
Abstract
As in many other surgical fields, the desire for improved cosmesis has heavily influenced surgical technique within endocrine surgery. After the success of endoscopic parathyroidectomy at the end of the 20th century, surgeons began to explore the possibility of endoscopic thyroidectomy. 1,2 Although multiple techniques for endoscopic thyroidectomy exist worldwide, minimally invasive video-assisted thyroidectomy (MIVAT), championed by Miccoli et al at the University of Pisa, 2 has become the most popular. During MIVAT, a 1.5- to 2.5-cm incision is made that provides direct access to the thyroid via endoscopic visualization.
The most compelling analysis of MIVAT outcomes was performed by Miccoli and his colleagues in Italy in an 833-patient prospective cohort 3 published in 2006. Patient satisfaction, scar length, length of hospitalization, number of complications, and control of pain have consistently either equaled or surpassed the results of traditional open thyroidectomies. 3–5 In the United States, Terris et al 6,7 at the Medical College of Georgia and Ujiki et al 8 at Northwestern University have both shown MIVAT to be equivalent to conventional thyroidectomy or minimally invasive thyroidectomy (conventional thyroidectomy through a 3- to 5-cm incision). Ujiki et al 8 also found that patients who undergo MIVAT experience less postoperative pain.
By retrospectively reviewing thyroidectomies at the Medical University of South Carolina, we noted that operative times and hospital stays appeared to be shorter for MIVAT than traditional thyroidectomies. Given the worsening national health care crisis and growing concern over the allocation of health care dollars, we believe that a thorough cost comparison of MIVAT versus the traditional procedure is prudent. We project that MIVAT is less costly than open thyroidectomy as the result of shorter operative hospitalization times in a cost-effective analysis.
Materials and Methods
With approval from the Medical University of South Carolina's (MUSC) Institutional Review Board, all thyroidectomies performed by head and neck surgeons at MUSC between January 5, 2006, and November 1, 2007, were reviewed retrospectively. MIVAT and traditional or minimally invasive open thyroidectomies meeting MIVAT inclusion criteria were then compared. There were two surgeons who performed MIVAT and seven who performed open thyroidectomy, including the two MIVAT surgeons, who also performed open thyroidectomy as the result of patient preference, equipment availability, or exclusion on the basis of criteria that were initially narrower. Exclusion criteria for MIVAT were as follows: previous ipsilateral thyroid surgeries, thyroiditis, metastatic disease, or significant substernal or retroesophageal extension. Visibly massive thyroids also were excluded.
Open thyroidectomies were considered appropriate for comparison with MIVAT if preoperative ultrasound nodule volume was 27 mL or less or by postoperative pathology data in patients without ultrasound if nodule volume was 27 mL or less, nodule cross-sectional area was 9 cm2 or smaller, or nodule diameter was 3 cm or smaller. The basis of these exclusion criteria is that a 3-cm × 3-cm × 3-cm nodule is the largest size that can be expected to be delivered through a MIVAT incision per a personal communication with Dr. Miccoli. Patients undergoing procedures that would significantly increase time in the operating room, including lateral or central compartment lymph node dissection, partial thymectomy, parathyroidectomy/neck exploration, or excision of unrelated skin/buccal lesions, were excluded. Surgeries that included parathyroid reimplantation were included.
Our MIVAT technique was fashioned on the basis of the technique described by Miccoli et al. 9–11 Resident involvement in MIVAT and open thyroidectomy was comparable. All procedures were performed under general anesthesia. Use of standard endotracheal tubes versus Xomed laryngeal monitoring endotracheal tubes varied by surgeon. No drains were used in either group.
Patient data were obtained from electronic medical records and included gender, age, race, height, weight, preoperative diagnosis, total thyroid and thyroid nodule size on ultrasound, thyroid pathology specimen weight and size, and diagnosis and nodule size per pathology. Outcome data included length of operation, estimated blood loss, length of hospital stay (LOS), complications, and length of follow-up. Body mass index was calculated by the use of BMI+ v.1.2 Epocrates-AAC Essentials for Cardiology (Epocrates, Inc., San Mateo, CA).
Cost data (U.S.$) were obtained from University Medical Associates Coding, Revenue Enhancement & Charge Capture Department, including anesthesia, surgical, pathology, and hospital charges. Anesthesia charges included the fees of the anesthesiologist and nurse anesthetist (if used), anesthesia time charges, and agents used. The surgical costs reflected the hospital charges for Current Procedural Terminology codes included by the attending surgeon. Hospital costs included surgical and perioperative supplies, operating room time, and facility fees. Pathology costs included the specimen processing costs and the pathologist fees. We calculated the total cost (excluding the surgery cost) by adding the anesthesia, pathology, and hospital costs.
Data Analysis
All data analyses were performed with Sample Power 2.0, SYSTAT 8.0, and Sigma Stat 3.5 (SPSS Science, Chicago, IL). Categorical variables were presented as percentages (%), and continuous variables were presented as mean ± SD. All continuous variables were assessed for normality by use of the Kolmogorov-Smirnov test.
Comparisons of outcomes were performed by use of the χ2 test (categorical variables), the t test (continuous variables), and the Fisher's exact test (expected observations in one or more groups (< 5). Linear regression was used to determine the learning curve associated with MIVAT. A P < 0.05 was considered statistically significant for all statistical tests. In addition, two (MIVAT vs open thyroidectomy) times two (hemithyroidectomy vs open thyroidectomy) analyses of variance (ANOVA) were performed for certain variables. All means reported from ANOVA were least square means unless stated otherwise. When an ANOVA model was found to be significant (P < 0.05), post-hoc comparisons were performed.
Finally, all data were applied to a cost-effective model in which the following variables were calculated and compared between MIVAT versus the conventional procedure for hemithyroidectomy and total thyroidectomy: hospital LOS, anesthesia cost, hospital cost, postoperative complications, and total cost. An independent t test or a Mann-Whitney rank sum test was used to compare between the two groups. A sample size was estimated on the basis of a two-tailed significance level of P < 0.05. A power analysis was performed by the use of a t test. For hemithyroidectomy hospital cost, the sample size requirement of 30 participants per group with standard deviations of 154.52 for MIVAT and 147.85 for the open procedure was estimated to provide a 99.8 percent power to detect the mean difference of 192.2. For total cost, standard deviations of 236.25 and 277.47, respectively, were estimated to provide a 97.0 percent power to detect the mean difference of 259.0. For total thyroidectomy hospital cost, the sample size requirement of 30 participants per group with standard deviations of 594.94 and 124.37 was estimated to provide a 100 percent power to detect the mean difference of 833.6; standard deviations of 481.12 and 317.67 were estimated to provide a 100 percent power to detect the mean difference of 2301.2.
Results
A total of 185 thyroidectomies were performed by surgeons in the MUSC Department of Otolaryngology-Head and Neck Surgery between January 2006 and November 2007. Just more than one half of thyroidectomies (50.3%, 93 surgeries) met our criteria for performing MIVAT. Forty-two of these patients underwent MIVAT, and 51 patients underwent open thyroidectomy. Three MIVATs were converted to open procedure and were kept in the MIVAT group for analysis; one was ultimately excluded from the cost analysis because a central neck dissection was also performed. The remaining two involved extending the incision for nodule delivery only. Of the MIVATs, 31 of 42 (73.8%) underwent hemithyroidectomy, compared with 34 of 51 of open thyroidectomies (66.7%). The remaining 11 MIVATS (26.2%) and 17 open thyroidectomies (33.3%) had total thyroidectomies. When Pearson χ2 was used, we did not find the distribution of hemithyroidectomy and total thyroidectomy to be significantly different in either MIVAT or open thyroidectomy (χ2 1 = 0.558, P = 0.455).
Demographic and diagnostic data
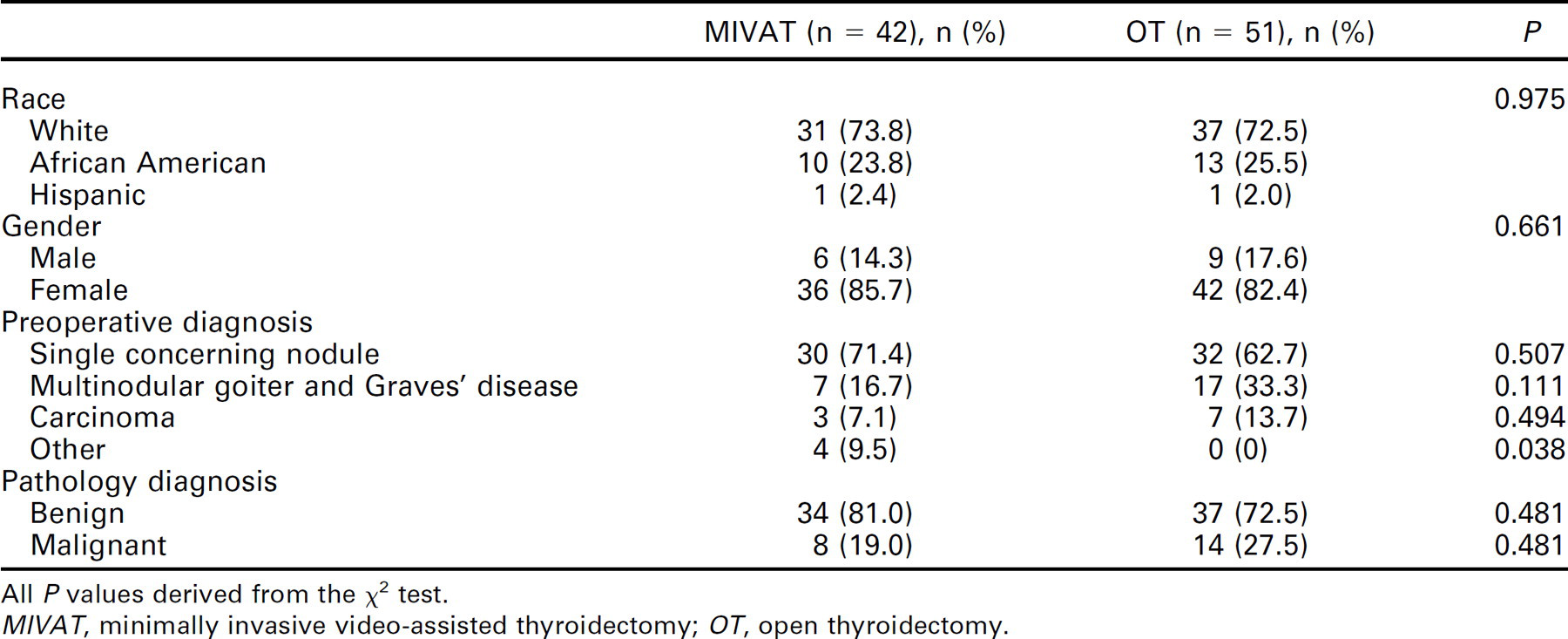
All P values derived from the χ2 test.
MIVAT, minimally invasive video-assisted thyroidectomy; OT, open thyroidectomy.
Demographic and pathologic data did not significantly differ between MIVAT and open thyroidectomy (Table 1). Difference in mean age (years) for MIVAT (50 ± 14.5) versus open thyroidectomy (48 ± 14.7) was not significant (t = 0.73, P = 0.467). The most common preoperative diagnosis in both groups was nodule with follicular cells but also included multinodular goiter, carcinoma, and other diagnoses (Table 1). There was no significant difference between MIVAT and open thyroidectomy mean specimen volume, weight, or nodule size (Table 2). Mean BMI for MIVAT (30.5) versus open thyroidectomy (28.3) was not significantly different (P = 0.142). Mean incision length was significantly shorter in MIVAT (2.3 cm) versus open thyroidectomy (4.3 cm, F (1, 65) = 38.682, P < 0.001). Mean length of follow-up was 20.3 months for MIVAT and 30.2 months for open thyroidectomy. The difference in follow-up was not significant on ANOVA (F(1, 89) = 2.919, P = 0.091). Postoperative complications included transient RLN palsy, permanent RLN palsy, transient hypocalcemia, permanent hypocalcemia, hematoma, seroma, superior laryngeal nerve palsy, and anesthesia complications. The overall complication rate was not significantly different between MIVAT and open thyroidectomy (31.0% vs 37.3%, χ2 1 = 0.405, P = 0.524). No individual complication was statistically different in MIVAT versus open thyroidectomy (P > 0.05, Fisher's exact test).
Thyroid nodule size and weight
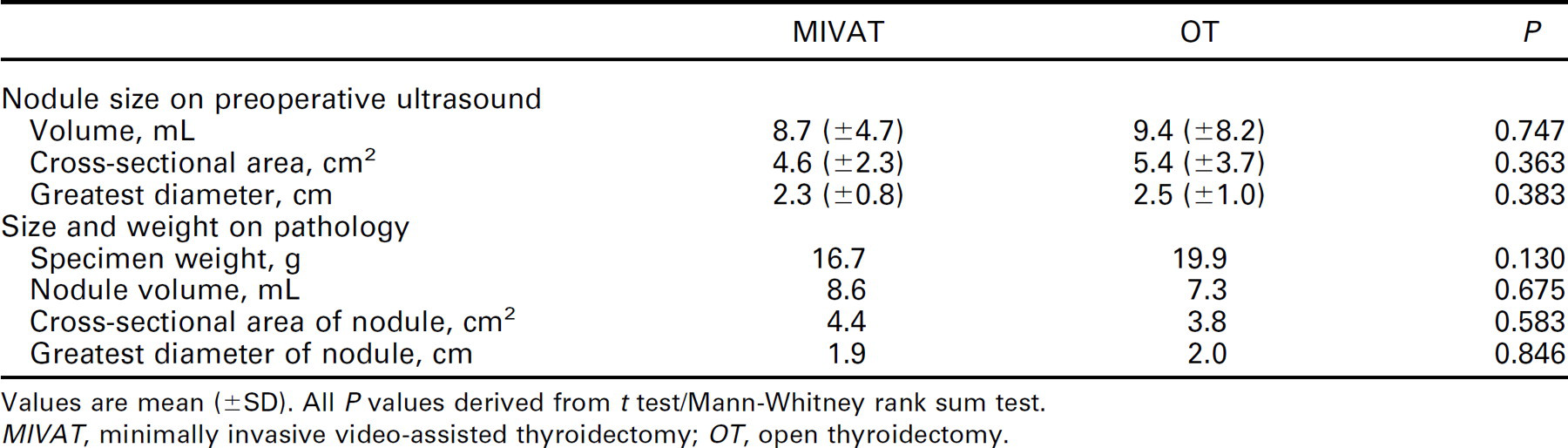
Values are mean (±SD). All P values derived from t test/Mann-Whitney rank sum test.
MIVAT, minimally invasive video-assisted thyroidectomy; OT, open thyroidectomy.
Hemithyroidectomy length of stay, anesthesia cost, pathology cost, hospital cost, total cost
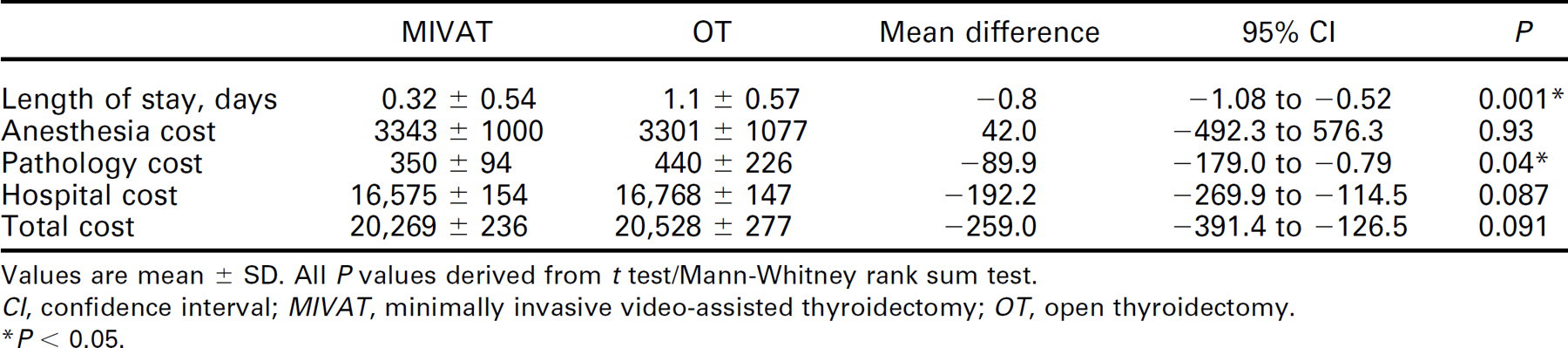
Values are mean ± SD. All P values derived from t test/Mann-Whitney rank sum test.
CI, confidence interval; MIVAT, minimally invasive video-assisted thyroidectomy; OT, open thyroidectomy.
* P < 0.05.
Mean LOS (days) in the hospital (MIVAT vs open thyroidectomy) and the mean cost of anesthesia, pathology, hospital, and total cost are summarized in Tables 3 and 4. LOS was significantly shorter in the MIVAT hemithyroidectomy group than in the open group (0.32 vs 1.1, P < 0.001) and was similar between groups for total thyroidectomies (1.9 vs 1.8, P = 0.87). Mean anesthesia cost (U.S.$) was similar between groups for both hemi- and total thyroidectomies. MIVAT mean pathology cost was significantly less than open thyroidectomy for hemithyroidectomy (350 vs 440, P = 0.04) and approached significance for total thyroidectomy (632 vs 775, P = 0.066). Hospital cost for hemithyroidectomy (16,576 vs 16,768, P = 0.087) and total thyroidectomy (22,856 vs 23,689, P = 0.078) was less for MIVAT than open thyroidectomy. Finally, the total cost was also less for MIVAT than open thyroidectomy for hemithyroidectomy (20,269 vs 20,528, P = 0.091) and total thyroidectomy (26,257 vs 28,558, P = 0.064). The surgeon's fees were equivalent between MIVAT and open thyroidectomy, since there is no separate Current Procedural Terminology code for the endoscopic procedure.
A two-way ANOVA was used to combine both hemi-and total thyroidectomies to compare MIVAT versus open thyroidectomy. The results were significant for mean hospital LOS, which was significantly shorter for MIVAT versus open thyroidectomy (1.16 days vs 1.62 days, F(1,89) = 7.812, P = 0.006). The interaction of MIVAT/open thyroidectomy and hemithyroidectomy/total thyroidectomy was significant (F(1, 89) = 7.812, P = 0.006). As a result, post hoc tests were performed that showed that the significance of MIVAT vs open hemithyroidectomy (0.323 days vs 1.235 days, F(1, 89) = 26.781, P < 0.001) was the major reason for the significant difference in hospital stay between MIVAT and open thyroidectomy.
Discussion
Some surgeons argue that the utility of MIVAT is limited by the increased operating times and cost; 12–15 however, our comparison of matched minimally invasive and open procedures demonstrates a shorter time in the operating room and no difference in overall cost. This relationship remains after excluding outliers in operative time (highest and lowest). The difference in pathology cost is significant but not relevant. It is uncertain whether more frozen sections were taken during open procedures than MIVAT or if more work was performed by the pathologists on the specimen after surgery. Given that the cost of MIVAT is equivalent to open thyroidectomy and that there are proven advantages to MIVAT over open thyroidectomy, including improved cosmesis4,6,9–10,12,13,16–23, and decreased postoperative pain, 4,8,10,12,14,17,18,22–24 fewer days in the hospital, and faster recovery, we argue that MIVAT is a cost-effective option for appropriately selected patients.
Total thyroidectomy length of stay, anesthesia cost, pathology cost, hospital cost, total cost
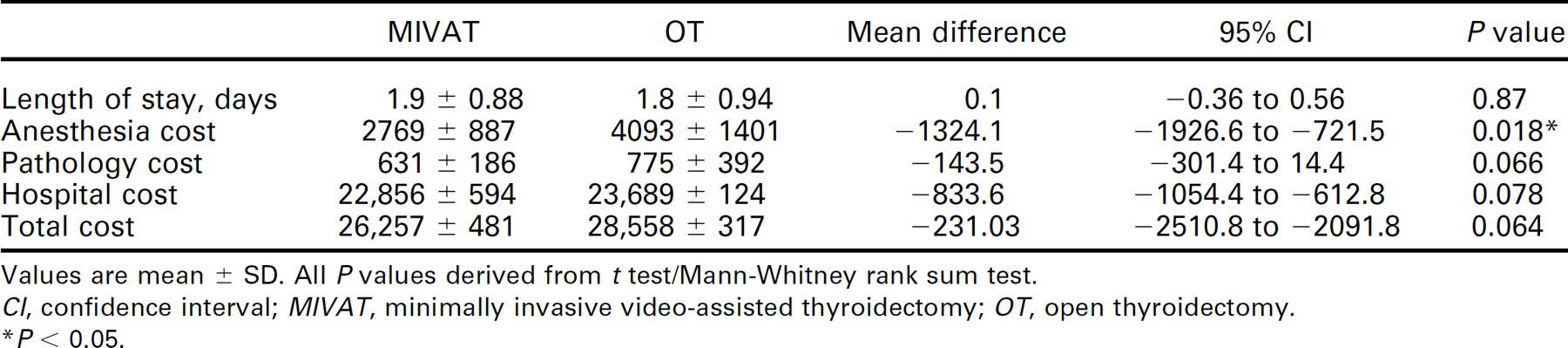
Values are mean ± SD. All P values derived from t test/Mann-Whitney rank sum test.
CI, confidence interval; MIVAT, minimally invasive video-assisted thyroidectomy; OT, open thyroidectomy.
* P < 0.05.
In our study, MIVAT and open thyroidectomy cohorts were not significantly different in size, thyroid volume, nodule size, and specimen weight on pathology. However, we recognize that a prospective study would create the strongest evidence of equal matching. The patient population eligible for MIVAT is more inclusive than previously thought; 50.3 percent were eligible, and 22.7 percent of all thyroidectomies performed in the time period were MIVAT. One potential difference between groups was the use of laryngeal EMG monitoring, which was used more often in MIVAT than open thyroidectomy due to surgeon preference. The costs of the tube and stimulator (U.S.$623) were included in the hospital cost (and therefore total cost) for these patients. The impact of this is unknown; however, it may in fact inflate the cost of MIVAT in our analysis.
More assistants are currently required to aid in MIVAT than for conventional thyroidectomy, which is not factored into the cost of the procedure at our institution because of resident involvement. In the private setting, this may change the cost relationship if an additional scrub nurse or surgeon is present. The need for a second assistant in surgery may be diminished in the future with the use of camera holders, more sophisticated self-retaining retractors, and robotics. 6
Assessment of these results should take into account several limitations of the study. There was a lack of statistical power because of small sample size to show statistical significance for most variables. Second, the nodule volume limit of 27 mL retrospectively applied to determine the eligibility of open thyroidectomies for MIVAT criteria postoperatively has no basis in the literature, although it is a more stringent criterion than was applied in selecting patients for MIVAT preoperatively. Third, the cost data reflect only a single institution's billing, and the actual overall cost may vary greatly worldwide. Finally, our model could not control for differences between surgeons in the data, and there were several more surgeons in the open thyroidectomy group than the MIVAT group, which are significant limitations. A large prospective, blinded, randomized trial controlling for surgeon and case-to-case variability should be considered for a future studies because selection bias is a problem inherent in any study comparing a new technique in certain patients versus those that were later determined to have been eligible.
Conclusion
In our study of matched cohorts, we found no difference in cost for MIVAT when compared with open thyroidectomy. The results of this study strengthen the argument for a minimally invasive procedure whose detractors argue that it is cost-prohibitive. These results suggest the need for a future multicenter, prospective study with larger sample sizes to verify our results.
Acknowledgment
We acknowledge Terry Day, MD (MUSC Department of Otolaryngology-Head and Neck Surgery), who provided valuable feedback throughout the manuscript drafting process.