
Abstract
The present study investigated the effects of supervision on the management of vicarious traumatisation among telephone and online counsellors on BoysTown Helplines. BoysTown Helplines include Kids Helpline, a 24-hour national counselling service for young people aged 5–25 years of age, and Parentline (PL), a counselling service for parents in Queensland and Northern Territory. The services provide telephone and email counselling services and Kids Helpline also provides web counselling. All counsellors (100%) worked as Kids Helpline counsellors (N = 38) and 42.1% (n = 16) as PL counsellors. The counsellors conducted 50,979 counselling sessions in 2008, of which 38,703 were completed over the telephone and 12,276 online. Of these, approximately 44% involved trauma clients, putting the counsellors at risk of suffering some level of vicarious traumatisation. The findings from 38 supervised telephone and online counsellors showed that vicarious traumatisation fell within normal limits and positive coping strategies were above average. While correlations did not prove to be significant between supervision and vicarious traumatisation, the size of counsellors’ trauma caseload proved to be strongly related to both vicarious traumatisation and negative coping style.
Telephone and online networks are now recognised as increasingly important counselling mediums as they have a unique facility to create alternate access pathways for those who may not otherwise access a clinic-based counselling service, a fact acknowledged by a national review of telephone and online counselling services (Urbis Keys Young, 2003). Significantly, while both telephone and online counselling confer advantages on trauma clients there are drawbacks to these forms of counselling (for a review see Taylor & Furlonger, 2011). One of these drawbacks, although not unique to digital counselling environments, is the effect of vicarious traumatisation on counsellors. Vicarious traumatisation itself is known to impact on the wellbeing of telephone counsellors (Dunkley & Whelan, 2006a; Mauldin, 2001).
Conversely, supervision is assumed to act as a preventative measure for vicarious trauma through the provision of a safe environment for counsellors to process their reactions to and develop adaptive strategies for working with trauma clients (Adams & Riggs, 2008; Courtois, Ford, & Coitre, 2009; Dunkley & Whelan, 2006a; Harrison & Westwood, 2009; Wheeler, 2007). However, the value of supervision has been inconsistently supported in the trauma literature (Bober & Regehr, 2006; Sabin-Farrell & Turpin, 2003). Indeed, there is little research to support the assumption that supervision ameliorates the effects of vicarious traumatisation on telephone and online counsellors (Dunkley & Whelan, 2006b; Mauldin, 2001), leading to the conclusion that a further examination of the role supervision plays in assisting counsellors working with trauma clients in digital environments is justified.
In what follows, the term ‘vicarious traumatisation’ (VT) is defined, factors contributing to VT are examined, the effects of supervision on counsellors’ wellbeing are reviewed, and finally, details of the current study that aimed to examine the relationship between supervision and VT among telephone and online counsellors are presented. For the purposes of this study, the term ‘vicarious traumatisation’ is defined as ‘the negative transformation in the helper that results from empathic engagement with trauma survivors and their trauma material, combined with a commitment or responsibility to help them’ (Pearlman & Caringi, 2009, p. 202). The Constructivist Self-Development Theory (CSDT) of McCann and Pearlman (1990) underpins the definition of VT preferred in the present study. The authors of the theory contend that the construction of individual realities is formed by way of the development of unique cognitive structures (schema) used to interpret events. Within the CSDT model, schemas are described as a belief, assumption or expectation of self and the world that enables an individual to make sense of their experiences. As each counsellor's response is unique to the complex interplay between intrinsic experiences of the traumatic event and the context of work, negative effects are seen to depend on the clinician's ability to integrate and transform client's trauma stories into their own schema in a way that may or may not be problematic (Pearlman & Saakvitne, 1995; Pearlman & Mac Ian, 1995).
Key factors that contribute to greater risk for negative effects of trauma work have been identified as a counsellor history of personal trauma (particularly in childhood), counsellor caseloads with a high proportion of trauma clients, and less counsellor experience in working with trauma clients and therefore less opportunity to develop coping skills to manage harmful schema disruptions (Bride, 2004). Conversely, the use of social supports and positive coping strategies were found to be associated with lower risk (Schauben & Frazier, 1995). As a result, there has been a commensurate interest in understanding how counsellors adapt a positive coping style (Adams & Riggs, 2008; Bride, 2004; Dunkley & Whelan, 2006a; Sabin-Farrell & Turpin, 2003). Tentative links have been demonstrated between supervision and a positive coping style, indicating the relevance of further investigation into how supervision works to facilitate adaptive behaviours for counsellors (Follette, Polusny, & Milbeck, 1994; Dunkley & Whelan, 2006a; Iliffe & Steed, 2000). Supervision has been linked to the development of counsellors’ awareness of their personal internal process when engaging in trauma work, the early recognition of possible negative responses to trauma work and subsequent proactive determination of positive coping strategies (Adams & Riggs, 2008; Dunkley & Whelan, 2006a; Harrison & Westwood, 2009). Thus, potentially, supervision can provide a safe, facilitative environment within which counsellors can process their response to trauma work and develop self awareness and professional boundaries enabling them to proactively address trauma related responses and to serve as a component of self-care (Adams & Riggs, 2008; Bride & Figley, 2007; Courtois et al., 2009; Follette et al., 1994; Harrison & Westwood, 2009).
Regrettably, counsellors often do not access supervision (Dunkley & Whelan, 2006a; Wheeler & Richards, 2007). An explanation for the avoidance of supervision by both experienced and inexperienced counsellors advanced by a number of researchers is that counsellors experience feelings of anxiety, shame or incompetence in relation to their trauma work, which in turn leads to the avoidance of supervision (Deutsch, 1985; Ladany, Hill, Corbett, & Nutt, 1996; Neumann & Gamble, 1995). Termed ‘impression management’, this behaviour is related to counsellors’ perceived need to be regarded by their supervisor as a highly competent and effective mental health professional (Ladany et al., 1996). In contrast, counsellors who were less concerned with how they might be viewed within a supervisory context demonstrated that supervisory engagement enhanced their self-awareness and therapeutic ability, providing evidence for the utility of proactively addressing the negative effects of trauma work in an effective and timely way (Adams & Riggs, 2008; Bride & Figley, 2007; Courtois et al., 2009; Pearlman & Caringi, 2009; Wheeler & Richards, 2007).
In summary, when studies have demonstrated the advantages of supervision for counsellors, they have been undertaken with counsellors working in traditional face-to-face environments. There is much less evidence on the effects of supervision to address the negative responses to trauma work of telephone and online counsellors in order to evade the cumulative, transformative effect of VT described by Pearlman and Saakvitne (1995). Likewise, there is a lack of evidence on the importance of the relationship between the supervisory alliance and positive benefits for the counsellor. Therefore, the aim of the present study was to investigate the relationship between supervision and vicarious traumatisation experienced by telephone and online counsellors. Accordingly, it was assumed that counsellors who had experienced regular supervised practice would exhibit normal levels of VT. It was also anticipated that counsellors undergoing regular and compulsory supervision would also report above average positive coping styles (i.e., problem-solving and seeking social support). In addition, there was also an expectation that there would be a significant relationship between years of supervison and VT, years of supervision and positive coping style, strength of working alliance with a supervisor and VT, and finally, strength of working alliance with supervisor and positive coping style.
Method
Participants
Participants for this study were all recruited from BoysTown Counselling Services’ Kids Helpline and Parentline. All counsellors in the present study worked on Kids Helpline telephones and of these counsellors 42.1% (n = 16) also worked as Parentline counsellors. Clinical supervision is a mandatory condition of employment for all counsellors. Full-time counsellors attend fortnightly sessions and part-time counsellors attend monthly sessions.
Clinical practice supervisors are experienced counsellors, employed specifically for this role, who hold postgraduate qualifications in a counselling-related field. ‘Clinical supervision’ was defined in BoysTown Policy and Procedure documents as a supportive, professional development process that aims to assist staff to develop confidence, competence and creativity in their work. A total of 38 counsellors from a possible pool of 75 BoysTown telephone counsellors voluntarily responded to a request to complete a survey (response rate of 50.7%). Of these, 13 were men (34.2%) and 25 were women (65.8%) with an age range of 23.8 to 60.8 years (M = 36.7 years, SD = 11.0). The proportion of men to women, while varying a little over time, is typically 25% male to 75% female. All participants were paid professionals with backgrounds in psychology, social work, teaching or nursing. The average time spent working as telephone counsellors was 4.2 years (SD = 3.9), and as counsellors for BoysTown Helpline Counselling services, 3.8 years (SD = 3.9). All participants (100%, of N = 38) worked on telephones; 44.7% (n = 17) also worked on email counselling; 28.9% (n = 11) worked on telephone, email and web counselling and were obliged by management to access on-site debriefing and monthly supervision sessions.
Measures
Demographic information
Data collected included age, gender, years of counselling experience, trauma caseload numbers, time working on BoysTown Helpline (BTHL), and weekly contact with trauma clients.
Qualitative information
Information was sought on the caseload of trauma clients carried by counsellors. Trauma was defined in this questionnaire as ‘a unique individual experience, associated with an event of enduring conditions to which (1) the individual's ability to integrate affective experience is overwhelmed or (2) the individual experiences a threat to life or bodily integrity’ (Pearlman & Saakvitne, 1995, p. 60).
Trauma Attachment and Belief Scale (TABS)
This is is an 84-item, pen and paper self-report questionnaire designed to assess the impact of trauma, particularly disrupted beliefs related to the five areas of psychological need: control, esteem, intimacy, safety and trust (Pearlman, 2003). The measure yields a total score together with 10 subscale scores related to separate items that tap into beliefs about oneself and others (e.g., self-safety and other-safety). Information is acquired by participants responding to statements that were typically posed in the following way: (Item 1) ‘I believe I am safe’ is a negatively structured item relating to Subscale Self Safety. Higher scores reflect greater disruption of beliefs. The measure uses a 6-point Likert scale (1 = disagree strongly, 6 = agree strongly). Negative items are reverse scored. Internal consistency estimates of .96 and a test–retest correlation of .75 for the total score have been reported.
Coping Strategy Indicator (CSI)
This assessment examines coping styles across three dimensions of problem-solving (e.g., ‘tried to solve the problem’), seeking social support (e.g., ‘confided your fears and worries to a friend or relative’) and avoidance (e.g., ‘daydreamed about better times’), reflecting distinct, fundamental modes of response. Participants provided information by responding to statements that were related to a particular problem they might have personally encountered over the previous 6 months. Participants were then asked to respond to questions such as ‘Keeping that stressful event in mind, indicate to what extent you . . .’. An example question drawn from the Problem Solving Subscale is Item 2: ‘Rearrange things around you so that your problem had the best chance of being resolved.’ High scores in a particular style indicate that the participant used a coping style frequently. Participants rated their response to the questions across three dimensions of a lot, a little or not at all. Scoring was undertaken by unit weighting of scale items. Interpretation of scores is aided by scale norms, which eliminate the need for median cut-off points in applications using smaller or more homogeneous samples (Amirkhan, 1990). Internal consistency, test–retest reliability and construct validity have been demonstrated. Strategies related to avoidance were regarded as negative strategies, as suggested by Dunkley and Whelan (2006a).
Impact of Event Scale-Revised (IES-R)
The IES-R assesses symptomatic status over the previous 7 days related to a specific traumatic event across the three domains of post-traumatic stress disorder (PTSD) symptoms, including intrusion, avoidance and hyper-arousal (Weiss & Marmar, 1997). While designed to measure directly experienced trauma, the scale has been used to test secondary symptoms (Bride, Radey, & Figley, 2007). Test instructions request participants to anchor responses to a particular event to ensure counsellors are focusing on therapeutic work with traumatised clients and not a personal event. Participants in this study were asked to relate their experience to the ‘stressful material related by trauma clients’. The IES-R consists of 22 questions measured on a 5-point Likert scale (0 = not at all, 4 = extremely). It produces a total score and three subscale scores for intrusion, avoidance and hyper-arousal. In this study, only total scores were used. An example of a typical item related to the Intrusion subscale is Item 1: ‘Any reminder brought back feelings about it.’ High total scores indicate distress from PTSD symptoms (Weiss & Marmar, 1997). Cut-off points are not used with the IES-R and are not appropriate as the scale was designed as an assessment of symptomatic status following a traumatic experience (D.S. Weiss, personal communication, July 10, 2009). Weiss and Marmar (1997) have reported that the three subscales have internal consistency coefficients ranging from .79 to .92, and test–test reliability coefficients ranging from .51 to .94 .
The Supervisee Form from the Supervisory Working Alliance Inventory (SWAI)
The SWAI assesses the supervisory working relationship from the perspective of both parties and measures the relationship from the point of view of the supervisee (Efstation, Patton & Kadash, 1990). It consists of 19 items rated on a 7-point Likert scale (1 = almost never, 7 = almost always) and contains two subscales: rapport and client focus. A high total score signifies a high working relationship. An example of a typical item related to the Rapport subscale is Item 1: ‘I feel comfortable working with my supervisor.’ The total scores on the SWAI were graded from low to high using mean scores to depict levels of supervisory satisfaction (low: 0–1.4; below average: 1.5–2.9; average: 3–4.4; above average: 4.5–5.9; high: 6–7). Patton and Kivlighan (1997) have demonstrated that the measure has convergent and discriminant validity through significant correlations with the Supervisory Styles Inventory and the Personal Reactions Scale (Revised). Both Efstation et al. (1990) and Wheeler and Richards (2007) have reported that the SWAI is a valid instrument.
Procedure
Written consent from the BoysTown and ethics approval from Monash University was obtained prior to the study commencing. Potential participants were advised of the study through information provided in personal packages that could be collected from a ‘sign-in’ area of the counselling floor by interested employees. Approximately 30 to 45 minutes of participants’ time was required to complete the questionnaires. To ensure participant anonymity, responses were forwarded in reply-paid addressed envelopes to a registered psychologist not associated with BoysTown, who had been recruited to check and remove consent forms from the returned questionnaires prior to passing them on to the student researcher.
Study Design
Survey methodology was used to collect data on the attitudes and behaviours of a non-random sample of counsellors, as the phenomena were not easily obtained through direct observation. It was expected that information provided by counsellors across the range of self-report measures used would most appropriately access the depth and breadth of information required to enable comparative consideration of this group of counsellors with those of earlier studies into telephone counselling.
Results
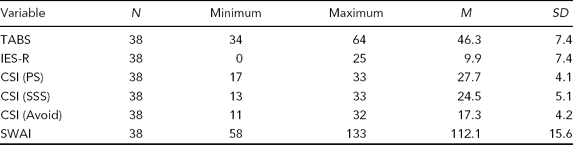
Minimum, Maximum, Mean, Standard Deviations for the TABS, CSI Subscales (PS, SSS, Avoid), IES-R and SWAI-Supervisee Scale
Summary of Research Hypothesis 1
Mean, Standard Deviation, Minimum, Maximum, N, and Correlations for the TABS, CSI Subscales (PS, SSS, Avoid), IES-R and SWAI-Supervisee Scale
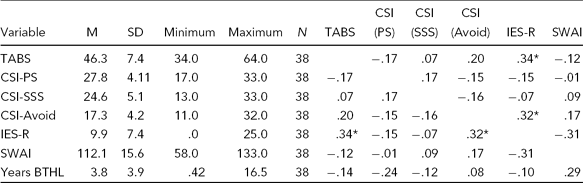
Note: *p < .05.
Summary of Research Hypothesis 2
The hypothesis that counsellors undergoing supervision would have positive coping styles above the average (i.e., Problem-Solving and Seeking Social Support) was met. Table 2 shows that there was a higher than average use of Problem-Solving (CSI-PS normative M = 26, SD = 5), a higher than average use of Seeking Social Support (CSI-SSS normative M = 23, SD = 5), and a below average use of Avoidance (CSI-Avoid normative M = 19, SD = 4).
For the following three hypotheses, correlation coefficients were computed among the measurement scales detailed in the Method section. Using the Bonferroni approach to control for Type I error across the 10 correlations, a p value of less than .005 was required for significance.
Summary of Research Hypothesis 3
Correlations Between variables of Age, Gender, Years Counselling, Years HL, Years BTHL, Trauma Caseload, Weekly Contacts by Trauma Clients, TABS, CSI Subscales (PS, SSS, Avoid), IES-R, Supervisee Scale of SWAI
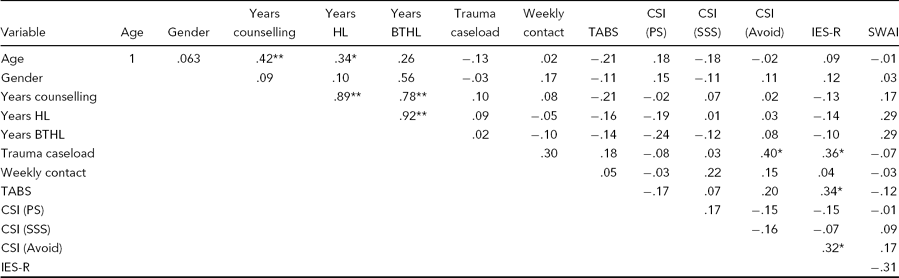
Note: Years HL: Years on a Helpline; Years BTHL: Years on Boystown Helplines; TABS: Trauma Attachment and Belief Scale; CSI: Coping Strategy Indicator; SWAI: Supervisee Form from the Supervisory Working Alliance Inventory; *p < .05, **p < .0.
Summary of Research Hypothesis 4
The hypothesis that supervision and a positive coping style would be significantly positively related was not met as only a weak negative relationship (r = −.24) was observed (see Table 3), with the relationship between Supervision and Seeking Social Support (r = −.12), and Supervision and Avoidance (r = −.08) producing negligible relationships. This was an unexpected result as it was assumed that supervision would have had some impact on the development of a more positive coping style.
Summary of Research Hypothesis 5
The hypothesis that Strength of Working Alliance (SWAI) with a supervisor and VT tabs would be significantly negatively related was not met (r = −.12), although it was in the expected direction (see Table 3).
Summary of Research Hypothesis 6
The hypothesis that there would a significant positive relationship between the SWAI with the supervisor and positive coping style was unsupported, (CSI-PS; r = −.01) and (CSI-SSS; r − .09).
Discussion
This study presents a further attempt to clarify the relationship between supervision and the mangement of vicarious tramutisation. The central assumptions were that (1) supervision would normalise the prevalence of vicarious traumatisation and increase the level of positive coping styles, and (2) the relationship between supervision and vicarious traumatisation and supervision and positive coping styles, and strength of supervisory working alliance and vicarious traumatisation and positive coping would be significant. If the data suggested that the answer to the first assumption was confirmed, the same cannot be said of the second assumption.
Overall, the findings from the present study added to the small body of literature related to the wellbeing of counsellors working in telephone and online environments, as the data suggested that with support from ongoing supervision the group of telephone and online counsellors maintained average levels of VT and more positive styles of coping. However, the relationships between supervision and vicarious traumatisation and positive coping styles, and strength of supervisory alliance, vicarious traumatisation and positive coping style were not significant. Before examining the reasons why significance did not occur it is important to examine how the findings from the present study are in line with previous research.
The average VT scores and low trauma scores in the present study are similar to those of Dunkley and Whelan (2006a), but lower when compared to an earlier study conducted by Mauldin (2001). Dunkley and Whelan (2006a) suggest this may be due to Mauldin's use of the IES instead of the IES-R, a modified version structured to measure all three components of PTSD (hyper-arousal, avoidance and intrusion), rather than just the two contained in the IES. It may also be that Mauldin's larger focused sample (i.e., 98 sexual assault workers), compared to Dunkley and Whelan's smaller (range n = 9 to 15) and more wide-ranging samples of trauma counselling (i.e., death of a young child, life-threatening illness and violence), may account for the difference.
Further to this point, while scores in the present study on the IES-R were low (M = 9.9, SD = 7.4) they were not as low as those reported by Dunkley and Whelan (2006a; M = 9.21, SD = 10.36). However, when Dunkley and Whelan outcomes are broken into different trauma areas, the difference in mean scores (domestic violence Helplines mean = 6.46; child death Helplines mean = 13.56) becomes obvious, suggesting that levels of counsellor trauma may differ according to the type of client trauma experienced. Furthermore, although BoysTown counsellors conducted 50,979 counselling sessions, only 44% involved working with trauma clients. It may be that calls that did not involve trauma clients assisted in moderating the effects of vicarious traumatisation. However, at this point in time this possibility is best seen as a theory awaiting evidence.
The unexpected result that supervision was not significantly positively related to positive coping styles could be related to a possible mismatch between the supervision provided and that needed by the BoysTown counsellors. Given that BoysTown counsellors have an almost equal split of trauma and non-trauma clients, it is possible that there is a perception by the counsellors that the style of supervision does not quite address the unique set of problems created by working with the two different types of clients. Again, this interpretation needs to be reserved as it stands only as a potentially productive direction for further research.
The lack of a significant relationship between counsellors who had a stronger working alliance with their supervisor and vicarious traumatisation in the present study contrasts with the findings of Dunkley and Whelan (2006a), who observed that as the supervisory relationship strengthened so the reporting of vicarious traumatisation diminished. Regardless, counsellors in the present study did report an overall positive experience within the supervisory relationship, as the overall mean on the SWAI (M = 5.9) was toward the higher end of the scale (in a range of 0–7), going some way to explaining the maintenance of vicarious traumatisation within the normal range as measured by the TABS, and lower levels of trauma symptoms as measured by the IES-R.
Finally, and perhaps not surprisingly, in the present study a strong positive relationship (r = .40) between trauma caseload and negative coping style measured by the CSI (Amirkhan, 1997) and a moderate positive relationship between trauma caseload and VT (r = .36) measured by the IES-R (Weis & Marmar, 1997) was found. These outcomes are in line with findings that negative coping styles and increases in VT are linked to large caseloads of trauma clients (Arvay & Uhlemann, 1996; Brady, Guy, Poelstra, & Brokaw, 1999; Chrestman, 1999; Kassam-Adams, 1999; Schauben & Frazier, 1995; see Bride, 2004 for review).
The lack of statistical significance in the present study with respect to supervision and vicarious traumatisation also can probably be attributed to the small sample size, and the correlations seem to support this conclusion. Regardless, the ‘take home message’ that regular supervision attenuates the affects of VT on counsellors has probably not been diminished by a lack of significance in this instance. What is not clear is the effect size that a larger study might have provided. For example, a larger sample would have allowed the participants to be categorised according to the number of supervision sessions, allowing between-group analyses of the effect of supervision. In this way it could be established whether the effects of supervision are maintained over time or whether, with extended experience with trauma clients, the effects of supervision are moderated. Arguably, the variables supervision and counselling experience may always be difficult to disentangle; therefore, the impact of supervision may represent a composite effect of supervision and counsellor experience. While use of a control group may have gone some way to addressing this limitation, this was not an option in the present study as all BoysTown counsellors undergo compulsory supervision.
The overall pattern of results from this investigation suggested that vicarious traumatisation seems an inevitable consequence of counselling those in emotional distress. Regardless, it appeared the participants had been advantaged by BoysTown supervision in two ways: first, mandated supervision had normalised their levels of VT; and second, they were able to use more positive coping styles. A possible third advantage is that ongoing supervision allowed regular monitoring of the number of trauma clients each counsellor worked with as the size of a counsellors’ caseload was linked to their reported levels of vicarious traumatisation and their ability to cope with the accumulated effects of vicarious traumatisation.
Footnotes
Acknowledgments
The authors would like to thank Alan Richardson from Queensland Institute of Technology and Kathleen Ellerman-Bull from BoysTown who provided assistance during the data collection period.