
Abstract
Theoretical models of psychiatric disorders are diverse, as are the empirical measures used to test them. Multidisciplinary efforts have begun to encourage a freer exchange of information - resulting in a more Integrative Neuroscience 1 across disciplines, including the integration of theoretical models in psychiatry.
Empirically, however, there is a paucity of consistent and specific findings in neuroimaging, psychometrics and genetics. This lack of consistency may be influenced significantly by the methodological variability across research facilities.
In neuroscience alone, more than 60 000 neuroscientists and 300 specialist journals generate a plethora of poorly related datasets. In psychiatry there are hundreds of studies showing possible distinctive patterns of brain dysfunction, but they have been undertaken in relatively small datasets (sample sizes of less than 30). Such small subject numbers preclude proper account being
taken of the inherent intersubject variability in human brain function and behaviour. It may be myopic to continue to generate large numbers of such small study outcomes, without some commensurate evaluation of the relative amount of variance explained by the different measures, as well as the sensitivity and specificity of these findings across different psychiatric disorders. The lack of integration across studies also means there is no consistent and widespread platform from which to evaluate the efficacy of medication in these disorders. The present paper focuses on the potential use of neuroimaging-psychometrics-genetics databases in psychiatry and outlines the specifics of the first standardized database.
Two recent articles in Nature 2 and Science 3 have highlighted the need for neuroimaging databases but they emphasize the variables that have limited their development. The Nature article outlines the difficulties in obtaining a consensus among scientists about what data to collect, the difficulties in technical collation of brain data and the reluctance of researchers to embrace data sharing. The Science article emphasizes the difficulty in deriving standards and in developing interoperable databases.
These obstacles have begun to be overcome in neuro-science and to be implemented in a range of database architectures.
FLEXIBLE AND DISTRIBUTED DATABASES
Neuroscience databases have over the past decade begun to be established as part of the emerging field of ‘neuroinformatics’, 4 which deals with information as diverse as microanatomy, receptor distributions, single cell recordings, drug effects and computer science interoperability among databases. These databases have mainly been established to acquire data in a flexible manner and to store the data in a distributed fashion. This flexibility accommodates the rapid pace of change in neuroimaging technologies, as well as the highly specialized interests of individual researchers and the vexed issue of control over individual researchers’ data. These databases have additionally provided the catalyst for
significant interest among neuroscientists in sharing neuroscience data and analytical tools. The exchange of neuroscience data and tools between groups affords the opportunity to re-analyse previously collected data in different ways, encourage new neuroscience interpretations and foster otherwise uninitiated collaborations, and to provide a framework for the further development of theoretically based models of brain function. Data sharing will ultimately reduce experimental and analytical error. Many small Internet-accessible database initiatives have been developed, and specialized analytical software and modelling tools are distributed within different fields of neuroscience. 5
STANDARDIZED AND CENTRALIZED DATABASES
The present article outlines the potential advantages of a fully standardized and centralized approach to databasing, as exemplified by the first standardized International Brain Database. Our interest is in psychological and psychiatric assessment and so our database goals are limited to human data of the kind commonly employed in neuropsychology, psychophysiology and brain imaging. However, even within these constraints, there is still plenty of scope for incompatibilities across laboratories. Only by strict standardization of all variables across participating laboratories (where each subject carries out precisely the same protocols), can we perform direct comparison of sensitivity, specificity and treatment efficacy among all disorders studied.
Apart from the core data, there are numerous less obvious standardization issues such as informed consent, confidentiality, paradigm consensus in data acquisition, technical standardization, authorship credit and central analysis.
Database projects are more complex than single hypothesis studies. Therefore, subjects need to be informed of this approach in a clear and transparent manner, in order to give their consent to participate. The subject ethics information form makes it clear that many scientists may explore this data in different ways. Parts of this database will be provided freely to selected scientists in the fields of neuroscience and psychiatry research. It is also made explicit that possible commercial uses might emerge from the subjects’ data. Funding for this standardized international database was from a commercial source (http://www.BrainResource.com) and so ownership of the data had to be made as explicit as possible.
Confidentiality is essential and so this database is ‘de-linked’: subjects are issued an ID number and their name is not kept with their data in the centralized database facility.
Consensus about the choice of psychophysiological, brain structure/function and cognitive (psychometric) paradigms was complex and difficult. A further constraint was that the test battery needed to be relatively short, to avoid subject fatigue. A suite of paradigms were selected that tap the brain's major networks and derive a ‘profile’ of activities (rather than focus on a few specialized domains of function). Highly credentialed consultants, who had exceptional experience within a particular paradigm, were employed to resolve the most robust, reproducible and generic version of that paradigm to be employed in the database. This profile approach, and a focus on robust paradigms, helped to resolve a consensus among participating scientists and clinicians.
Figures 1 and 2 summarize the psychophysiological, brain structure/function, cognitive paradigms and genetics that were chosen to profile the brain's core networks and functions.
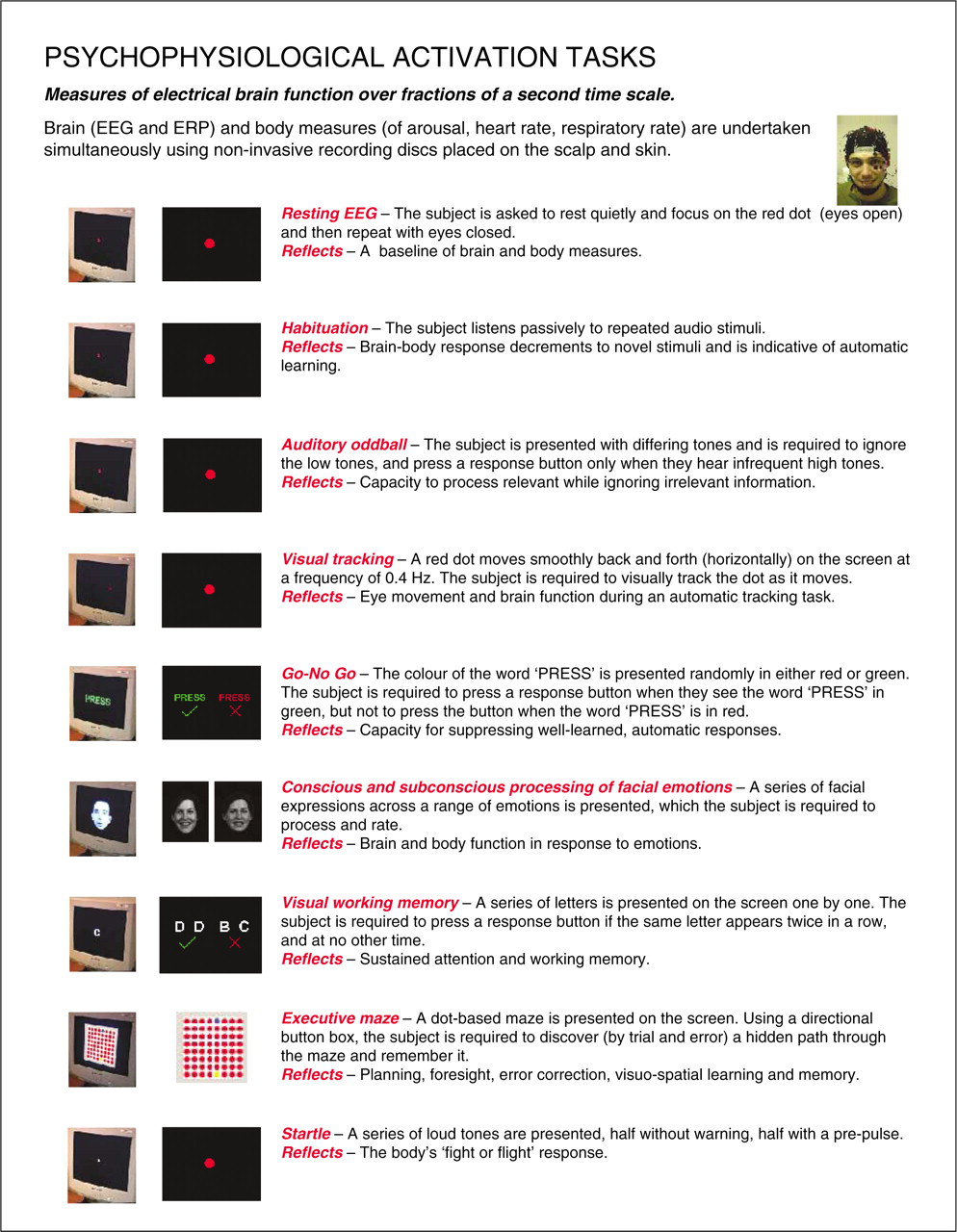
Psychophysiological activation tasks selected to tap the brain's core networks and processes.
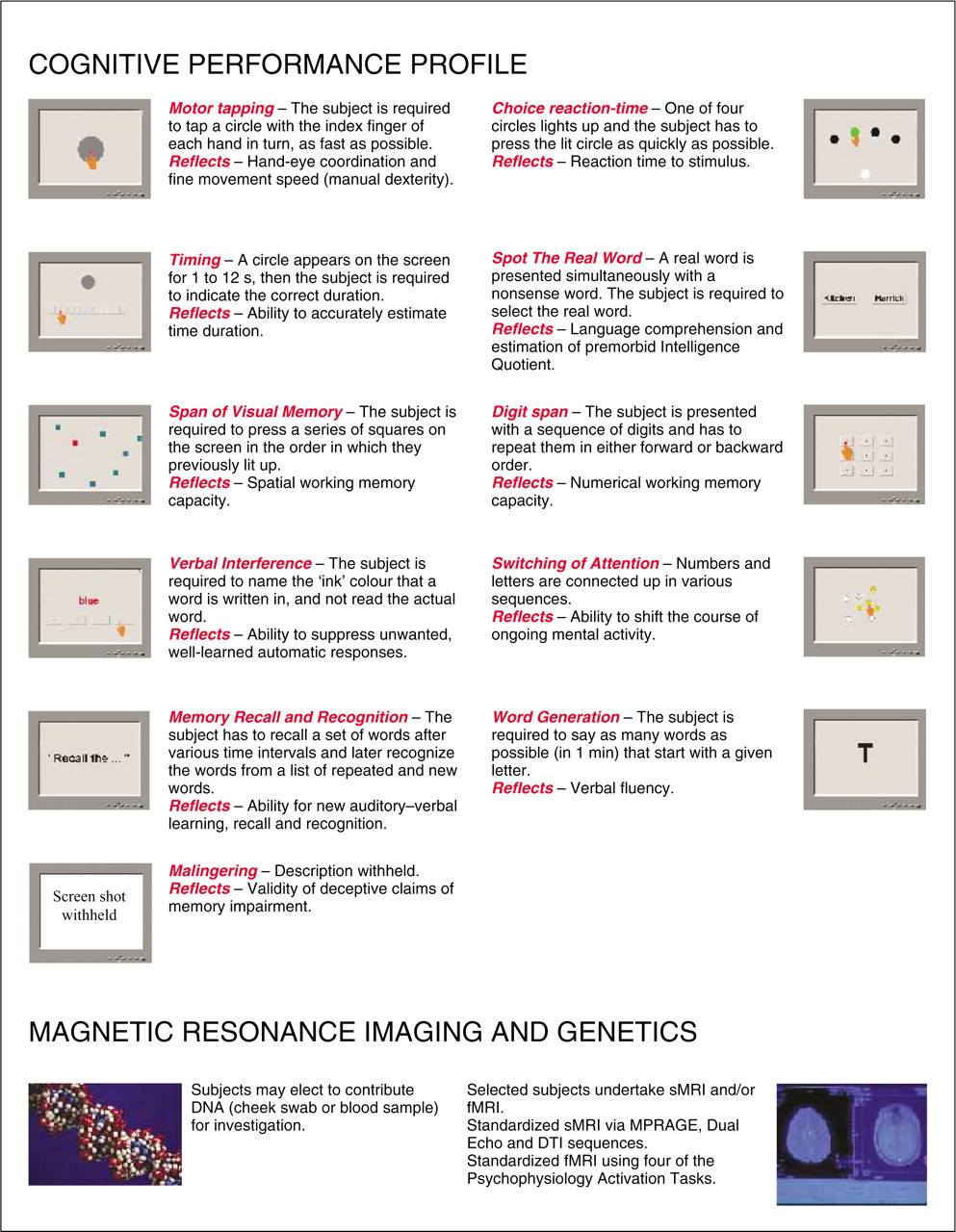
Standardized profile of cognitive performance, structural magnetic resonance imaging (sMRI), functional MRI (fMRI) and genetics. DTI, diffusion tensor imaging.
Technical standardization required an agreement on precisely which equipment to use for every paradigm. To ensure that the task instructions were delivered in an identical fashion, a recorded voice reading the task instructions are replayed in each laboratory through identical headphones. All data recording hardware and software are likewise identical in all laboratories.
Twenty-two demographic questionnaires were also selected by the consensus approach. These questionnaires are undertaken via the internet using the subject's ID code prior to the subject visiting any of the brain function laboratories. The web-based screening questionnaires encompass anxiety and depression (using the Somatic and Psychological Health Report (SPHERE) 6 ), medical, psychiatric, drug and alcohol history, sleep patterns, mobile phone use, early life stress and history of trauma.
A fundamental fear in a ‘data hugging’ scientific community is that credit will not be appropriately assigned to the contributing researchers. A scientific advisory committee was therefore set up to explore the best model for maximizing the scientific outcomes in the fairest manner.
A central analysis facility allows the control of standardization to be maintained with respect to artefact rejection, outlier removal, details of analysis etc. It has also allowed unprecedented efficiencies in processing huge amounts of disparate data. The analysis engine is set up in a modular and flexible manner, such that new methods can be readily incorporated and the amount of variance explained by the new method compared to the existing ‘gold standard’. Most importantly, examination of potential interrelationships among the variables is readily achievable, by having all the data in one database thereby subserving the overarching goal of ‘integrative neuroscience’.
Access to outcomes from new analysis methods developed within the consortium was a significant factor in attracting scientists to participate in this database. An increasing number of researchers are coming to the view that our limited understanding of imaged brain function may not have as much to do with what we have measured as with the level of sophistication with which we have analysed these complex signals.
New mathematical, signal processing and physics models extract more fundamental information from the measures of overall brain function. I provide three different examples of new methods developed within the international brain database consortium, which illustrate the advances that helped galvanize participation in this database.
EXAMPLES OF NEW BRAIN ANALYSIS METHODS
The first example is in the field of signal processing. There has been increasing evidence that synchronous phase of high-frequency (40 Hz gamma) oscillations are an important coding method in the brain. The earliest evidence of this arose at the microscopic scale from studies in the cat visual cortex by Singer and Gray. 7 Synchronous gamma activity has since been related to cognitive processing in humans, and has been observed across different scales of the brain, including the whole brain level. 8 This new measure may reflect one way in which the brain ‘integrates’ activity from the plethora of its ongoing parallel processes.
As a second example, numerical models and simulations of the brain are able to elucidate possible mechanisms underlying brain function, by capturing the essence of the mass of neuroscience details and determining their interactions in an explicit manner. In a brain with 100 billion highly interconnected neurons, only models treat massive network interactions realistically and can be expected to generate plausible predictions. An extraordinary brain simulation has been developed by Jim Wright from the University of Auckland, with significant reformulation of his model by Robinson et al. from the School of Physics and Brain Dynamics Centre, at the University of Sydney and Westmead Hospital. 9 In this model there is no attempt to reproduce the firing patterns of individual neurons. Instead it aims to model the collective behaviour of large ensembles of neurons, matching the whole brain scale of electroencelphalograms (EEGs). The parameters in the model are biologically realistic, including details about how neurons are interconnected over short and longer range, the rate of firing of network activity, the speed of conduction of electrical activity in the brain, the effect of various excitatory or inhibitory neurotransmitters and modulation of overall brain stability. The model output is matched to real data from the international database, which allows interpretation of dysfunctional mechanisms in health and disease, according to the realistic physiological variables in the model. There is the potential for this numerical simulation to add anatomical or neurochemical parameters of relevance to any psychiatric disorder.
The third example concerns the value of examining interactions in concurrently recorded brain and ‘body’ (autonomic nervous system) activity. We know that autonomic arousal modulates brain function in a significant way. For instance, when we are unexpectedly threatened, our body responses help to get us out of danger rapidly. The first studies to simultaneously record brain network responses (using functional magnetic resonance imaging (fMRI)) and autonomic arousal to threat perception, have shown that threat-specific networks are engaged during high levels of arousal but that different networks are active during lower levels of arousal. 10 Classifying individual responses according to instant levels of arousal has the potential to elucidate subtle brain disturbances in psychiatric disorders such as schizophrenia, posttraumatic stress disorder (PTSD), attention deficit-hyperactivity disorder (ADHD) and anxiety disorders, in which arousal modulation is disturbed.
TESTING INTEGRATED PSYCHIATRIC MODELS WITH NEUROIMAGING
Over the past two decades we have seen a paradigm shift from a narrow fixed modular conception of the brain (specialized ‘centres’), to one that consists of multiple modules, which are widely distributed, and interact in parallel.
When we juxtapose some of the most commonly cited whole brain scale biological models across different disciplines for example, the models of Luria 11 and Goldberg 12 (neuropsychology); Gray, 13 Posner and Petersen 14 (cognitive psychology); LeDoux, 15 Sokolov, 16 Halgren and Marinkovic 17 (physiology); Damasio 18 (neurology); and Schorre 19 (psychiatry) a pattern emerges of the overall flow of information processing in the brain (although the extraordinary extent of parallel and interconnected processes across scale should never be underestimated). Sensory input-motor output is processed from the back (posteriorly) to the front (anteriorly) of the brain. This core input-output (thalamo-striatal-cortical-cerebellar) network is underpinned by core decision-making about stimulus significance (particularly in the limbic system) and modulated by arousal and monoamine activity. A core aspect of elucidating stimulus significance is thought to occur by brain networks comparing the extent of familiarity:mismatch between incoming and stored information (the extent of mismatch triggering either defence, orienting or more complex adaptive processing). Ongoing inhibitory and excitatory activity is underpinned by neurochemistry over different time scales: rapidly via gamma-aminobutyric acid (GABA) and glutamate activity (10 ms time scale), over seconds via monoamines and over longer time scales with neuropeptides. Relatively ‘automatic’ subcortical survival processing is crude and rapid, whereas detailed relatively ‘controlled’ processing is undertaken more slowly and engages widespread subcortical and cortical networks. Disorders in psychiatry may reflect maladaptive magnifications of any of the processes in this continuum, with the added complexity of subsequent over-processing or under-processing of information as an adaptive response to an underlying instability.
Integration of temporal and spatial information allows testing of such adaptive dynamical models of instability in psychiatry, including in a standardized database with careful selection of neuroimaging technologies that provide complementary spatial and temporal resolutions of brain structure (MRI) and function (fMRI, EEG, event-related potentials, single photon emission computed tomography). 20
An ongoing caution is the ease with which a researcher can be overwhelmed by the sheer volume of data in a database. Therefore, theoretically driven exploration of the data via a priori directional hypothesis-testing is essential as the core approach to all analyses (with some judicious data mining with appropriate statistical controls to shape future hypotheses).
A goal of the database project is for clinical researchers around the world to add their patients to the continuum of disorders under investigation. As many psychiatric groups as possible will be studied employing standardized clinical, composite international diagnostic interview and other diagnostic instruments considered essential to diagnosis in each disorder. Data from seven disorders are currently being acquired to examine the sensitivity and specificity of findings. Patients from different disorders will also be studied longitudinally (including before and after medication), to examine developmental dynamics, as well as the efficacy of medication and adaptation of brain function and behaviour over time.
RESULTS FROM A STANDARDIZED LOCAL DATABASE
Results of significant findings in four psychiatric disorders in a local independent standardized database in The Brain Dynamics Centre at Westmead Hospital and University of Sydney (http://www.Brain-Dynamics.net), provide an ‘exemplar’ for extending this standardized approach to the International Database. A summary of significant results across four disorders is shown in Figure 3, which illustrates the potential for specific findings to be elucidated across psychiatric disorders.
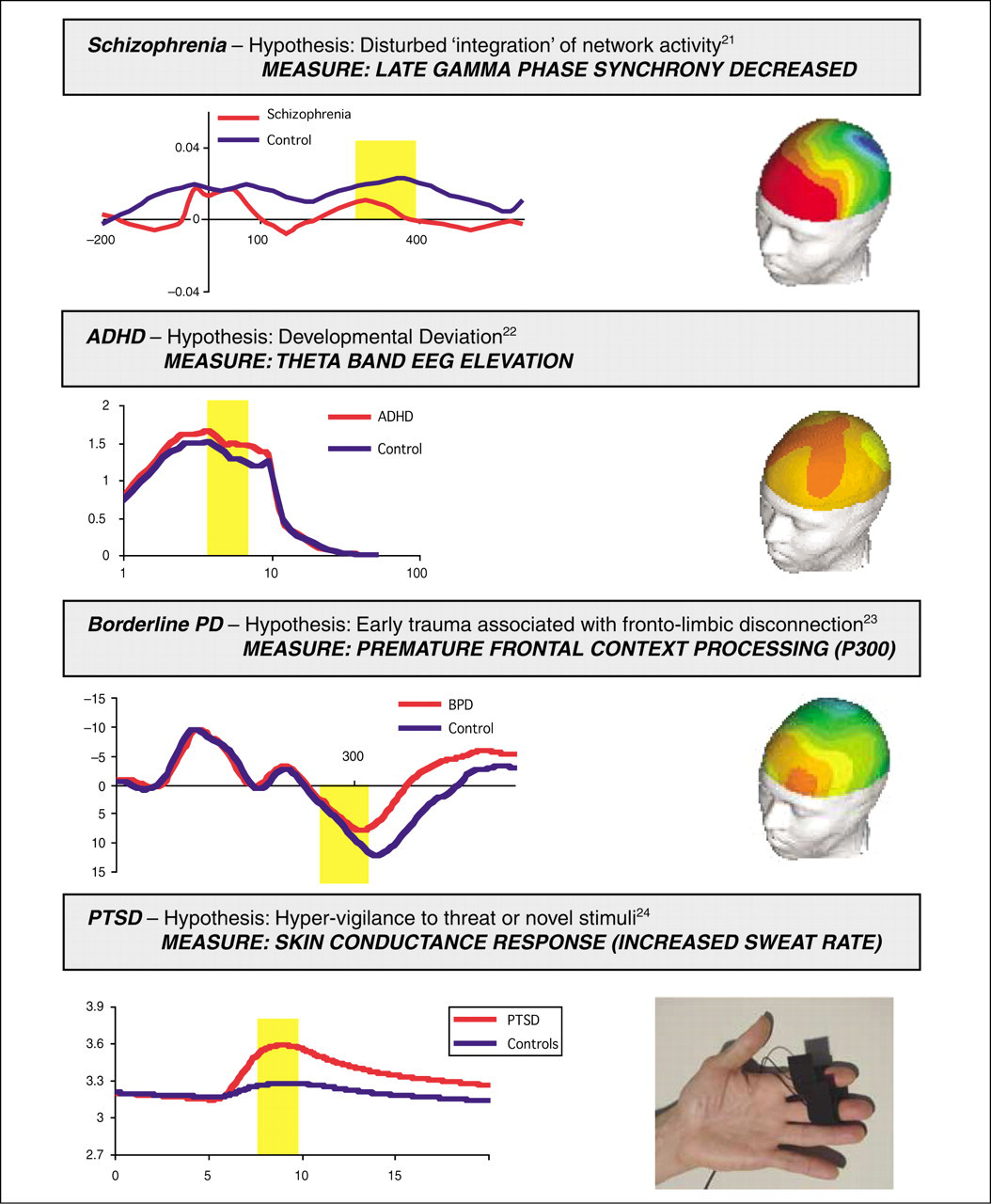
Clinical group examples from a standardized database at the Brain Dynamics Centre, Westmead Hospital (http://www.Brain–Dynamics.net). Waveform graphs on the left depict temporal aspects of brain function or arousal and images on the right show the spatial distribution of statistically significant findings.
CONCLUSIONS
This first standardized international brain database demonstrates that it is possible to obtain a consensus on the standardization of paradigms, and on the protocols and analyses required to tap the brain's major networks using neuroimaging, neuropsychological and demographic information. This integrated frame of reference provides an exemplar of an ‘evidence-based’ evaluation of the sensitivity/specificity of findings and the efficacy of treatment response in relation to brain-body function and cognition, in a range of psychiatric conditions.
Footnotes
Acknowledgements
Chris Rennie, Lea Williams, Daniel Hermens, Donna Palmer, all collaborators in The Brain Dynamics Centre and the International Brain Resource Database.