
Abstract
INTRODUCTION
Academic departments of psychiatry have played a vital role in the development of psychiatry as a major medical specialty in Australia. They have achieved this not only because of their undergraduate and postgraduate educational activities, but also through the willingness of senior academics to play leadership roles in the College, in State and Commonwealth departments of health, psychiatric service systems and in community organisations. Changes in both the university and the health system are putting pressure on academic departments to rethink their core responsibilities and redefine their mission.[1]
A REMINISCENCE
My own experience has occurred in four academic departments in Australia: the University of Sydney where I undertook my psychiatric training (1972-75), the University of Newcastle where I held the position of Senior Lecturer (1978-83), Monash University where I held a Chair of Psychiatry (1984-90), and the University of Melbourne where I have been Head of the Department since 1991. The differences between departments of psychiatry then and now become apparent when I recall the department at the University of Sydney in the early 1970s.
This department, led by Professor David Maddison, was limited to its site at the Royal Prince Alfred Hospital in Camperdown. There were three University funded academic staff, and satellites of the department had not yet been successfully established at any other hospital. The psychiatry ward was located on the ground floor of the neurosurgery building in a far corner of the hospital. It provided care for a cohort of anorexics, a mixed group of neurotic and personality disordered patients, and rarely an acutely psychotic patient sent in from the rooms of one of the three consultants or transferred via the consultation-liaison service. The ward had no catchment area and did not take certified patients. The patient population was determined by historical referral patterns, the interest of the consultants (one of whom was the Professor) and the needs of the general hospital in relation to treatment of patients who presented to the emergency department or were seen in the general wards. The ward was complemented by an active outpatient clinic with a large caseload of generally chronic patients with a full range of diagnoses and an embryonic consultation-liaison service to the general hospital.
Undergraduate students rotated through the psychiatric ward and had occasional ‘clinical’ demonstrations at the local psychiatric hospitals (Broughton Hall and Rozelle). Postgraduate training for the registrars fortunate enough to be selected was comprehensive. Supervision was intensive being both general and psychotherapeutic in orientation. All trainees were released two days a week to attend the postgraduate course, conducted by the NSW Institute of Psychiatry run at Broughton Hall and intended to prepare the candidate for the college membership which could be gained in three years. All trainees were obliged to spend six months at a psychiatric hospital to fulfil the college requirements for the ‘chronic case’.
The structure of the service was strictly hierarchical, with consultant psychiatrists clearly in charge. Some ward rounds were restricted to the doctors only (i.e. consultants, staff specialists, registrars and medical officers). Research was a low priority and appeared to be an optional extra for those academics who could afford the time. Few academics attempted a higher degree while sub-specialties other than child psychiatry were non-existent.
THE SITUATION TODAY
Such were the graceful conditions that existed in departments of psychiatry in the early 1970s. It is clear how much has changed! Academic departments are now much larger and multi-sited with most of the funding for this expansion having been derived from the psychiatric health services. The majority of units are now gazetted to cater for the mental health needs of a defined catchment. Only a few have managed to retain sub-specialty units and where these exist they are constantly under threat, a situation similar to that in the United Kingdom.[2] General hospital wards with a variety of ‘interesting cases’ are gone. Students see mostly chronic (or acute on chronic) psychotic patients in inpatient units and in community mental health clinics, which have all but replaced traditional outpatients. The patients who used to be seen in such units have ‘disappeared’ now being seen in private practice either in primary care or by psychiatrists.
Those with private insurance can afford private hospitalisation. The multi-disciplinary team utilising case management dominates the public sector and psychiatric training occurs predominantly in the community with the chronically psychotic and the multiply disabled or in acute wards with average lengths of stay of 7-10 days.
The laudable aims of the National Mental Health Policy and Plan, which provided high quality care for the ‘severe/seriously mentally ill’ in the community and an integrated based system of care, has unexpectedly produced a teaching and research environment restricted to one aspect of the rich field of psychiatry, namely psychosis.
THE CONTEXT
Why have these changes come about? Essentially, the answer is that both the health care system and the university system have changed dramatically as the result of the monumental forces that march under the twin banners of Equity and Access in health care and in tertiary education respectively. In many ways this can be seen as the natural consequence of the democratic process. As populations increase, inequities in health care cannot be ignored; solutions have to be found to meet the health needs of all. Governments are finding it necessary to stretch the health care dollar and distribute it more equitably across geographic and demographic lines as never before, in order to provide access to all segments of the population. The emphasis has shifted to dispersed health services that are focussed on the needs of the populations they serve, rather than the large centres of excellence devoted to specialist interests and are located in inner cities.[3] A similar thrust has occurred in education: 12 universities expanded virtually overnight to the current 38 (supplemented later by 2 private institutions) in order to provide tertiary education to an increasing proportion of the population who now must be educated if the country is not to be left behind in a world preoccupied with the ‘knowledge revolution’. While there has been an overall increase in funding, resources have had to be moved from the old to the new in health and education.[4]
The pace of these changes is immense. They are a result of exploding demand running headlong into the government's limited resources for the health and education services funded by tax dollars, which the community is increasingly unwilling to part with in a political climate dominated by the ethos of ‘smaller government’. A growing proportion of the public insists on a less hierarchical and a more participatory system in both education and health that responds to regional and community needs.
Both Commonwealth and State governments have moved directly to control the growth of public health care and tertiary education expenditure through new mechanisms such as case mix funding on the one hand and the introduction of Higher Education Contribution Scheme (HECS) on the other. Concurrently, the power of regional groups to influence government can be seen in the decision to establish the 11th and 12th medical schools at James Cook University and the ANU in 2000, at the same time as medical student numbers are being cut at other universities.
These changes have all impinged on patient care, teaching and research and are strikingly similar in a number of Western tertiary educational settings. Out of necessity, academic leaders have been forced to rethink the role of universities, medical schools and clinical academic departments of which psychiatry is one.
CLINICAL ACADEMIC DEPARTMENTS
Clinical academic departments have come relatively late to the medical school scene in Australia. The original split between the London teaching hospitals (in which clinical teaching was delivered) and the universities where basic sciences were taught, was transferred to medical training in Australia when basic science disciplines were firmly established in the original university medical schools at their inception. Clinical teaching occurred in clinical schools long before university departments of medicine and surgery were eventually established in these clinical settings. Departments of paediatrics, obstetrics and gynaecology followed while psychiatry came to most of these medical schools in the 1960s.[4]
Psychiatry in Australia faced particular challenges as an academic discipline because of its perceived link with a clinical-care system that was, while necessary, considered primitive, isolated and highly stigmatised. The staff of all these university clinical departments had to take on leadership roles in the clinical arena in addition to their traditional tasks of providing undergraduate teaching and establishing research studies to expand the boundaries of knowledge. The challenge for a clinical discipline is that it cannot be dissociated from its clinical base. It must provide care for its patients to establish its legitimacy and provide a clinical laboratory for its studies in order to be seen to be practicing what it preaches.
In Australia, the clinical involvement of academic departments of psychiatry occurred with psychiatric wards in general hospitals. There were good reasons for this focus at the time. General hospitals were the settings in which the other major academic clinical disciplines of medicine and surgery had established themselves. It is interesting to note, however, that obstetrics, gynaecology and paediatrics did not follow this tradition but in general were established in separate institutional settings (Women's or Children's Hospitals). It was psychiatry, however, that suffered a ‘cultural cringe’ about its institutional setting, namely the asylums that had spawned the discipline. It is useful to reflect on Gittelman's quote: “no institution has been so stigmatised and devalued as has been the asylum, far outweighing the prison and poorhouse”. Academic psychiatrists were trying to escape from the asylum, which had provided the setting for the origin of the profession at a time when governments were still preoccupied with the asylum as the solution to the problem of mental illness. Hence a wish of the nascent discipline of Academic Psychiatry to escape from the shadow of the spectre of the asylum and to be seen as an equal partner with its sister clinical disciplines Medicine and Surgery.
This was the situation in Australian universities until the Victorian government, in 1982, created and funded in conjunction with Monash University the first full University Chair located in an ‘asylum’. This was based at Royal Park Hospital in Melbourne, to which I was appointed in 1983. Numerous other such positions have been established across the country following this model.
CHANGES TO THE HIGHER EDUCATION SYSTEM
The Australian higher education system has been transformed over the past decade following the Dawkins reforms at the end of the 1980's. These reforms dismantled the binary system of universities and colleges of advanced education and encouraged higher education institutions to amalgamate, and saw the introduction of student fees. Change has been a continual feature since then.
The election of a Liberal National Coalition government in 1996, saw Australia, like the United Kingdom, Canada, New Zealand and the United States of America, begin to experience the withdrawal of government funding for higher education for the first time since the Commonwealth entered the field during the Second World War. HECS charges were raised, universities were encouraged to over-enrol and to accept fee paying Australian students. Meanwhile the universities were encouraged to adopt the efficiencies of the private sector and find cheaper ways of conducting their operations. There has also been a huge increase in overseas fee-paying students, numbers rising from approximately 10,000 in 1986 to more than 70,000 in 2000. This now amounts to almost 10% of total enrolments and provides value to the education system of approximately $2 billion. The Commonwealth government also made it clear that it regarded teaching as just as important an activity for universities as research. Therefore, university staff started to be assessed on the quality of their teaching. In addition, performance indicators
were implemented and university staff members came under continual pressure to produce in terms of acquiring grants, recruiting research students to their projects and publishing their work.[5]
These changes have had a major impact on faculties of medicine and thus on departments of psychiatry within universities. The increased focus on quality of teaching has meant further attention and time being given to both conducting teaching and evaluating and modifying it, based on the feedback. Similarly, the increased focus on research has meant that academics in psychiatry are under considerable pressure to demonstrate their productivity through the ability to acquire grants and produce papers. A concomitant focus on entrepreneurial activities to compensate for lost funding has meant that many academics have been forced to undertake activities that might not be seen as the core business of an academic department. In addition, as they in turn have felt the cold winds of economic rationalism waft through, clinical academics have been under particular pressure to contribute to over-stretched clinical services, to provide clinical leadership and support to other staff, and to contribute to the training of postgraduate psychiatrists as well as professionals from other disciplines.[6]
ACADEMIC MEDICINE TODAY
Mitchell T Rakin in a special article in Academic Medicine[7] has detailed some of the changes in practice as they have impacted on clinical academic departments in universities in the United States. He suggests that there has been a paradigm shift and he lists 25 changes that have occurred in the past two decades, which academics have had to come to terms with. I have summarised the 16 that are particularly relevant to the Australian situation in Table 1.
Peter Druker, a writer in business and management, made the following observation: ‘every few hundred years in Western history, we cross the divide. Within a few short decades society rearranges itself, its world view, its base values, its social and political structure, its art, its care institutions’. We are currently living through such a transformation. This is undoubtedly true in medicine, in academic medicine and academic psychiatry.
Comparison of paradigms that impact upon academic psychiatry, two decades ago and today
One option put forward to deal with this changing environment has been for medical schools to attempt to stand aloof from the health care system changes. Medical schools that wish to teach clinical skills to young health professionals have to place their faculty and students in clinical settings to do so. Those schools that wish to conduct research at the interface between laboratory and patient care need clinical settings. At the very least, therefore, clinical academic departments have to make the changes that are required to sustain partnerships with clinical facilities. This involves minimising the impost of teaching and research that clinical partners bear as they themselves struggle with shrinking health care budgets. Medical schools are having to formalise their relationships with their clinical partners, their products, as well as incorporating their perspective as part of their core business. A good example of the recent trend to formalisation is the agreement to the first memorandum of understanding between the University of Melbourne and its oldest teaching hospital, the Royal Melbourne Hospital, in a century.
THE SOCIAL CONTRACT BETWEEN THE UNIVERSITY CLINICAL DEPARTMENTS AND THE PUBLIC
Medical schools have an implicit social contract with the public although parameters and terms of the social contract vary, as medical schools vary.[8] In the tradition of social contract theorists society gives organisations privileges and resources. Medical schools derive their privileges from the preferences of society, developed from long cultural traditions concerning the need to train healers because of the essential contribution of healers to personal and social well being. By accepting these benefits, medical schools enter into to an implicit contact with the general public, forming the basis for asserting that the schools should work for the public good.
From the utilitarian perspective, society invests in institutions and individuals because it values the return of investment. In a free market society, the special economic and other privileges schools of medicine enjoy, whether these are expressed in funding from the Department of Education or the Department of Health's willingness to load the funding of teaching hospitals for this special role, or fund academic positions or indeed from the patient's eagerness to undergo care at teaching hospitals despite accepting the discomforts of being a teaching subject.
From the utilitarian perspective, to sustain and maintain this implied contract, medical school leaders need to understand the valued quality of what academic medicine provides and preserve this quality under changing circumstances.
From the perspective of any of these contexts for the notion of ‘social contract’ it follows that medical schools must ultimately be dedicated to improving the ‘public health’ through the dissemination of knowledge. Medical school programs in education, research, patient care, and community outreach are, or should become, a means to meet this overreaching mission to improve the nation's health.
As revenues from research and entrepreneurial activities become proportionally larger parts of schools' budgets, this implicit social contract extends to the organisations who control the external sources of revenue used to finance activities of medical schools and the leaders of those schools themselves.
All parties to the social contract with medical schools may be said to be ‘stakeholders’, meaning that they have stakes in the activities and resources of the institutions under either present or foreseeable future circumstances. In the case of academic medicine, the public (in the broad definition) is a stakeholder acting through the various agencies that have made the investments in medical schools using tax dollars.
THE ACADEMIC DEPARTMENT'S STAKEHOLDERS
The medical school has a social contract with students who deserve a high-quality education that will be the groundwork for a career in medicine. The education must be as relevant and as future oriented as possible. In exchange, from the student the medical school expects assistance with educational costs through tuition, an absolute dedication to the educational process and medical profession, and the maintenance of the highest ethical standards.
The staff looks to the faculty medical school for professional development, economic security, and the opportunity to work with other scientists, clinicians, and research reamers in an effective and collegial environment. In return, they support the institution's missions, demonstrate professional integrity, and are committed to modelling appropriate qualities for all students and colleagues. Above all, they must set high standards to achieve excellence in teaching.
From affiliated hospitals and clinics, medical schools should expect high standards of patient care and opportunities for education and research where students, residents and faculty can develop and flourish.
Governments at all levels are core stakeholders. From governments medical schools should expect support, financial and otherwise, and a shared vision of purpose and value of the nation's medical schools. From its investment in research, the federal government can expect advances in knowledge and technology and the scientific and clinical innovations that accompany such advances. Scientific integrity must be safeguarded and violators seriously disciplined. Schools that enjoy substantial state support bear the added responsibility to provide a well-educated medical work force.
Patients treated in academic medical centres have every right to expect treatment of the highest scientific, technical and humane quality by physicians and others who are knowledgeable, responsive, and respectful. These patients, knowing their care is rendered in a teaching environment, have an obligation to follow their treatment programs, participate in the educational process, and also, as appropriate and with informed consent, participate in research.
Postgraduate medical education has been the responsibility of medical schools in some instances, and of hospitals in others and more recently of the medical college. Increasingly, graduate medical education programs are affiliated with medical schools. Recognising that medical education begins with medical students but extends through the residency and beyond, medical schools have established high standards of postgraduate medical education programs.
Other health care professionals look to medical schools for scientific advances and for well-educated physicians prepared for effective interdisciplinary, collaborative practice. In return, medical students and faculties anticipate the professional respects and collegiality of other health care professionals and also expect those whom they work with to be well educated.
Last but not least, increasingly important core stake-holders in some, but not all, medical schools are those who have provided funds or entered into partnerships and achieve goals. Examples of such stake-holders include the State Health Department, Department of Veterans Affairs, research funding agencies, professional and voluntary health organisations, and more recently the private sector particularly pharmaceutical companies and private hospital groups who believe such links offer them a strategic advantage in a competitive commercial environment.9–11
A SOLUTION FOR THE TIME - THE PHENOMENON OF REINVENTION
In the changing era clinical academic departments are being pressured into taking on roles and responsibilities for which their staff may not be qualified nor even endorse. In each era, however, whether it is every few years, decades, or lifetimes, all institutions have to constantly review their roles and re-examine their perspective. Implicit in this process is the recommitment to a social contract in whatever form is most appropriate for the time. Precisely because the social contract is implied rather than explicit, its dimensions have to be assessed as comprehensively as possible by the academic leaders of the time and the role and mission of the department restated for the time and if necessary reinvented itself.
This process of reinvention does not mean overturning traditional values of excellence in teaching and research, but it does mean redefining the agenda so that the public and those who fund practice institutions can understand and support it. What does this mean in practical terms? In general, it means embracing increased partnerships with outside organisations to provide funding for mutually beneficial initiatives. The most common and acceptable of these joint ventures has been with public psychiatric services which retain high quality staff and provide a focus for quality improvement of services. More problematic but equally important are the links with the private sector - private psychiatric hospitals and pharmaceutical companies who have a particular interest in advancing the understanding and treatment of those with mental illness.[11], [12] However, both have an aura of opprobrium, which surrounds them because they are engaged in for profit activities.
Today as a result these links are essential. In the following two examples I will highlight two elements of activities of my current department with private and public sector which have involved reinvention.
HEALTHSCOPE, THE MELBOURNE CLINIC AND THE UNIVERSITY OF MELBOURNE - THIRTY YEARS OF REINVENTION
Members of the University of Melbourne Department of Psychiatry played key roles in the establishment of the first major private psychiatric clinic in Melbourne in the early 1970s. At that time such involvement was considered outside the realm of legitimate academic activities of the University to the extent that private practice conducted by the University academics in this setting was frowned upon and attempts were made to ban it. In the early 1990s, however, when Healthscope, the company that then owned the Melbourne Clinic, approached the Department of Psychiatry to create an academic unit there, the University was much more accommodating. An academic unit was established under the leadership of an associate professor who was employed by the University under exactly the same conditions as applied to similar positions in the public sector but with funds provided by Healthscope. At the end of the five-year period the arrangement was so mutually beneficial that Healthscope agreed to fund a Chair of Psychiatry at the Melbourne Clinic and jointly fund an additional Chair of Psychiatry in Geelong where they owned the Geelong Clinic in partnership with the public psychiatry service (Barwon Health). Professors Isaac Schweitzer and Michael Berk respectively now fill these positions.
THE EARLY PSYCHOSIS PREVENTION AND RESEARCH PROGRAM - AN EXAMPLE OF REINVENTION OVER 20 YEARS
In Figure 1 an example is provided of the key changes that have occurred in a major clinical and research area of interest in the Department of Psychiatry at the University of Melbourne, namely, the Early Psychosis Program.
A chronology of changes in the Early Psychosis Program, Department of Psychiatry, University of Melbourne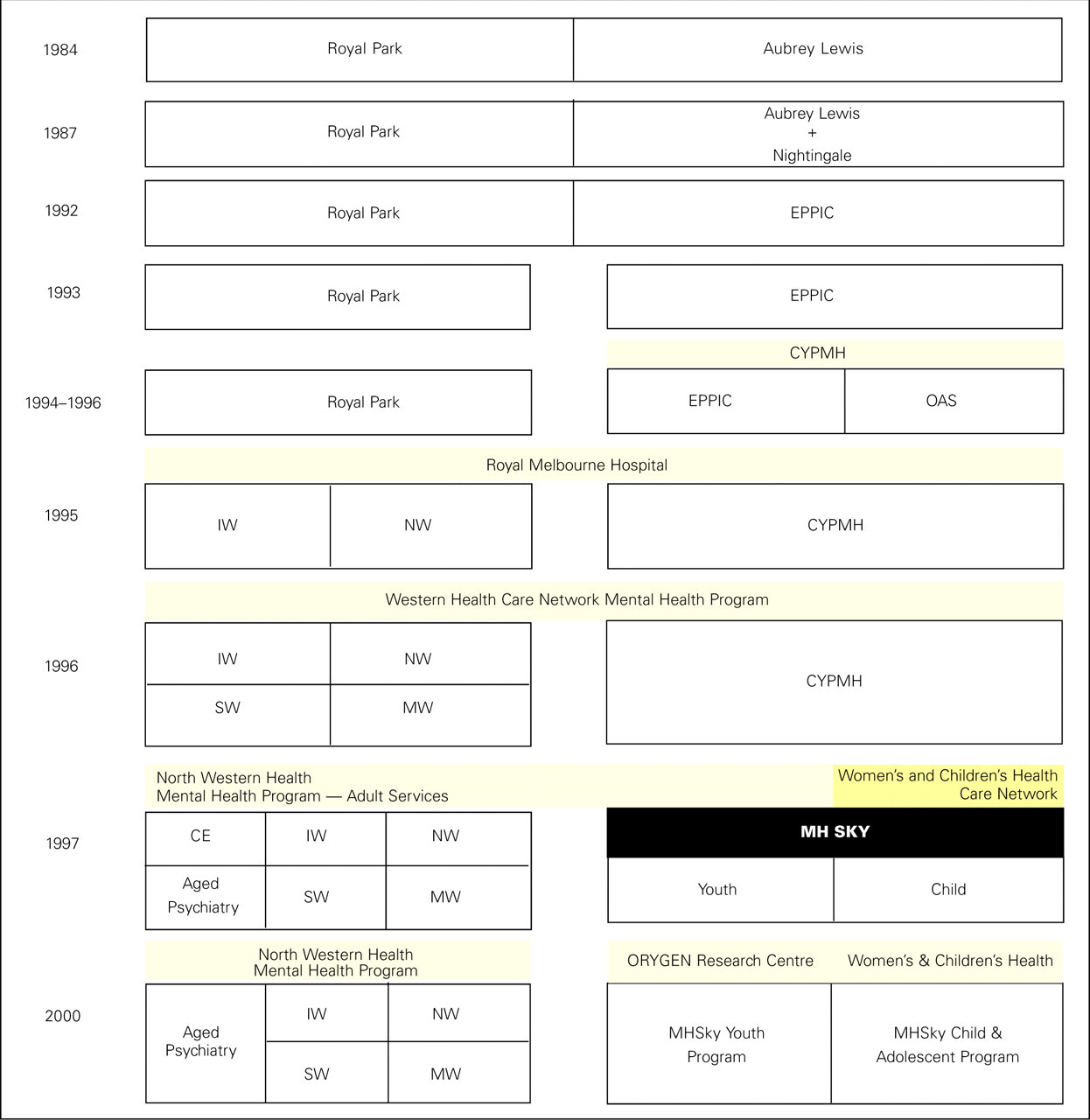
The beginning of the Early Psychosis Program Unit at Royal Park Hospital occurred in 1984 following the establishment of the Monash clinic in 1983, which led to the opening of a 10-bed establishment focusing on patients with schizophrenia who were appropriate for research studies. One component of this unit was dedicated to studying people with their first episode of psychosis. The history of the developments of this unit has been documented.[13], [14]
In 1987 it became possible to merge this unit with a 10-bed rehabilitation ward, which was seeking a new role. The Aubrey Lewis Unit was merged with Nightingale Ward to establish what was called a ‘recovery program’ for patients with early psychosis. In 1992 these hospital-based components were supplemented by community component services to form the Early Psychosis Prevention and Intervention Centre (EPPIC). In 1993 this program separated itself from the administration of Royal Park Hospital to become independent. As a result of negotiations the Centre for Young People's Mental Health incorporated the older Adolescent Service from the Royal Children's Hospital and became active in 1995 as part of the Royal Melbourne Hospital structure. In 1997, the Centre for Young People's Mental Health linked with the Child and Adolescent Service of the Royal Children's Hospital to form the Mental Health Service for Kids and Youth (MHSKY). In 2001 a large grant from the Colonial Foundation facilitated the development of all the research activities as the ORYGEN research centre in conjunction with the MHsky clinical program now to be known as the ORYGEN youth mental health service.
Each of these developments was both opportunistic and strategic in the sense that each was designed to capitalise on opportunities that existed at the time, as well as to demonstrate to funders of the service that the service was performing vitally important - if up to then neglected - tasks. The service provides an opportunity for the department to maintain access to a specialised area of psychiatry to recruit and obtain high quality staff, to provide a world-class facility for teaching undergraduates and trainees and to provide ground breaking research in the development of guidelines for appropriate management of early psychosis. Each of the changes occurred in the context of an environment that was constantly changing and required the support of administrators at all levels of the service from the hospital through to the Regional Office and Psychiatric Services Program of the Department of Health in Victoria. They illustrate the considerable flexibility that needs to be demonstrated if academic centres are to be able to continue to work in the areas in which their expertise can be valued.
CONCLUSION
The future of academic psychiatry in Australia is likely to continue changing over the next decade. Increasing financial pressures will continue to impinge on these departments. However, academic psychiatry can survive and indeed thrive within such an environment. Alan Gilbert, Vice Chancellor of The University of Melbourne, has reminded those who yearn for the ‘good old days’ that universities, although 1000 years old, have rarely been stagnant. They have constantly had to modify and adapt and have been one of society's most successful institutions in making these changes. They must be relevant to the needs of their communities while defending traditional values of scholarship and research.
Despite innovative partnerships coming under increasing scrutiny and some criticism for so called selling out of traditional academic values, they remain one of the few ways that university clinical departments such as Psychiatry can continue to deliver on their social contract with the community.