
Abstract
INTRODUCTION
Australian psychiatry is a pioneer in the world-wide trend to develop treatment-oriented clinical practice guidelines, but has been unremarkable in disseminating them so that they become widely available to clinicians and consumers. 1 The goals of developing and disseminating evidence-based guidelines are to improve the quality and outcomes of care, stop unnecessary or ineffectual care, and reduce inappropriate variations in practice across systems of care. This is achieved by aligning treatment decision making with a judicious use of guidelines by clinicians, jointly with consumers. 2
In late 1998, the Royal Australian and New Zealand College of Psychiatrists (RANZCP) initiated a project to develop and implement clinical practice guidelines (CPGs) funded by the National Mental Health Strategy and the New Zealand Health Funding Authority. A series of six evidence-based guidelines for providers and users of specialist treatment services are being developed, along with a plan to implement and evaluate the uptake of the guidelines.
Both common and low prevalence disorders are included in the series. The titles include schizophrenia, major depression, bipolar disorder, panic disorder and agoraphobia, anorexia nervosa, and repeated deliberate self-harm. A decentralised approach has been taken in developing the guidelines, each being written by its own multidisciplinary expert group and supported by a national development secretariat.
By contrast, dissemination and implementation planning will have a coordinated, centralised approach that aims to devise diffusion and dissemination strategies for the series as a whole, as well as for planning priority implementation for key recommendations within particular titles. This is not to say that a top-down approach is being taken. Rather, this approach ensures that adequate attention is paid to flexibility, local planning to use the guidelines and that plans to evaluate the uptake of the guidelines can be built into the dissemination and implementation plan from the outset. The guidelines are nearing the final draft stages and decisions about assertive dissemination, as opposed to passive distribution will be made once the series is finalised. This paper provides an overview of the project, in particular, the dissemination planning that the RANZCP is undertaking with other professional bodies and other stakeholders, which takes into account the consultation and pre-dissemination phases of the program.
KEY CONCEPTS
The new guidelines will aim to be evidence-based rather than consensus statements. The term evidencebased medicine is defined as “the conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients”. 3 It means integrating individual clinical expertise, such as the skill and judgement gained through experience, with the best available evidence from systematic research.
Clinical practice guidelines are “systematically developed statements to assist practitioner and consumer decisions about appropriate health care for specific clinical circumstances”. 4 Guidelines distil large bodies of knowledge into convenient formats. Their rationale is to enable a practitioner to make decisions based on the research evidence, while avoiding the need to access bibliographic databases and appraise the literature critically in every clinical circumstance. Evidence-based guidelines contain explicit recommendations about treatments, based on: a systematic appraisal of the evidence about efficacy of the treatment; the potential health outcomes and side effects of the treatment; and consideration of the economic factors in the provision of care.
A number of factors have contributed to interest in guideline development in the last decade. 5 These include:
evidence of wide inappropriate variations in the use of some treatments, and corresponding variations in the costs of health services;
an increasing focus on the quality of health care and the health outcomes attributable to that care;
uncertainty about the effectiveness of new treatments compared with more traditional treatments;
increased interest in methods of disseminating research evidence to clinicians and consumers and concern about unwarranted delays in getting new improved treatments into mainstream practice; and
increasing acceptance of the “evidence-based medicine” approach to clinical practice.
A very important concept is that guidelines be understood as tools to aid decision-making and should be differentiated conceptually from standards, rules, protocols or codes of conduct. 6 They should not be taken to mean that the recommendations must be applied in every clinical encounter. The adoption of guidelines in Australia and New Zealand has not been mandated by policy makers. Rather, they are one strategy among many for promoting evidence-based practice. The dissemination of the RANZCP series will position dissemination in a way that complements and differentiates the role of guidelines from other policy and quality effectiveness initiatives.
INTENDED USERS OF THE GUIDELINES
Guidelines are published in a variety of lengths, styles and formats depending on their purpose and target audience. The RANZCP project decided that the series should target a readership wider than psychiatrists and consumers to include non-medical disciplines working in secondary and specialist mental health care. The disciplines being consulted are psychiatrists, clinical psychologists, social workers, occupational therapists and mental health nurses. Dissemination planning will take into account the different needs of these audiences.
The series is not intended for general practitioners. This approach is consistent with cautions against applying specialist guidelines in primary care in recent reviews of primary care guidelines. 7 , 8
Patient versions of the guidelines are being developed in line with the NHMRC recommendations on quality guideline development 9 and to improve patient-doctor communication. These versions are intended to increase treatment adherence and to aid education about self-care. If guidelines are sufficiently well written, however, they should also permit clinicians to work directly from the clinicians' guideline in consultations with patients. A range of formats appropriate to the consultation setting are likely to be provided.
Guideline dissemination need not mean only the active use of hard or electronic copies. Strategies such as posters for the waiting room can inform patients that the guidelines are available. This may help demystify mental health problems and clarify the goals of treatment, but also enable patients to request evidence-based treatment approaches from their mental health clinician. Dissemination strategies that target both users and providers of treatment can support the development of a more therapeutic relationship with active partnership by the patient in arriving at a treatment plan. The dissemination of the consumer versions and communications strategies in support of the guidelines will be the subject of a separate dissemination plan to ensure an evidence-based approach to dissemination that is capable of yielding actual use of the titles.
USING GUIDELINES IN PRACTICE
Figure 1 shows how a clinician will make use of a guideline and how it will inform, but not dictate to, the clinician about clinical decisions. Having defined the problem requiring treatment, the clinician may refer to a guideline to obtain information that will assist him or her to determine the most appropriate treatment for an individual with that problem. The guideline should provide clear information and recommendations on:
treatment options;
the outcomes of providing those treatment options;
the evidence supporting those options;
the benefits and harms; and
issues in the cost of that treatment.
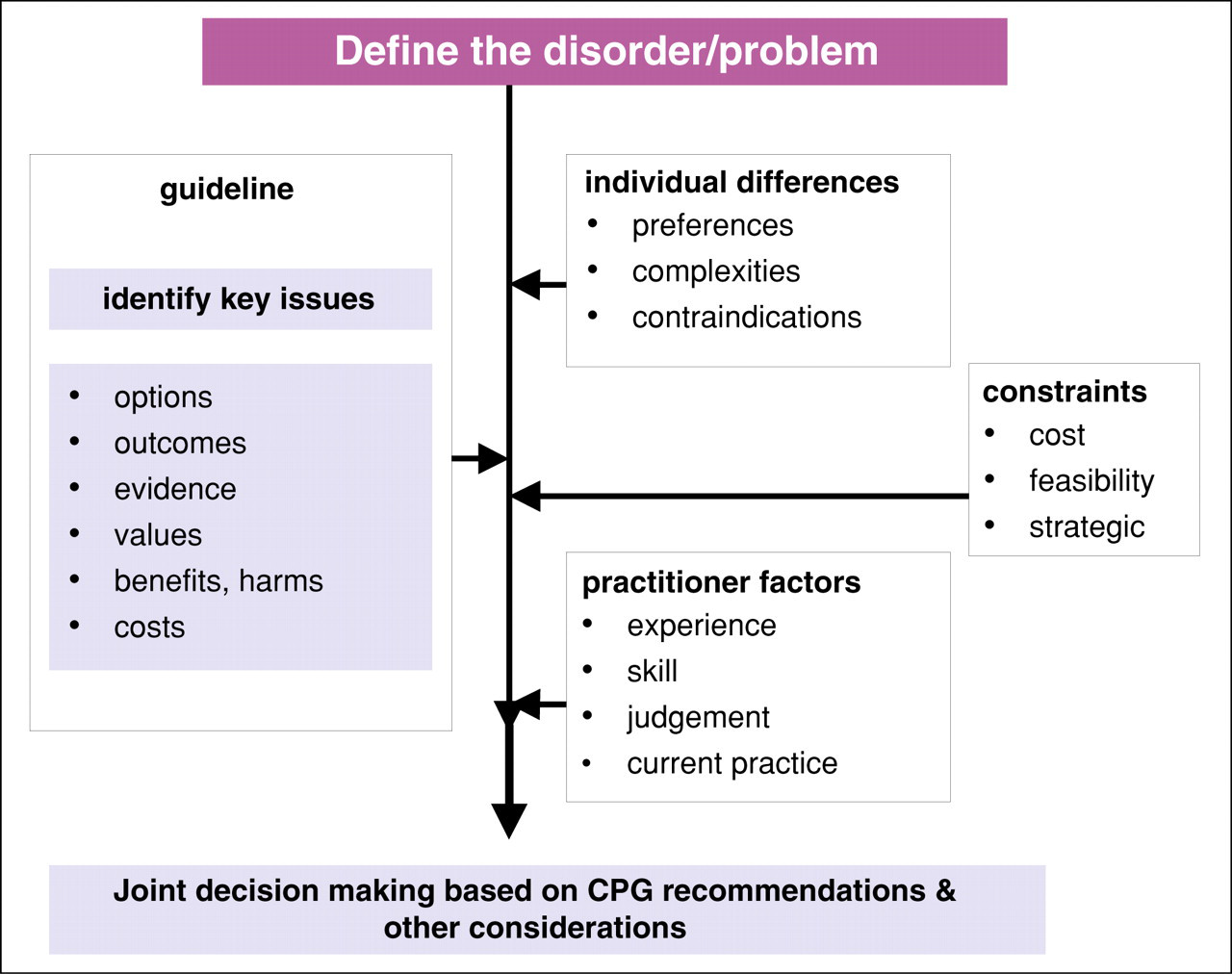
The role of a CPG in clinical decision making.
The clinician can then integrate the recommendations with information about the individual patient's problems, such as their preferences, the clinical complexities of the condition, contraindications to the use of particular treatments, and so on. The clinician will also have to take account of factors relating to their own practice, including their level of experience, their own preferences, and whether or not they have the skills to use the recommended treatments. There may also be other constraints, such as whether the treatment is feasible or economically viable. The clinician, in collaboration with the patient, will then make a decision about the most appropriate treatment to pursue.
ISSUES FOR THE DEVELOPMENT TEAMS
As with the development of standards, guideline developers must decide upon a title's scope, and pitch and agree on what expectations it should contain for achieving particular changes in practice. The guidelines are usually written to reflect either a foundation for good clinical care, or the ceiling of care (best practice). They must make evidence-based recommendations, but at the same time, not disen-franchise clinicians with recommendations that are not feasible to carry out. For example, they should recommend medications that not only work, but also are those that a health system in a particular country can afford to provide. Another example is that they should recommend treatments that are indicated by the research, but in the event that clinicians have insufficient skills in applying the optimal treatment, an alternative should also be given. The implementation plan should address closing any skills gaps so that clinicians can, in time, be equipped to deliver the recommended first line treatment in the majority of cases.
All guidelines represent a tension between what the evidence says, what is current practice, and what practices must stop or otherwise be influenced in order to achieve evidence-based care as a systemwide norm. The RANZCP guidelines will be making recommendations that contribute to identifying or meeting particular public health objectives. In this sense, authors who argue that guidelines exceed their mandate as clinical decision tools, and suggest instead, that they are more instruments of public policy are somewhat correct. They identify the real potential of guidelines as capable of improving whole systems of care if used widely. 10 Guidelines as a technology are part of the building blocks of a health system and, like any clinical resource, may influence change depending upon their content and how they are used. The consultation on the RANZCP series must achieve awareness as to the intended role of the guidelines, and make the goal of dissemination explicit.
While some guidelines in medicine are couched in terms of ‘best practice’, it would be erroneous to think of the RANZCP series as being able to document optimal practice in all cases. They could not cover all clinical eventualities that arise in the care of people who often have comorbid conditions. Instead, they aim to be foundation documents, from which effective practice can begin so that at the outset, evidence informs first line and subsequent treatments. This is not ‘dumbing down psychiatry’. Rather, it is building a solid foundation upon which to base quality clinical practice. Such a foundation is an essential input to all specialist mental health disciplines and could be considered a prerequisite for optimal practice.
ISSUES FOR DISSEMINATION
Guidelines do attempt to standardise care where there is unjustified variation of practice. This variation can be between different clinicians of the same profession in the same clinic, on the management of a particular condition. The public health benefit of addressing variations of care by getting the foundations right should not be underestimated. Unjustified practice variation may erode public confidence in seeking mental health care. The dissemination strategy will emphasise the importance of treatments reaching currently untreated individuals and groups who may benefit from treatment. Ensuring the spread of those treatments and retaining people in treatment so that completion rates can be improved are two significant public health challenges that may improve if guideline implementation were successful. It is entirely conceivable that guidelines could influence consumer, professional and indeed population mental health literacy. 11 All these aspects will be considered in a public health approach to evaluating guideline uptake.
Understanding ‘dissemination’
The knowledge utilisation and dissemination literature often uses dissemination and implementation interchangeably for they are overlapping concepts. The goal of dissemination is to implement or use the guideline in practice. 12 Unfortunately, dissemination is often confused with mere information distribution. The latter is passive and is better understood as predissemination or diffusion, whereas dissemination is active and strategic. It is the positioning, planning and operationalising of health informatics and education programs to ensure the uptake of the guideline recommendations into practice. 13 Predissemination prepares the ground for effective dissemination. 14
Pre-dissemination quality checks
The pre-dissemination phase of the RANZCP project will use Norheim's (1999) criteria, 15 as one of a number of quality checks for judging each title's readiness for dissemination:
Validity - is the guideline scientifically valid (i.e. is it right?)
Importance - is what the guideline recommends worth doing? (does it justify dissemination?)
Acceptability - what is the legitimacy, transparency and trustworthiness of the development process?
Validity is being addressed as the core business of the development teams. The RANZCP consultation explicitly addresses this issue to ensure the widest scientific scrutiny of the guidelines' recommendations. The RANZCP approach has ensured appropriate composition of the teams through representation from:
consumers and carers who identify with the clinical areas; clinicians from a range of relevant disciplines, experienced in that clinical area; and experts in health care planning and management, health economics and evidence appraisal.
Norheim defined importance to mean that both professional and consumer values should be contained within guideline recommendations, as well as public health importance. The literature shows that a perception by clinicians that their individual clinical practice is insignificant in influencing public health goals to be a potential barrier for the uptake of guidelines. 16 The titles that promise the greatest public health impact, if disseminated first, may address any such perception by clinicians.
Finally, it is critical that a guideline is acceptable as well as scientifically valid and practically important. Acceptability is more or less the reputation of the guideline as a whole. Its integrity hinges upon how readers understand the development process and many of the key concepts that define guidelines as different from other resources. The series will include clear statements about the development processes that justify placing trust in a guideline as opposed to any other resource claiming ‘evidence-based’ status.
Common pros and cons of guidelines
Our consultation has detected similar concerns to guideline introduction that is described in the evidence based medicine literature. These will now be discussed.
1. “Guidelines don't work”
There is sufficient evidence in other areas of medicine to suggest that potential benefits may accrue if guidelines are routinely used in clinical practice. 17 The principal anticipated benefit is an improvement in the quality and consistency of care, which has been shown to lead to health improvement and other outcome in numerous international studies and meta analysis.
2. “Guidelines don't work in mental health more particularly”
It is premature to conclude that guidelines don't work in mental health since only one large study in the United Kingdom 18 on primary care depression has been undertaken, the results of which were pessimistic. There is virtually no reliable international research evaluating guideline uptake in specialist settings by psychiatrists or other specialist mental health workforces. 8
3. “Guidelines will ration care and limit treatment choice”
The concern that guidelines may limit the right of consumers to exercise choice between available treatments has been refuted by the NHMRC in its own statement of intent in relation to guidelines in Australia, where they state that Australian guidelines are not a rationing device. 19 However, it is a fundamental ethic of medicine and health care to be concerned both about the quality and distribution of services so that scarce resources are used equitably.
4. “Evidence-based psychiatry is premature due to weak evidence”
There is literature that expresses the views that evidence-based psychiatry is premature as a doctrine. 20 It is indeed legitimate to be vigilant about evidence quality and some skepticism about EBM is possibly healthy. But given that less than 30% of medicine is based on sound evidence 21 psychiatry is perhaps not faring so badly. The point is, that there is sufficient evidence for developing confident treatment recommendations for most conditions but it is entirely insufficient and inappropriate that it does not more rapidly get adopted into mainstream practice.
“Guidelines as medico-legally threatening”
There is a literature on medico-legal implications of guidelines. Courts have used them to both defend and prosecute doctors and affirms that they are more often used defensively. However, providing reasonable and skilled care, has been shown at law not to equate directly with the use of guidelines. 22 , 23
6. “Guidelines as dumbing-down or threatening the patient-doctor relationship”
Fears about ‘cookbook medicine’ are not new and in part relate to concern that guidelines are based only upon outcomes for ‘a statistically average patient’, and that applying a guideline to actual patients requires case by case judgement and not a cookbook response. The concern is that guidelines are dumbing down or oversimplifying psychiatry into protocols. An alternative way of looking at this is that rather than oversimplifying psychiatry, psychiatry using guidelines is becoming more patient-centred. The notion that doctors ‘teach’ consumers to participate in their health management is central to medical ethics 24 and guidelines apart from anything else, attempt to make treatment user friendly by adopting manuals and guided treatment approaches. Manualised approaches including through the self-help movements, have been acceptable to consumers for a long time and guidelines represent a new evidence-based generation of these approaches. It is almost self evident that guidelines may enhance the patient-doctor relationship by empowering consumers in clinical decision-making and by improving accountabilities between mental health practitioners and the community as to what constitutes mental health treatment more generally.
CONCLUSION
Guidelines should be resources that are available to use, and not introduced in ways that mandate use. Ideally, practitioners become familiar enough with them to have clear reasons for using them or not using them in particular clinical instances. A good clinician will commit to memory key recommendations and thereby integrate the guidelines with the needs of the patient to advance a good outcome. Guideline development, dissemination and implementation should be a matter for collective interest, discussion and planning in the mental health field so their potential utility to a wider range of stakeholders can be pursued. It is anticipated that the series will unite the sector in the provision of better and more confident professional practice.