
Abstract
Keywords
In recent times, spirituality has become an area that has been discussed at major professional meetings and conferences. This subject has, in the past, been alienated by the world of psychiatry. In medicine, the dividing line between religion and science has been clearly drawn. This artificial separation is in marked contrast to the earliest roots of medical practice. In many parts of the world a holistic view of the person has survived; this is seen in Chinese medicine, in the healing arts of the American Indians and, in our own culture, among Indigenous Australian peoples.
The last fifty years have witnessed a gradual rapprochement between science and faith. The western model of the dichotomised mind/body has been challenged on many fronts. Wig and Narendra 1 used illustrations from Hinduism to show the interrelationship of mental health and spirituality in India where the mind/body dichotomy concept is not followed. The impact of Eastern religious thought, emergence of New Age thinking and popularity of alternative health providers have all called for a more holistic understanding of health related issues. In an American study, 2 Austin et al. found that the central reason that many people are looking outside the biomedical model for their health care was the need for “whole person” therapy.
There is increasing awareness across professions of the importance that spirituality and religiosity has for many patients. Thus, there have been suggestions and research in relation to validating the incorporation of aspects of spirituality and religiosity into multidisciplinary assessments and interventions for patients with psychological and physical illness.
The domain of spiritual aspects of psychiatric patients has been overlooked in psychiatric assessments and management planning.[3] Cited reasons for neglect include the emphasis on psychiatry solely as a scientific discipline and the presence of a religiosity gap (or spiritual gap) between clinicians and their patients. In a study in New Zealand, a “practical gap” was identified between patients and their therapists. 3 This study found that while two thirds of the sample of patients reported beliefs in “God”, atheism and agnosticism were more frequently reported in the sample of psychiatrists, suggesting the presence of a religiosity gap, thus replicating similar findings in UK and USA. This study also found that only 11% of the sample of patients reported a spiritual history being taken in their psychiatric assessments, despite the fact that psychiatrists confirmed that these beliefs were important in the assessment. Lack of practical skills and poor teaching may be associated with this “practical gap”. The study also found that 94% of psychiatrists surveyed indicated they had not received formal or informal training in this area in their postgraduate training. 3
The alienation that has existed between the health professions and religion for most of the 20th century is ending and there is now more spiritual awareness. During the 1990s, many articles on religious and spiritual issues in health and psychotherapy were published in mainstream journals. 4 This area has been a focus at many conventions of health organisations. Topics have included attitudes and skills of spiritually sensitive and competent therapists and there has been a call for greater competency in religious and spiritual diversity in managing patients's illness and recovery.
In patients with a history of psychological trauma, there are suggestions that addressing spiritual and religious issues has an important place. Grame et al. 5 identify four theories that highlight the body-soul connection involved in psychological trauma, namely attachment theory, self-psychology, Thomas Aquinas theology of embodiment, and object relations' theory. There have also been suggestions for cross-professional training for psychotherapists and the clergy. 6
Unfortunately, this area–potentially crucial for the psychological and physical health and wellbeing of patients–has been under researched. It is important for those concerned with patients' psychological wellbeing and positive mental health outcomes, to be able to draw on every aspect of knowledge and appropriate interventions, and use supports and strengths that are available to the patient. This will ensure that all avenues are fully utilised to enhance recovery, global health and wellbeing of the patient, thus fulfilling the often heard need for whole person therapy or, more simply, “good medicine”. Accordingly, I aimed to carry out a pilot study surveying the spiritual attitudes and needs of rural and remote patients with a psychiatric illness.
METHOD
Patients attending the Department of Psychiatry of the Broken Hill Base Hospital, NSW, took part in the survey. Inpatients and outpatients were included. This survey instrument was a questionnaire developed and tested for reliability at the Centre for Excellence in Remote Psychological Medicine, Broken Hill, NSW. The questionnaire had 6 items. The test–retest reliability studies, using the questionnaire on a sample of ten patients and repeated after eight days, achieved a correlation of 0.83, suggesting good reliability. Case managers and the duty member of the Department of Psychiatry distributed the instrument to the patients. This questionnaire was a self report instrument.
RESULTS
The questionnaire was completed by 79 patients. The mean age of the sample was 44.6 years, with a maximum age of 71 years and a minimum age of 17 years. 28 males (mean age= 43.9 years) and 51 females (mean age= 45.0 years) completed the questionnaire. Included in the total number of participants were 14 (15.7%) Indigenous Australians. They consisted of 6 males (mean age= 42.8 years) and 8 females (mean age= 39.0 years).
After expectancies were adjusted to reflect general population, it was found that significantly more non-aboriginal than aboriginal people took part in the study and significantly more females than males participated.
The survey found that most patients (79%) rated spirituality as important, 13.4% considered it not important (or of little importance) and 7.6% were not sure (Fig. 1).
Patient ratings of importance of spirituality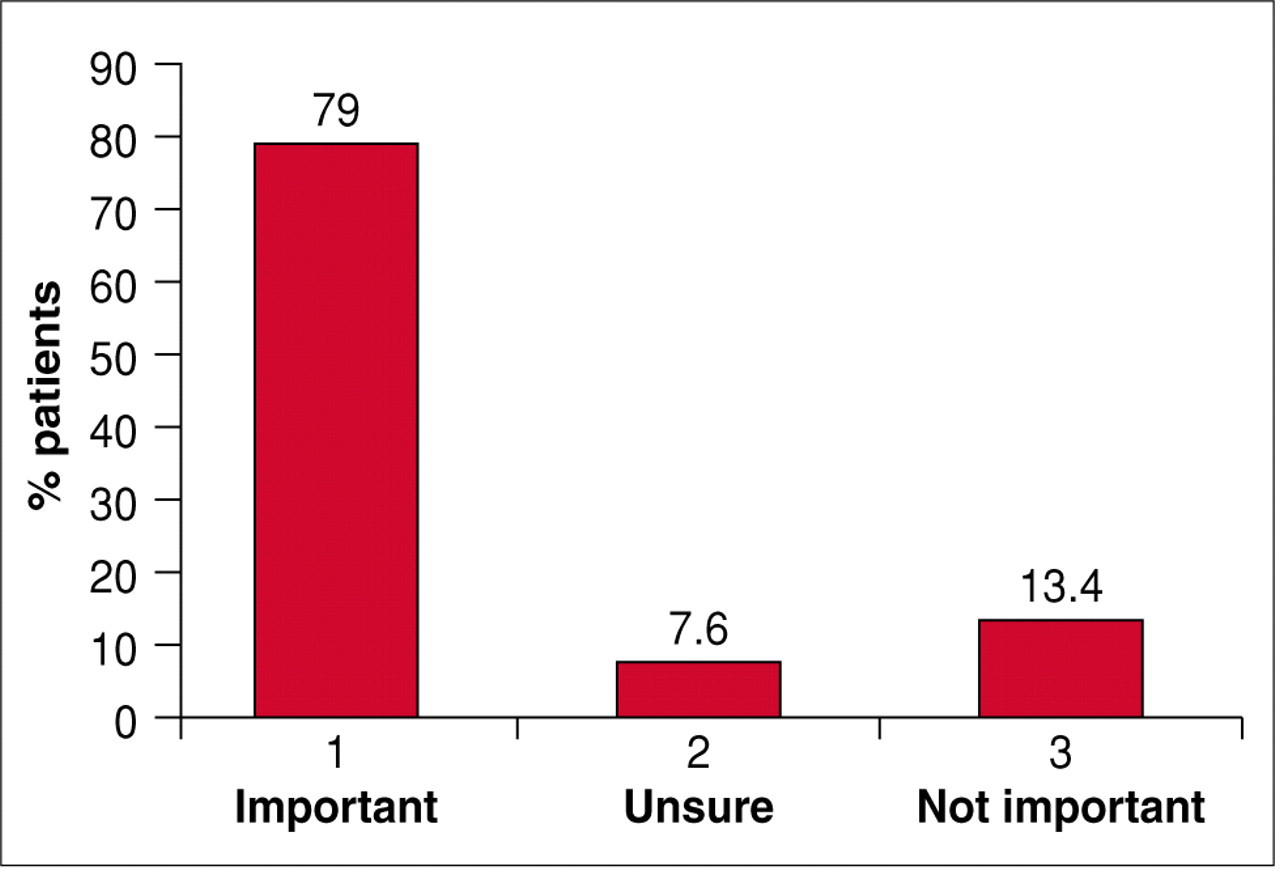
When asked if it was important that therapists should be aware of spiritual beliefs and needs, 82% of patients said “yes”, 13.7% said “no” (or “probably not”) and 4.3% were not sure (Fig. 2).
Patient ratings of importance of therapist awareness of spiritual beliefs and needs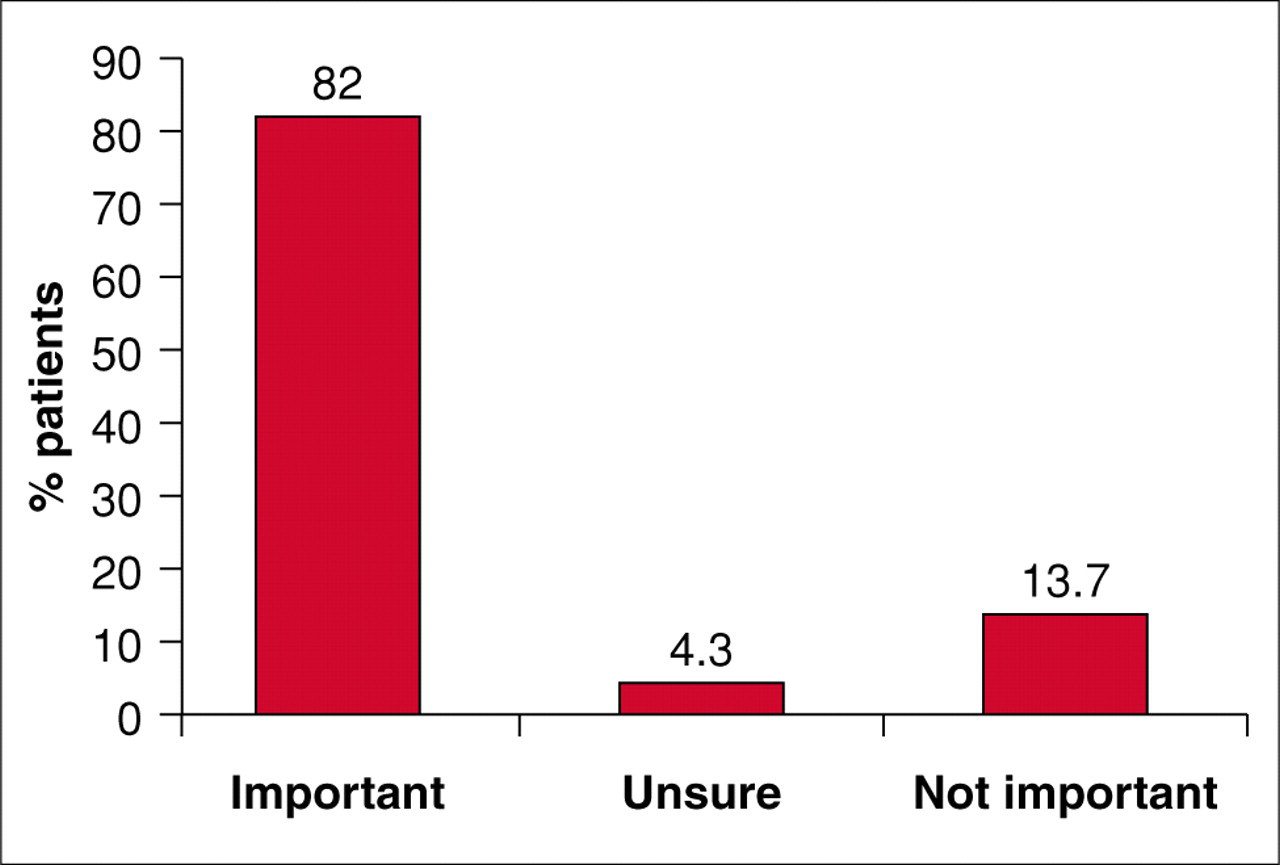
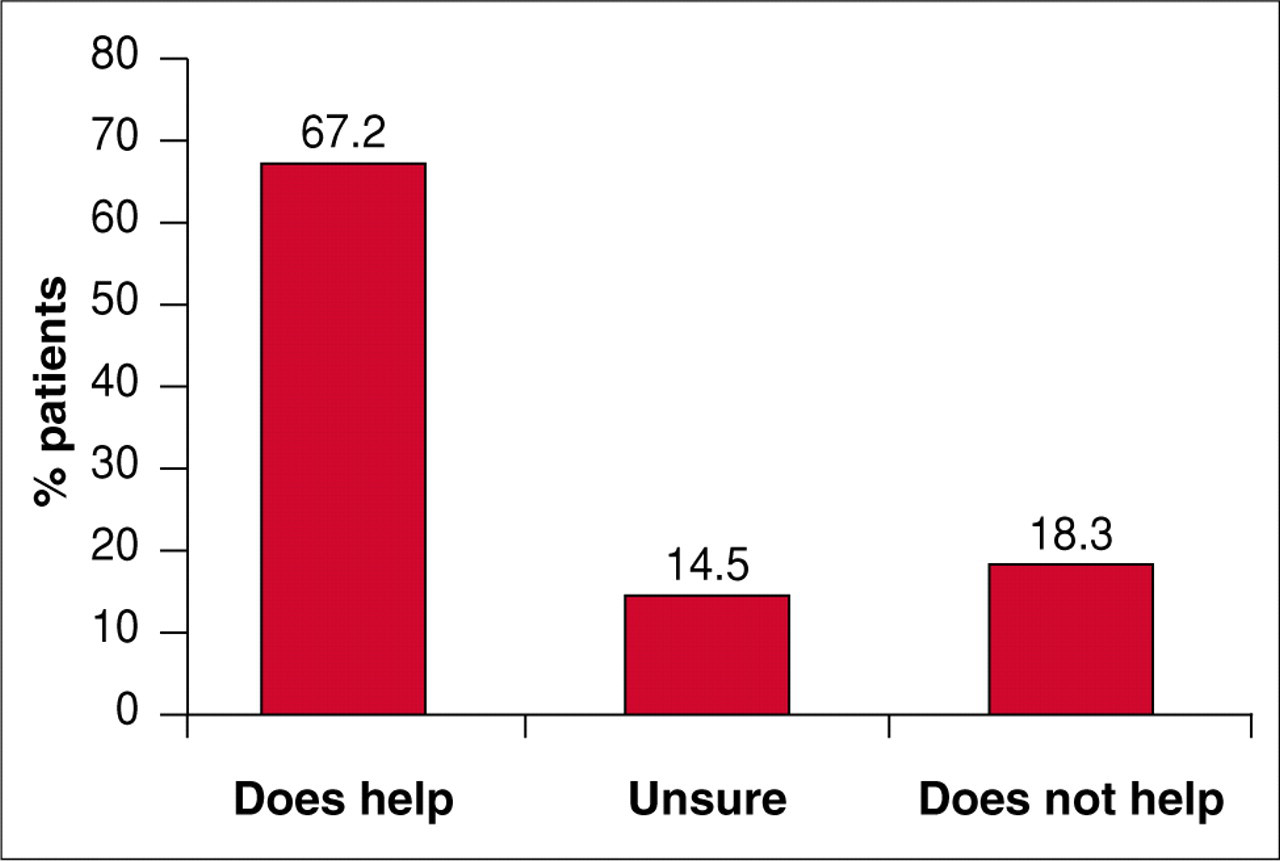
The majority (68.7%) of respondents believed that patients' spiritual needs should be considered by the therapist in treating psychological illness (Fig. 3); 19.7% did not believe these needs should be considered and 11.6% were not sure. About two-thirds (67.2%) of patients believed that spirituality helped them to cope with psychological pain (Fig. 4); 18.3% did not believe that spirituality helped in this way and 14.5% were not sure.
Should therapists consider patients' spiritual needs in treatment? Does spirituality help cope with psychological pain?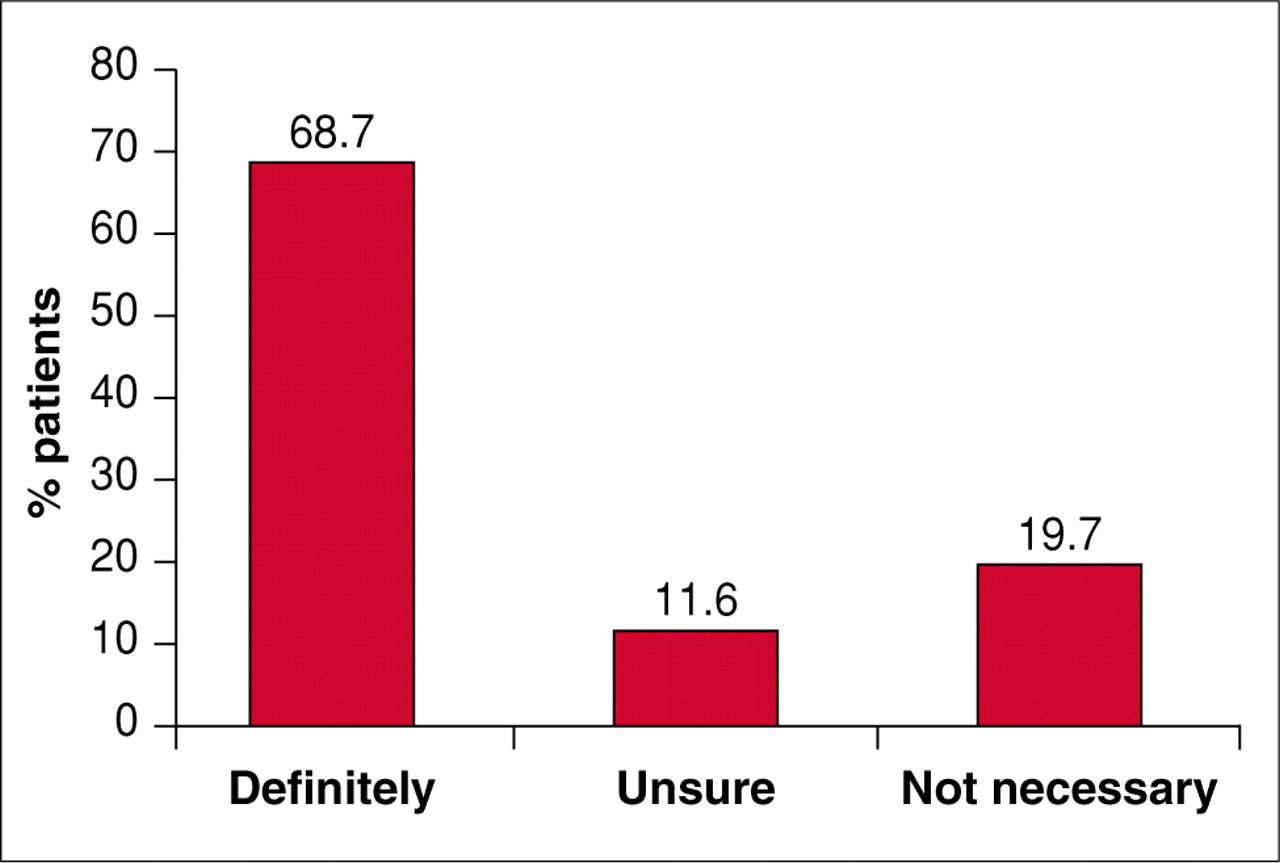
DISCUSSION
Spiritual issues encompass what is most meaningful and central in human existence. In times of crisis, illness and transition, spiritual issues are likely to come to the fore of human awareness for both patients and professionals. All health care professionals in different disciplines have distinct contributions to make in the way they use their training to assess religious and spiritual issues and needs of patients. All health care professionals need to include the spiritual dimension in assessment and treatment of patients. There is thus a need for interprofessional dialogue and collaboration in order to understand each other's perspective on the spiritual dimensions of care. 7
Therapists might utilise patients' beliefs to complement and facilitate the process of psychotherapy. Where appropriate, patient's spiritual resources can be used to enhance mental, emotional and physical healing. While, admittedly, this can be difficult ground for the psychiatrist, and physicians, addressing spiritual issues with patients is becoming an increasingly accepted part of whole person care in medicine. Although clinicians will differ in the extent to which they decide to utilise and delve into religious issues with their patients, there is a minimal standard that has emerged in this area. 8
The results suggest that, in this cohort, spirituality was an important issue with the majority of patients. There was strong mention of the requirement of these patients' therapists to be aware of their spiritual beliefs and needs. A requirement was also expressed by patients for their spiritual needs to be taken into consideration when treatment was being planned. In other words, in a majority of these patients a spiritual intervention would not only be accepted but also desired. 9 The outcome of this type of intervention on facilitating recovery and coping with psychological and physical problems is likely to be positive. Further research in the type of intervention and the outcomes of not only incorporating aspects of spirituality into the assessment but also offering, supporting and validating the spiritual beliefs of the patient will be an important, and interesting, exercise. The current evidence certainly suggests that the place of patient's spirituality needs to be considered in the assessment and management of persons with physical and psychological illness. To this end, the incorporation of spiritual history taking and spirituality into training of the medical practitioner and allied health professionals will be a step in the right direction.
At our centre, a multidisciplinary team, which includes pastoral care workers, indigenous health worker and consumers, has developed a model of taking a spiritual history that takes into account sensitivities and adopts necessary precautions. Doctors and counsellors are in positions of power and hence need to be careful not to invade people's spiritual space and exploit their vulnerability.
A “Spiritually Augmented Cognitive Behaviour Therapy” has been developed at the centre by the multidisciplinary team's members. This is a non denominational, structured ten week cognitive therapy with a focus on hope, acceptance, forgiveness and love. The behavioural interventions of relaxation, meditation, prayer and validation of the patient's spiritual belief system are incorporated into the cognitive component. The preliminary findings of a pilot study on the use of this intervention by trained professionals in a cohort of depressed patients who rated spirituality as important found the intervention to be very beneficial. 10 This has led to a randomised control study. The study compares a spiritually focussed intervention with conventional supportive case management for those patients with depression and hopelessness who rate spirituality as important.
In conclusion, the integration of spirituality into treatment may enhance recovery. Spiritually based interventions and collaborations that can optimise treatment should be used so that we can achieve the goals of social and emotional well being and maintenance of good health for our patients.