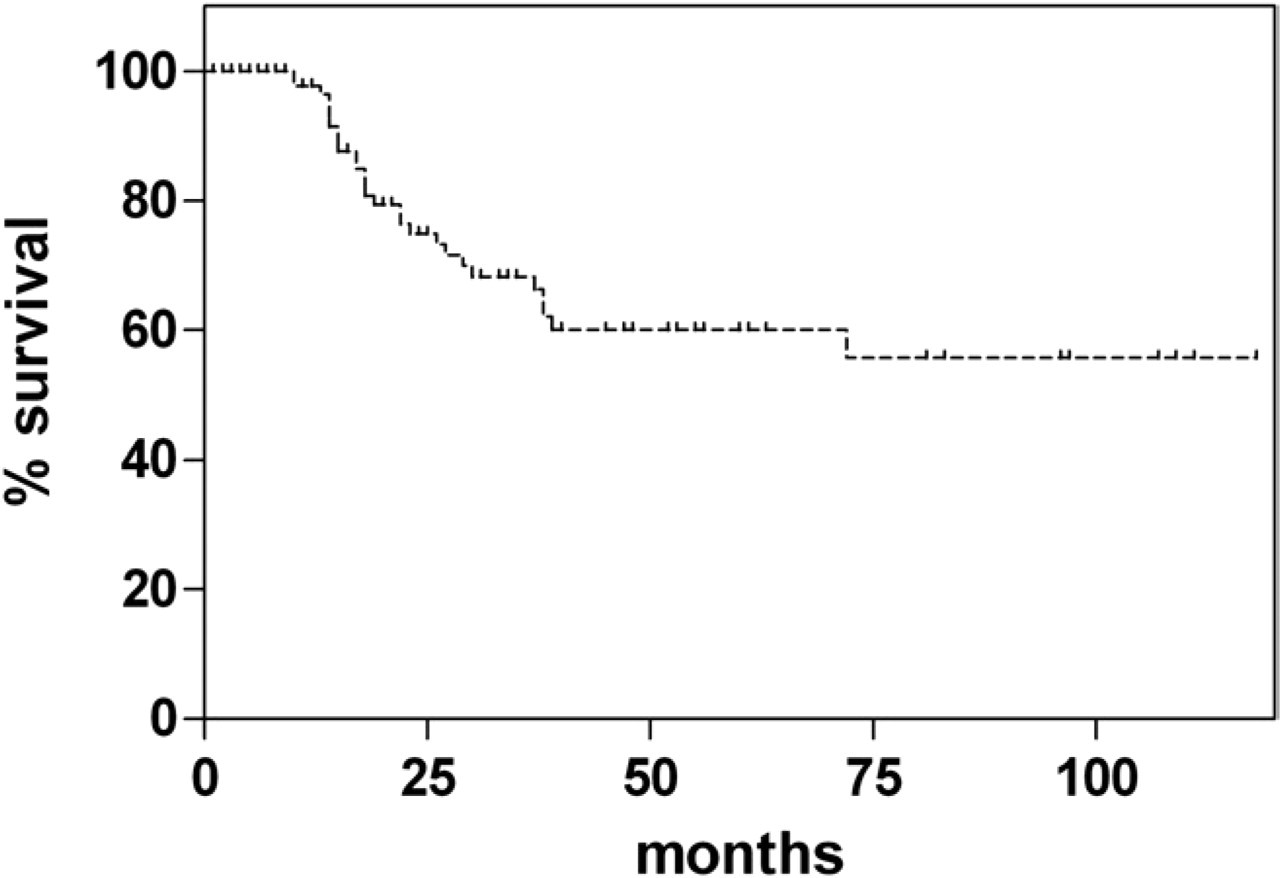
Locoregional control rates.
Univariate Cox proportional hazards analysis of the effect of variables on survival among patients treated with primary surgery for oropharyngeal cancer
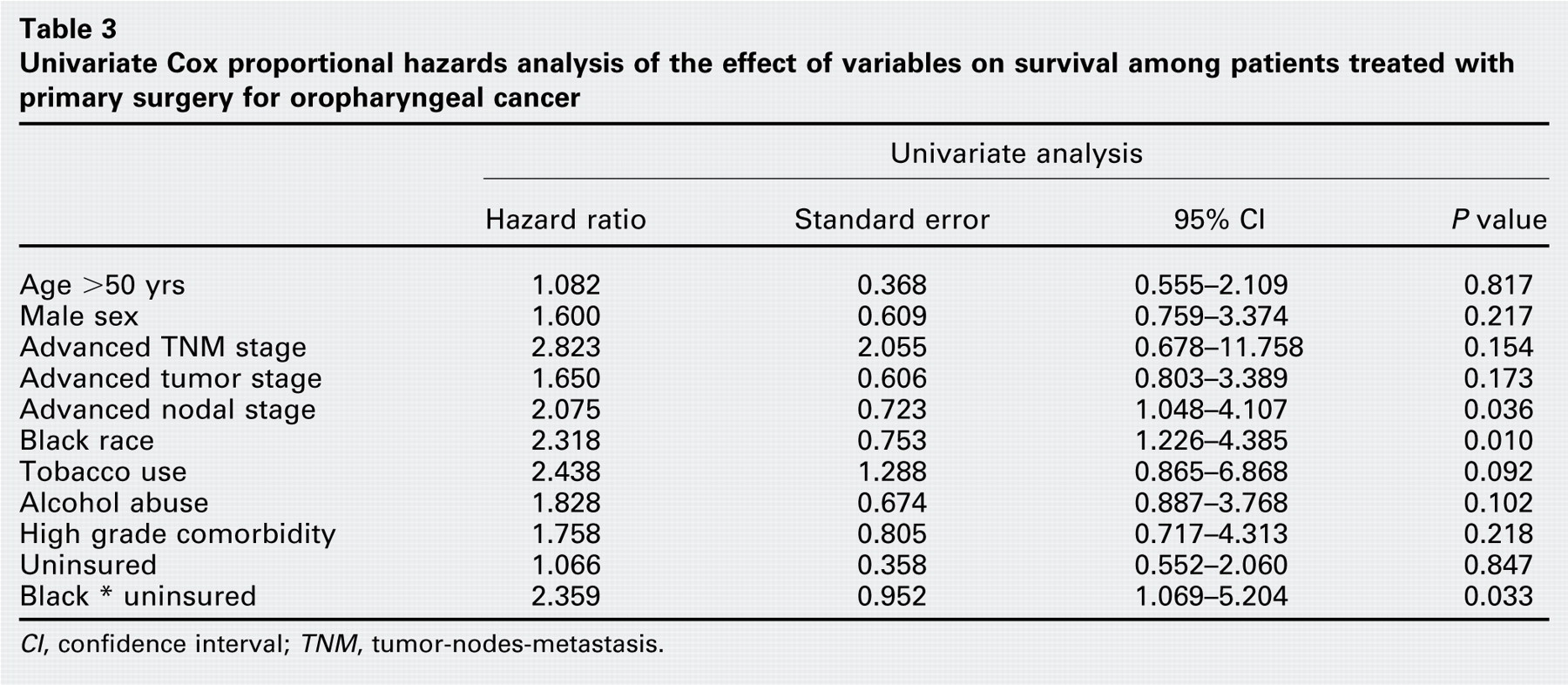
CI, confidence interval; TNM, tumor-nodes-metastasis.
The survival benefit of HPV-positive disease suggests that some patients with HPV-positive disease may benefit from less toxic regimens, although this hypothesis requires formal testing in the clinical trial setting. Our data demonstrate that excellent locoregional control and survival are achieved with a primary surgical approach that does not include adjuvant chemotherapy in the majority of cases. Because nonoperative therapy appears less likely to be successful in HPV-negative disease and the results of surgical salvage are poor, future research must focus on delineating differences in outcome in patients with oropharyngeal SCCA based on HPV status to optimize treatment selection and outcomes and identify those patients who would benefit from a primary surgical approach.
Multivariable Cox proportional hazards analysis of the effect of variables significantly associated with survival among patients treated with primary surgery for oropharyngeal cancer
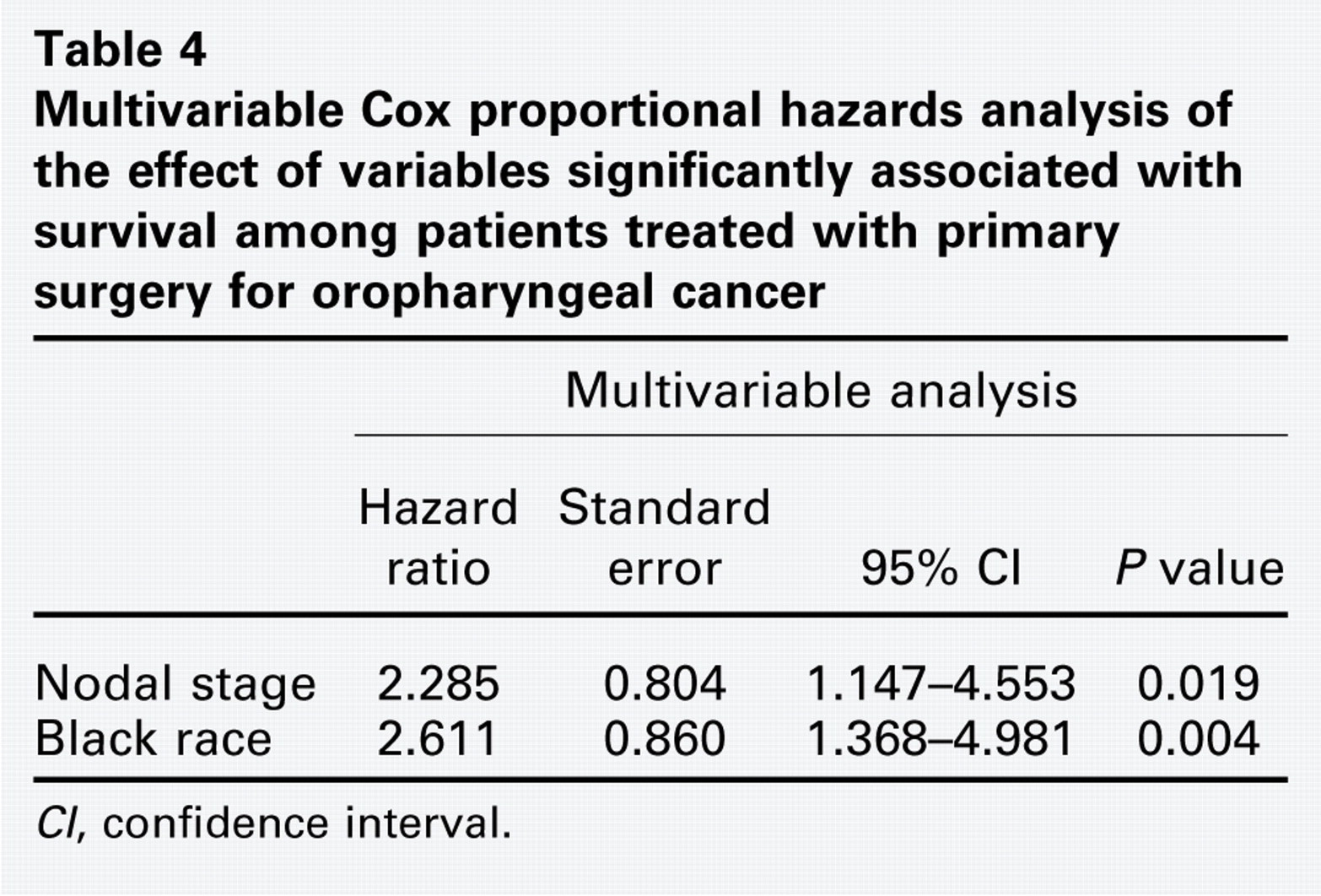
CI, confidence interval.
Conclusions
Primary surgical treatment of oropharyngeal SCCA is effective in achieving excellent locoregional control and permits deintensification of adjuvant therapy, even in patients with advanced stage disease. Nodal status and race are the primary determinants of disease-free survival. These data provide useful information for counseling and treatment planning.
Footnotes
Author Contributions
Disclosures