
Abstract
Closure of psychiatric hospitals has engendered much debate. There is a growing body of literature resulting from such closures. Lamb [1] in a lecture has pointed out the need for deinstitutionalisation to be clinically driven rather than by pre-conceived ideology. Bachrach [2] discussed the need to espouse a bio-psycho-social and humanistic approach coupled with the provision of adequate resources. In a limited survey conducted among community homes and long-stay hospitals in London, it was found that the most disabled were still living in hospitals and received the poorest quality care. Whilst there were no overall differences amongst the community facilities, they noted the importance of staff training and morale in order to improve quality of care [3].
The team for the assessment of psychiatric services (TAPS) has longitudinally followed patients for five years following closure of two long-stay psychiatric hospitals in England. They found that there was some improvement in the patients. More importantly they were living in less restrictive conditions in the community and their appreciation of the freedom tended to increase over the years. However, they cautioned against generalising these findings [4]. In similar follow-up studies from the US [5,6] and Finland [7] the patients' preference for living in the community is noted [5,7]. It is of interest to note that another study from the UK confirms this view and subjective ratings showed improvement in other areas of social activity but patients themselves did not perceive it as such [8]. From the TAPS studies it is evident that there is limited change in patient psychiatric symptoms [9]. Community residences established under the resettlement program served as relatively stable homes for the majority of patients [10].
From these studies it is evident that patients enjoy the relative freedom of living outside the hospital but their psycho-pathology has not altered appreciably. There appears to be a paucity of published information regarding the process or outcome of hospital closures in the Australasian context. We have outlined a process that underpinned the closure of a long-stay ward and the outcome, primarily in terms of their psychiatric status and their accommodation five years post discharge. The ward was part of a stand-alone psychiatric hospital built in the mid-1950s in rural Victoria.
The Hospital accommodated over 250 patients including the chronically mentally ill and the intellectually disabled. There was a gradual ‘downsizing’ of the facility during the mid-80s leading to its eventual closure in the early 90s. The hospital was mainstreamed and a change from services provided around institutional care to a more community-oriented model of integrated health care was implemented. We specifically address the closure of the remaining long-stay unit in the context of a hospital closure. This paper examines the processes involved and the outcome five years onwards.
There were 11 males and 6 females whose ages ranged from 22 to 63 years with an average 15-year history of institutionalisation. The majority had treatment-resistant schizophrenia or chronic psychoses. There were those without an Axis I diagnosis. Many suffered from concomitant physical illnesses. They also had developed idiosyncratic coping styles moulded by prolonged institutional care.
CONSULTATIVE PROCESSES AND STAFF RETRAINING
Prior to closure extensive consultation between administration and clinical staff took place and most importantly clients and families were involved. Throughout the period of moving to a group home, clients were apprehensive but thought it would be a better option. Inpatients treated under the mental health act were placed on community treatment orders. Family members were given a patient hearing and illness education and explanations were provided according to their questions and commensurate with their understanding. Informal carers, families and friends were encouraged to accept a greater degree of responsibility and were provided with continued updates of the progress. Medication management and compliance training took place in conjunction with the patients. In order for patients to be nearer to their families liaison was established where possible, with other regional psychiatric services for transfer of those patients who were out of area to their area of origin.
Inpatient nurses were offered an opportunity to obtain employment in the community, move to the acute facility to voluntary departure packages (VDPs). The staff had continuing education throughout the transitional phase. The main focus of training was a humanistic model that provided an appreciation and greater understanding, thereby developing growth and independence with respect to each individuals' rights. In many instances it appeared that staff were resistant to the ‘news’ ethos.
CLOSURE PROCESS
At the outset two patients were discharged, one was transferred to her region of origin and one to a high security unit in Melbourne. The others were relocated in suitably modified hospital houses. The complex consisted of five units and an office situated within the hospital campus but on its perimeter. They were three bedroom houses. Each unit housed 2 or 3 residents. The clients were grouped according to their illness profile, mutual compatibility and degree of disability. The units themselves were classified as high, medium and low dependency in terms of the need for support and supervision. Staff were rostered to each of these houses according to the need with more experienced staff being allocated to the houses that required greater supervision.
Each resident was treated as an outpatient and was assigned a case manager from amongst the multi-disciplinary community team. Each patient had an individualised rehabilitation program which focused on activities of daily living. Whilst they were encouraged to prepare their own meals, there was an option of obtaining hospital food. Each unit functioned as a miniature household with individual responsibilities. They had ongoing medication reviews including introduction of clozapine for treatment-resistant schizophrenia. Each house was a self-sufficient unit, with safety features incorporated. Local general practitioners were approached for registering these patients. Detailed medical histories and a synopsis of their psychiatric situation was submitted and physical care was transferred to the general practitioner. Case management by the community team meant that in addition to the staff on the site there was further access to the psychiatric team which included access to the service on a 24-hour basis for all of the patients who remained within the area. The psychiatrist reviewed all patients as required.
Over a period of three years suitable accommodation options were explored. All but two of the thirteen clients were found alternative housing facilities. Hence of the original sixteen, six are living in their own home/home environment and they receive varying levels of support by psychiatry services and other non-governmental agencies. Another six are living in supported accommodation (nursing home/hostel type). One is in a high dependency psychiatric unit, one died of natural causes and the other following an accidental overdose of heroin. Two remaining in a house staffed by the public psychiatric services. Figure 1 outlines the process.
Flowchart of the closure process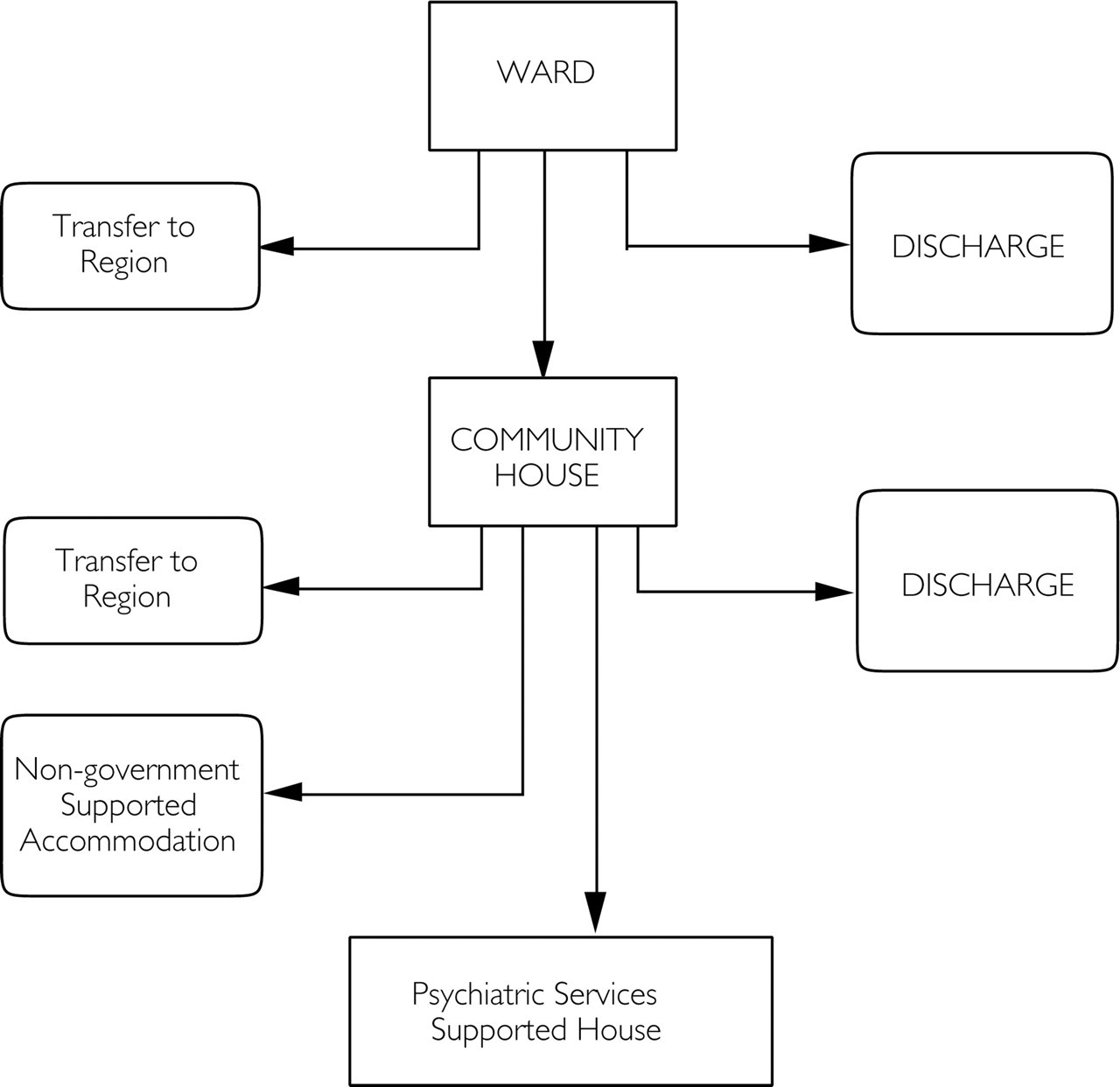
One adverse event that occurred when the patients were moved to the houses was when a client was found in another house. This was reported in the local press and the police were involved in his return [11]. One other major incident took place when an unprovoked attack took place on a member of staff.
DISCUSSIONS AND CONCLUSIONS
This study takes a qualitative approach [12]. Our patient population is similar to those described in other long-stay institutions [9]. Except for four patients, the others who are living in supported accommodation are in fact receiving some form of institutional care. Their psycho-pathology has not dramatically changed, with the exception of the clozapine residents. Similar findings have been noted in the TAPS project [9]. Although suicides have been discussed as a feature highlighting a failure of community care for those with chronic mental illness [13] there are several methodological problems related to making such statements [14]. It is worthy of note that none of our patients committed suicide.
Our experience confirms the view that general practitioners are pivotal in the role of providing medical back-up for these patients [15,16]. The importance of training for [17] and the involvement of the nursing profession [6], and the necessity of engaging the carers [18] is well documented. This was paralleled in our study. We felt that a relatively smooth transition from a custodial setting to a less restrictive environment was achieved by a process of planning, extensive consultation, and involvement of families and carers. Both patients and staff had education provided. We utilised resources in the community to take on these patients and to continue to provide them with ongoing professional help in order to care for these individuals no longer living in the community.