
Abstract
OBJECTIVE
To assess current microvascular training strategies in otolaryngology residency programs.
STUDY DESIGN
Cross-sectional study.
SETTING
U.S. otolaryngology residency programs.
SUBJECTS AND METHODS
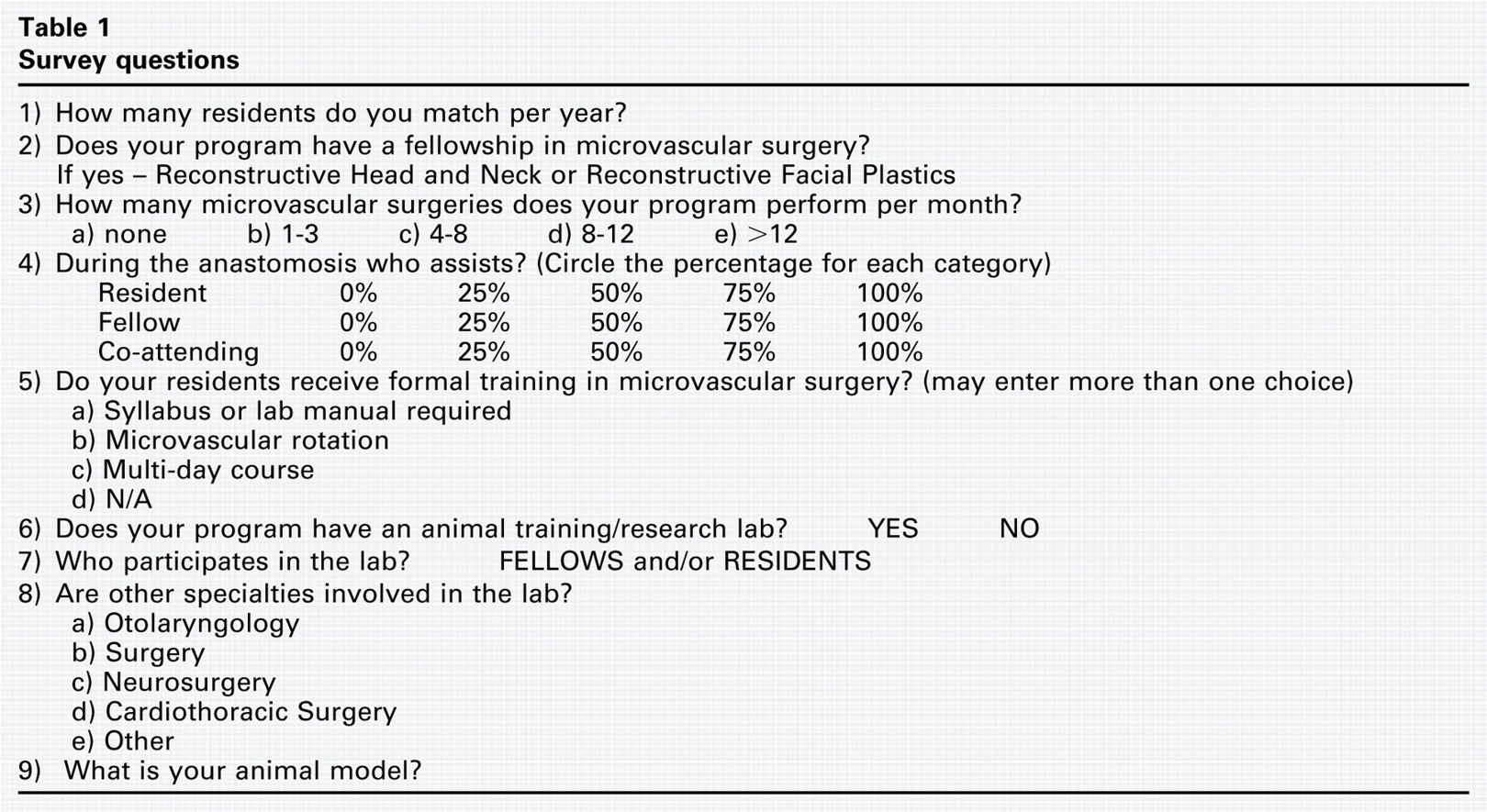
A total of 104 U.S. otolaryngology program directors received surveys inquiring about program size, the presence of fellowship training in microvascular surgery, the number of microvascular cases per month, the use of microvascular animal laboratory, and whether residents, fellows, or co-attendings assist in the anastomoses.
RESULTS
A 51 percent response rate was achieved, and of the 54 programs that responded, 78 percent reported no microvascular fellowship positions in plastics or head and neck reconstruction. A total of 52 percent reported performing three or fewer microvascular surgeries per month. Of the programs that did not have a microvascular fellow, only five (12%) performed eight or more surgeries per month. A total of 65 percent of the programs reported that residents assist during the anastomosis at least 75 percent of the time. Of the programs where residents assist 75 percent or more of the time, 70 percent have a formal training in microvascular technique ranging from demonstrating laboratory competencies to multiday courses. A total of 48 percent of the responding programs report having an animal laboratory for microvascular surgery. All animal laboratories used the rat as the model.
CONCLUSION
Many programs find value in providing residents with microvascular training, both in the operating room and in the laboratory. Only a small minority of programs without fellowship positions responded that they perform microvascular surgery on a regular basis (4 or more surgeries per month).
Despite considerable efforts at standardization, otolaryngology residency training programs may vary in the educational opportunities afforded their residents, especially with regard to surgical experience. Areas that tend to have the greatest variability of exposure between programs include skull base, cosmetic plastic procedures, microvascular surgery, allergy, and airway reconstruction. Focused training in these subspecialties is often reserved for fellowship recipients, decreasing the likelihood that they will be performed by the general otolaryngologist.
To improve and standardize procedural training, many specialties have invested in randomized, controlled trials of skills assessment that use simulation models for medical students and residents. Positive results have prompted programs to mandate the use of training models.1, 2 Specifically, otolaryngology residencies have refined educational courses in temporal bone dissection, cadaveric facial aesthetics, and airway management. More recently, the continued development of temporal bone virtual simulators and sinus simulators has led to their incorporation into residency program curricula.3, 4 The major objective of this study was to assess resident microvascular operative experiences and current training strategies across otolaryngology residency and fellowship programs in the United States.
Materials and Methods
A survey of 104 U.S. otolaryngology–head and neck residency program directors was performed. A 10-question survey was sent by an Internet survey company (http://www.surveymonkey.com) to the e-mail inboxes of the respective program directors. The survey included questions regarding residency size, the presence of a microvascular fellowship program in either head and neck or plastics reconstruction, the number of anastomoses performed each month, and the training level of the physician assisting the primary surgeon during anastomosis. For those programs that have instituted a formal microvascular training program, we asked a number of follow-up questions about their microvascular lab options (Table 1). The data were then categorized and analyzed in a descriptive manner. This study was exempt from IRB review according to the Thomas Jefferson University Hospital IRB committee.
Survey questions
Results
After the first distribution of the survey to 104 otolaryngology residency directors, 44 of the recipients responded (42%). Following a repeat request, this total was increased to 54 (52%). We found no significant difference between responding programs compared with nonresponding programs with regard to location or number of resident's per year (Fisher's exact test, P = 0.39 and P = 0.60) (Table 2).
Overall, 87 percent (47 of 54) of the programs that responded to the survey perform microvascular surgery to some degree. A total of 54 percent (29 of 54) of the total reported performing one to three microvascular procedures per month, whereas 17 percent (9 of 54) perform eight or more per month (Fig 1). In Question 4: “Who assists the attending?” the responder was able to choose 0, 25, 50, 75, or 100 percent of the time for each category (resident, fellow, and co-attending) and in 19 of the 54 total programs (35%), residents assist the attending during vessel anastomosis in most every case. The remaining 65 percent of programs indicated that fellows or co-attendings assisted more often during the anastomosis. Dedicated microvascular training programs are available to residents in approximately 63 percent (34 of 54) of programs. In 27 percent of responding programs, they have full rotations in microvascular surgery, with 46 percent of responders involved in laboratory training or multiday courses. Required competency was reported in only nine programs. To augment the teaching experience, nearly half (48%; 26 of 54) have an animal model training laboratory that may be used by residents and fellows. All animal laboratories use the rat model.
Among the programs that responded, eight (15%) have a microvascular head and neck reconstructive fellowship, and four (7%) have a microvascular facial plastics fellowship. In these programs with fellowships, four (33%) perform eight or more microvascular surgeries per month, yet none perform more than 12. A total of 58 percent of this subset of programs has an animal research laboratory in microvascular surgery. However, the majority of these programs do not have a formal microvascular training program in which residents can participate. Only three of these 12 fellowship programs identified that residents assist the attending during anastomosis more than 50 percent of the time.
Program location and residents/year (responders vs nonresponders)
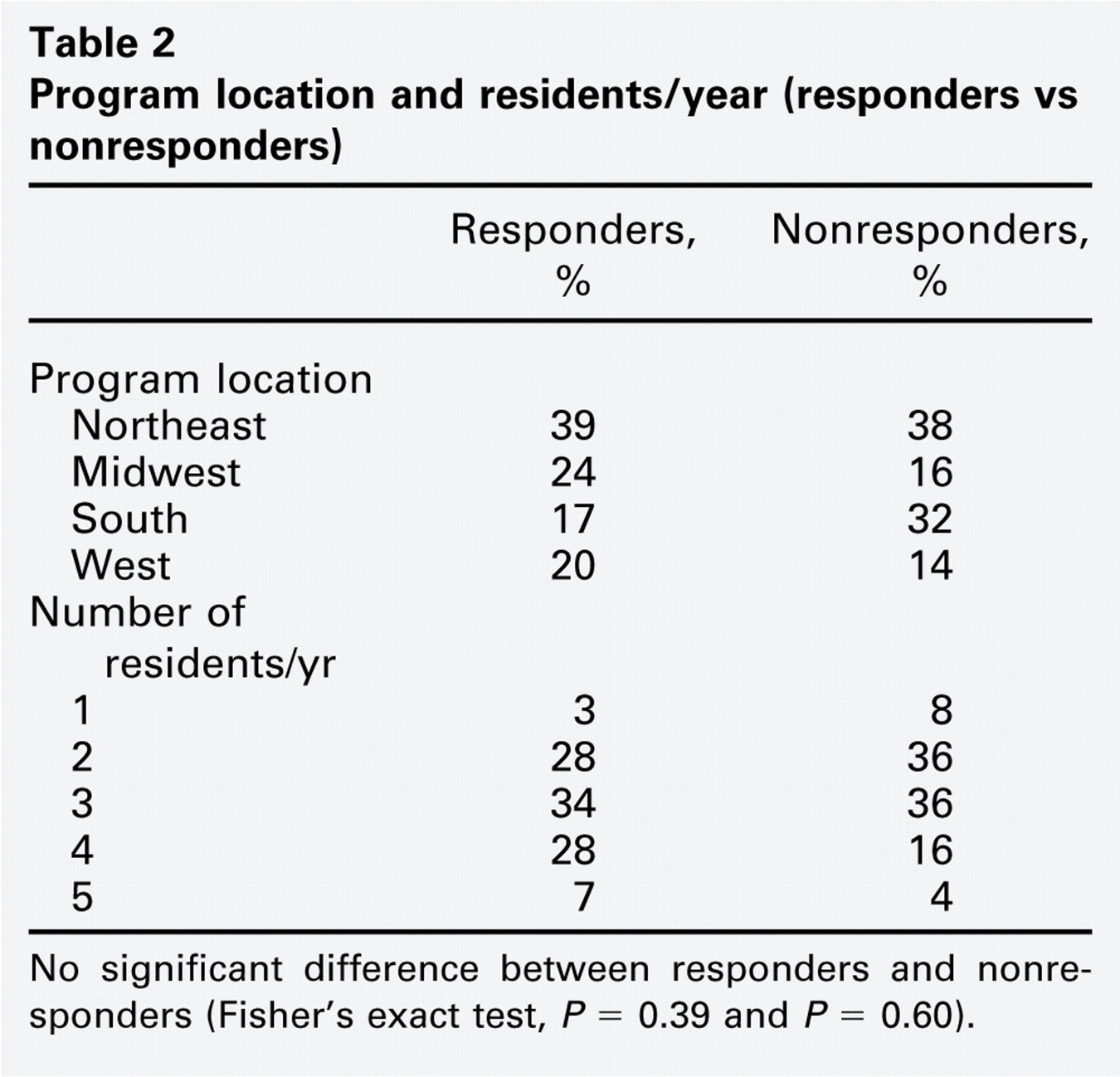
No significant difference between responders and nonresponders (Fisher's exact test, P = 0.39 and P = 0.60).
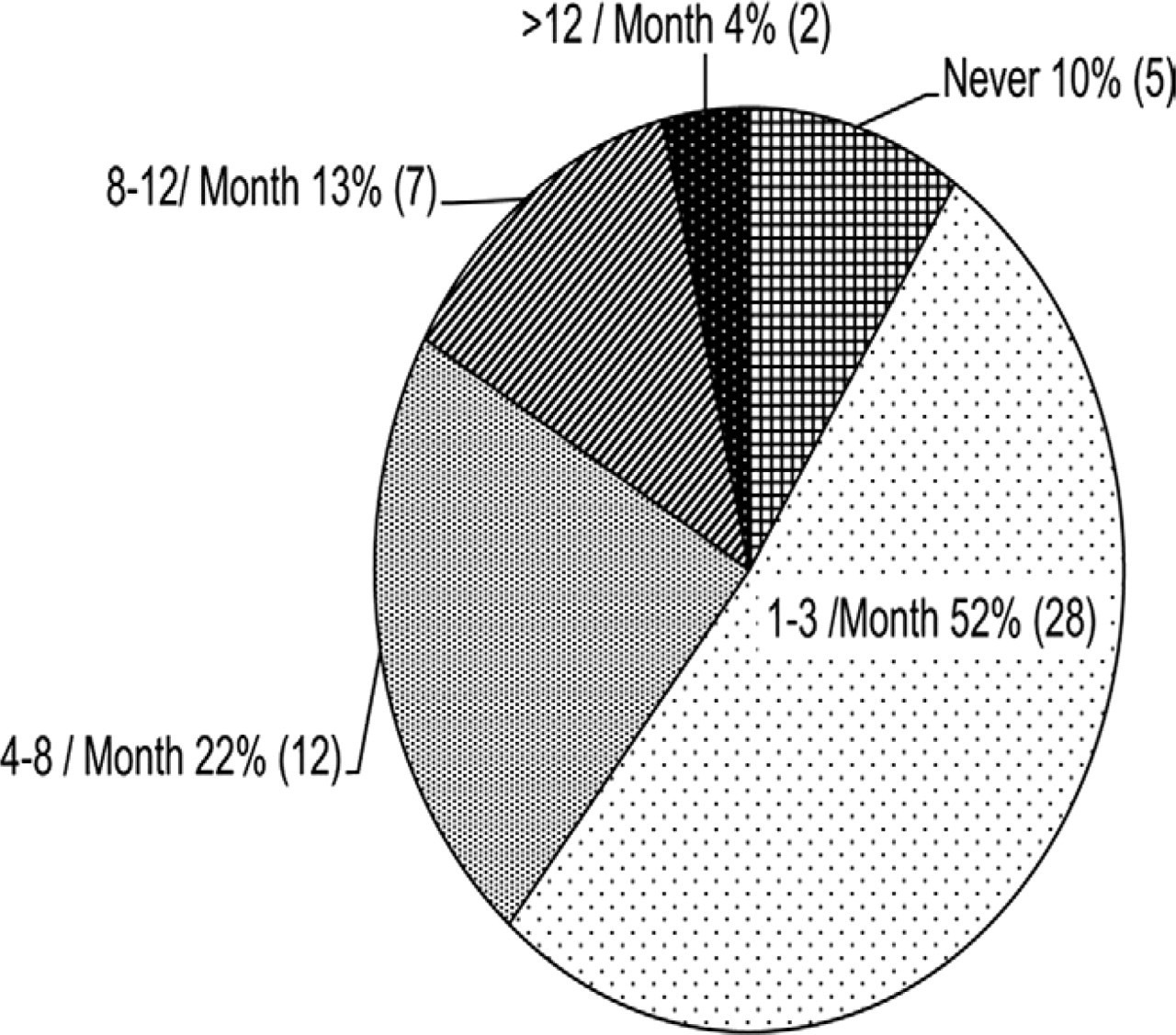
Number of free flaps performed per month at responding U.S. otolaryngology programs.
Twenty-five of the 42 otolaryngology programs (60%) without associated fellowships that responded to the survey perform one to three microvascular cases per month; 12 percent (5 of 42) of this subcategory complete at least eight cases per month, including two programs that accomplish 12 or more microvascular cases per month. There were 12 programs with no microvascular fellows and a high volume of cases (4 or more per month), 67 percent (8 of 12) of programs responded that resident surgeons assist during the anastomosis 75 percent or more of the time (Fig 2). A total of 62 percent (26 of 42) of nonfellowship programs include some form of structured microvascular training activity. However, there was no preference noted for the type of resident training because it was spread evenly between syllabus/laboratory manual, full microvascular rotation, and a multiday course. More than 48 percent (20 of 42) have an animal microvascular laboratory. The breakdown of which programs used the microvascular rat laboratory was as follows. Of the programs designated as low volume (1 to 3 per month) the majority, 77 percent (10 of 13), did not have microvascular rat laboratories in their curricula and used co-attendings as the assistant to the reconstructive surgeon. Those programs with greater volume (≥ 4 per month) without fellows had identified residents as the primary assistant more than 75 percent of the time had rat microvascular laboratories at 50 percent (6 of 12) of the programs. The final category of programs with fellows as the primary assistant revealed 75 percent (9 of 12) with microvascular rat labs (Fig 2).
Discussion
The collected institutional survey data yielded three broad types of programs (Fig 2). The first type had an associated microvascular fellowship (reconstructive head and neck or reconstructive facial plastics) and performed greater than or equal to eight free flap procedures per month. The fellows were involved in 100 percent of the anastomosis, and residents therefore played a minor role. In the second type of program, fewer than three free flaps per month were performed, and during anastomosis, the attending microvascular surgeon was usually joined by a second attending. Residents, again, took a subordinate role during anastomosis and had no specific training program or requirements in microvascular surgery. The final program category completed a robust number of microvascular flaps per month (approximately 8), even without the benefit of a fellowship program. Residents assisted in the majority of cases and also had access to an associated animal laboratory for further training. A total of 80 percent of the rat vessels training regimens were performed as either an intense, one-week course or in an ongoing microvascular laboratory.
Moulton et al2 concluded that those who received microvascular training distributed over the course of several weeks outperformed peers who received an equal curriculum during an intensive microvascular course. The fundamental reasoning behind this model design can be best likened to athletic skill: practice interrupted by rest leads to greater retention and overall improved capabilities. An animal laboratory allows for supplemental physical learning to be experienced outside of the operating room. Its availability year-round fosters continuous growth and retention of skills.
Free tissue transfer with microvascular surgery remains the last rung in the interventional ladder of reconstructive surgeons. Because of the inherent complexity of microsurgery, the necessary knowledge base and dexterity take time to acquire in a training environment. Lascar et al5 demonstrated that first-year residents required an average of 36 attempted anastomoses to attain a 90 percent patency rate. Fourth-year residents who already had completed an abbreviated training course necessitated 28 anastomosis attempts to reach an adequate success rate plateau. Conversely, proficient attendings achieved a 95 percent success rate after their first set of four anastomoses.5, 6 The authors concluded that a progressive, multimodal protocol was superior to an intensive course in creating a positive learning curve in microsurgical training.
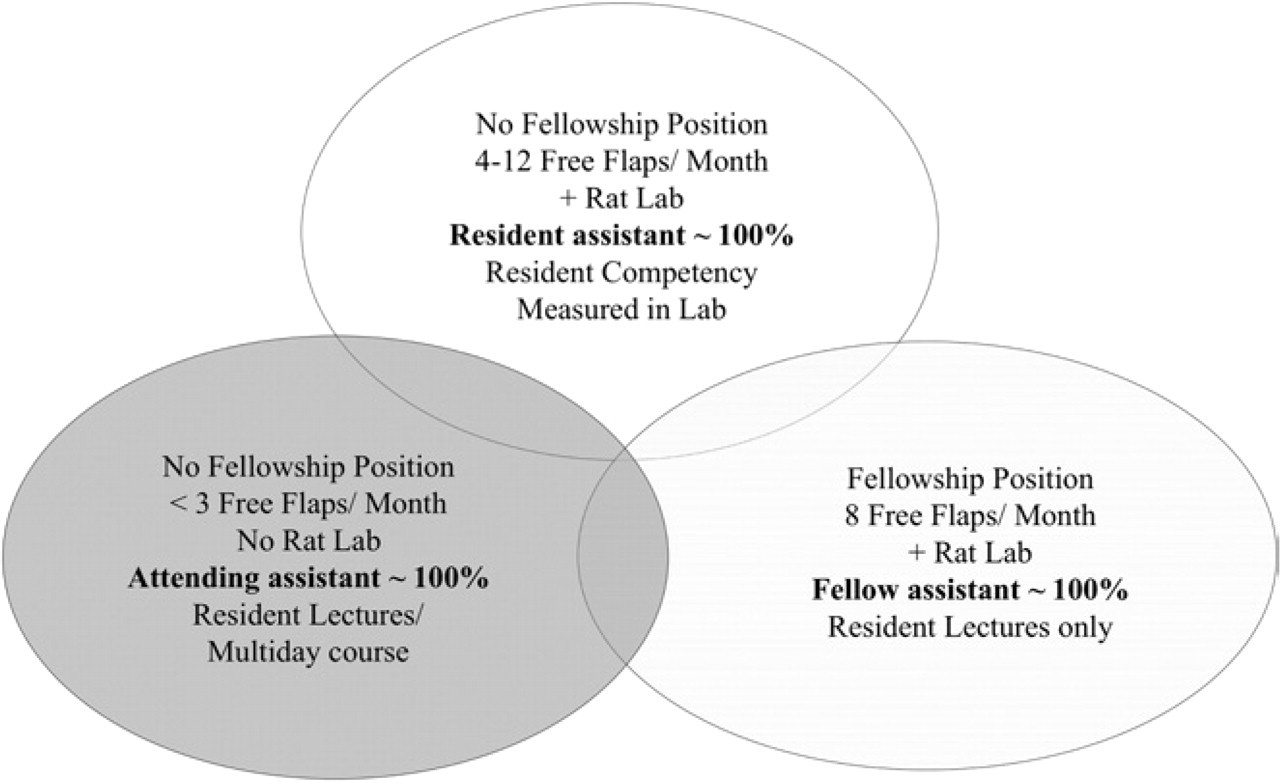
Each circle describes the three major types of programs that were reported in the survey. Although the majority of programs (80%) fit into these silos of who assists the primary surgeon, there is a five to 10 percent overlap of program description in this Venn diagram.
Similarly, Sidhu et al7 evaluated the efficacy of training on the basis of the fidelity of this training model and found that residents trained with complex vessels outperformed counterparts who trained on nontissue alternatives. In this study population, the degree of anastomosis success was independent of the participant's residency level. Furthermore, Lascar et al5 also demonstrated that the number of anastomosis attempts necessary to achieve competency was not significantly different between junior residents and senior residents. Although the authors of these studies have examined outcomes in the laboratory, the limitation of our survey and questions that remain are 1) trainee performance in the clinical setting, 2) how these animal training models translate into improved clinical performance, and 3) how these programs measure resident/fellow competence. We have asked questions that address structure of training and experience, and we have established the prevalence of animal laboratories within those programs that responded to the survey.
The limited response rates inherent in surveys yield an incomplete picture. This study presents a subset of programs that statistically do not appear to be different in geographic location or number of residents per year (Table 2). We expect a sampling bias with underrepresentation of programs that do not perform microvascular surgery on a regular basis. It is well known that responses to voluntary surveys are driven in large part to the interest of the responder. Follow-up communication with the program directors yielded an additional 10 responses.
Among the responding program population, the vast majority (75%) performs fewer than eight flaps per month, whereas 50 percent of all programs perform fewer than three per month. Multiple factors influence the degree to which microvascular surgery is incorporated into the program. Causes of a decreased allotment of such cases include the employment of plastic surgeons for the microvascular anastomosis or the preferred use of large pedicled flaps for reconstruction. During the past decade, microvascular surgical fellowships have produced dozens of otolaryngology-trained physicians to perform these operations. We expect that as these specialized surgeons continue to join academic otolaryngology faculty more programs in the future will focus on the development of these advanced techniques for their residents.
Conclusion
This study demonstrates that many programs find value in providing residents with microvascular training, both in the operating room and in the laboratory. A minority of responding programs without fellows performs microvascular surgery on a regular basis (≥ 4 surgeries per month), and residents in these programs will have significant exposure to microvascular anastomosis during their training. We also found that busy programs to facilitate in training of their residents and fellows use the animal microvascular model.
Footnotes
Acknowledgments
We thank Michael Savino and Joanne Gathier.
Author Contributions
Disclosures