
Abstract
The political, professional and economic context in which mental health care is delivered in Australia has changed significantly over the last two decades. Traditionally, emphasis was placed on the central roles of mental health specialists and associated institutional and community-based forms of service care. In reality, a large proportion of mental health care was delivered by general practice and other primary care services. Now, the central role of these professionals, and changes in the ways in which they will deliver primary care services, are of utmost relevance.
Many psychiatrists and clinical psychologists, and some consumer and carer groups, consider the drive towards primary care-led mental health services (which is directed largely at persons with common mental disorders such as depression, anxiety or substance misuse) to be misplaced. Fears of low cost, low quality, pharmaceutically-dominated treatment systems, with limitations on access to specialist services, are common. Other critics have suggested that the expected increase in treatments will result in other unforeseen circumstances, such as increased instances of discrimination in employment or insurance.
This report describes the movement towards a broader and more collaborative system of mental health care for Australia and highlights its potential merits. A primary care-based system is the only system that has the potential to reach the broader population, provide access to the right mix of affordable primary and secondary care services, and promote the integration and continuity of medical and psychological care that persons with mental disorders require.
Currently, mental health services are fragmented and disjointed (primary vs secondary care, private vs public systems, Federal vs State-based initiatives, medical vs psychological care systems). Perhaps, more importantly, key aspects are so poorly distributed that major sections of the population, particularly outside capital city environments, have great difficulty accessing any specialist care. 1 , 3 Additionally, socioeconomic factors have a marked effect on access to both medical (due to very poor distribution of psychiatrists) and non-medical (due largely to the lack of government-based financing systems) specialised forms of care. A key theme of current community education and destigmatisation campaigns is to see mental health as ‘health’. The more such patients are managed well in general health settings, and the more general practitioners (GPs) promote mental health as a central aspect of their work, the more quickly community attitudes towards help-seeking for mental health problems will change. 4
The movement towards a system of primary mental health care has been influenced by a series of major events, studies and reports. These are listed chronologically in Table 1. The general themes of the key policies, reports, initiatives and government directives on mental health and general practice reforms listed here are: the need for the development of collaborative and integrated ways of delivering mental health care, and an increasing emphasis on the central role of primary mental health care.
Chronology of a decade of major events impacting on reforms to mental health care in Australia
In short, these major influences included:
the growing body of evidence pointing to the need for more effective mental health care for a broader range of consumers than those traditionally cared for by public sector mental health services (the point was made earlier that GPs had always been the key providers of this care);
the second National Mental Health Plan, 14 which emphasised the development of partnerships between primary and secondary providers. This included recognition that GPs needed to be better supported by their specialist colleagues; and,
the evolution of the Federal General Practice Strat-egy 20 over the past decade, which has argued that health outcomes for a range of common health problems could be improved through more appropriate primary care services.
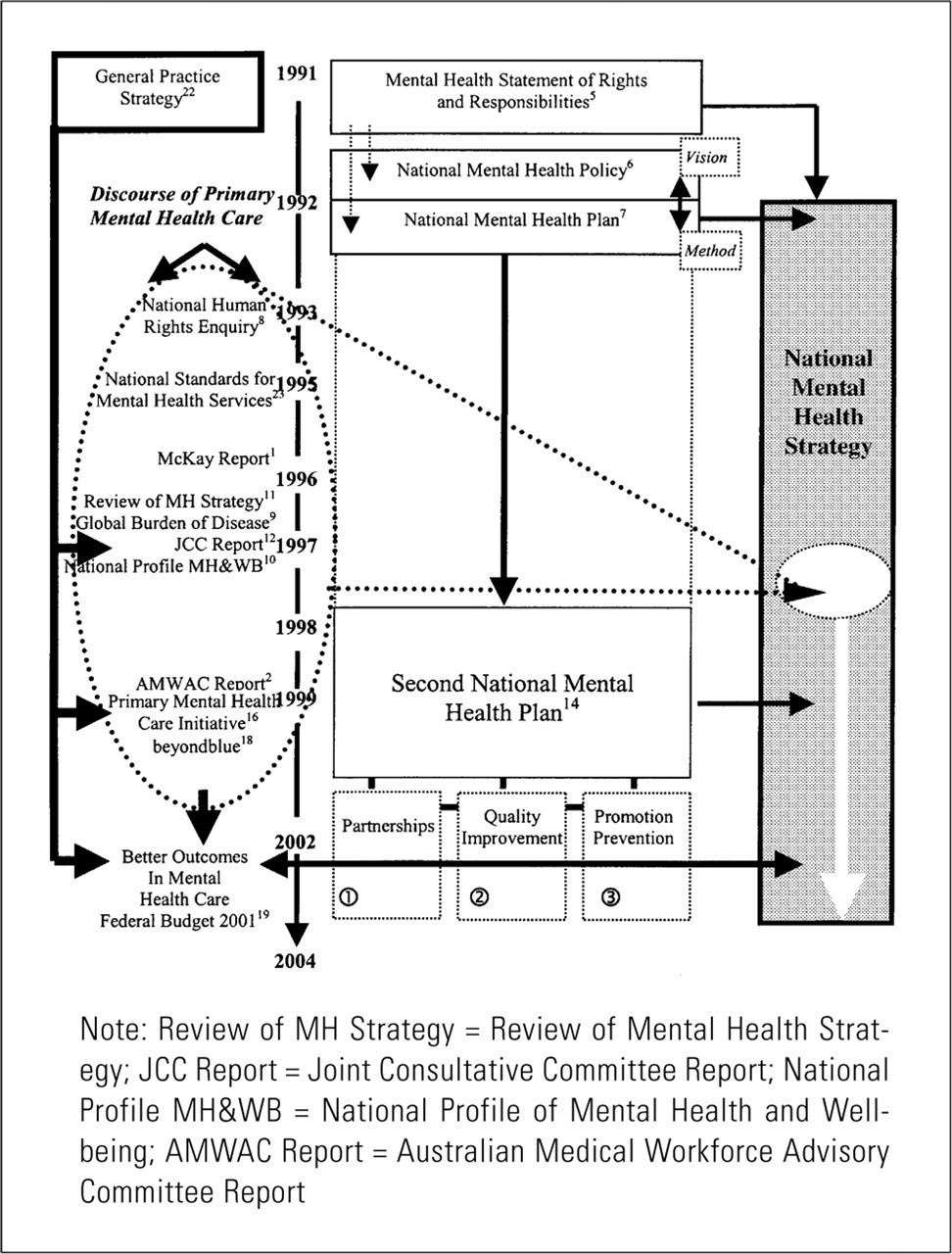
The process of reform, though incremental in nature, appears to have been constant in its movement away from institutional towards community-based primary mental health care. However, there is a risk here that this chronological analysis suggests a planned and proactive approach to mental health care reform by the Commonwealth Government. In reality, the process appears to have been much more organic, being influenced at critical points by a wide range of other national and international factors. Figure 1 illustrates this organic process as an emerging ‘discourse of primary mental health care’ - a body of knowledge developed over a 10-year period that has influenced the attitudes of clinicians and policy makers.
The emerging ‘discourse of primary mental health care’ and its relationship with the National Mental Health Strategy is portrayed in Figure 1. The thick black arrows in Figure 1 highlight a number of major influences on the Federal Government's decision to finally allocate $120.4 million over four years to primary mental health care in its 2001 Federal Bud-get. 19 Here it is shown that the ‘discourse of primary mental health care’ both influenced, and was influenced by, the evolving Mental Health and General Practice strategies.
An emerging ‘discourse of primary mental health care’ and its relationship with mental health care reform 21
As mentioned, in the 2001-2002 Federal Budget, the Commonwealth Government approved $120.4 million for the Better Outcomes in Mental Health Care initiative - a model designed to advance primary mental health care in Australia over a four-year period. 19 At the time, this was the largest single allocation of funding by the Australian Government for primary mental health care reform. It is worth noting that this allocation of funding was in addition to the $6 million previously allocated for the Primary Mental Health Care Initiative and the $17.5 million of Commonwealth funding (over five years) for ‘beyondblue: the national depression initiative’.
The main driving forces behind these significant new reforms were:
a partnership between a range of mental health advocacy groups (“beyondblue: the national depression initiative” - www.beyondblue.org.au; The Mental Health Council of Australia) and key professional groups (Australian Divisions of General Practice, ADGP; Royal Australian College of General Practice, RACGP; Royal Australian and New Zealand College of Psychiatrists, RANZCP; Australian Psychological Society, APS);
the Commonwealth Department of Health and Aged Care (DHAC; incorporating the concerns of both the Primary Mental Health Care Initiative within the context of the Second Plan of the National Mental Health Strategy, and relevant developments within the General Practice Strategy, focusing largely on maximising health outcomes in patients with common, chronic and relapsing disorders such as diabetes, asthma and depression); and,
a Federal Health Minister (Dr Michael Wool-dridge) who was committed to the implementation of reforms in both the mental health and primary care sectors. The total cost of the new reforms, the response of the Minister to the model proposed by the stakeholder partnership, and the process of collaboration between the stakeholders and the Commonwealth Department to design and implement the package, were all indicative of broad stakeholder support for this process.
Following the Budget announcement, the then Federal Minister for Health, Dr Michael Wooldridge, charged the General Practice Memorandum of Understanding (GP MoU) Group (the GP MoU Group comprised representation from the ADGP, RACGP, Rural Doctors Association of Australia (RDAA) and DHAC) with the responsibility for the development of the details around this Budget measure. A national committee, called the Committee for Incentives in Mental Health (CIMH), was formed by the GP MoU Group in June 2001 to provide it with advice and recommendations on the development and implementation of this initiative. The membership of CIMH is outlined in Table 2.
In recognition of the need to maintain ownership of the initiative by all major stakeholders, CIMH made the decision to establish three task groups to provide it with advice on the development of specific areas of the initiative. The three task groups established were:
the Education and Training Task Group (chaired by RACGP);
the Medicare Benefits Scheme (MBS)/Incentives Task Group (chaired by ADGP); and,
the Allied Health Task Group (chaired by APS). 24
Each of the task groups comprised membership from the organisations represented in CIMH. The individual members of the task groups were expected to seek the input of their respective organisations and/or constituents prior to agreeing to a particular position. Following their consultations and deliberations, the task groups were asked to provide CIMH with advice on the development and implementation of the specific areas (e.g. education and training). CIMH then took this advice and used it to formulate a set of recommendations for consideration by the GP MoU Group. Once all the details were agreed to by the GP MoU Group, they were then put to the Federal Minister for Health for consideration and formal ratification. This process is represented diagrammatically in Figure 2.
The double-headed arrows in Figure 2 represent the iterative nature of the policy process. To illustrate this point it is worth considering the relationship between the task groups and CIMH. In the first instance, following consideration of specific issues relevant to their area (e.g. education and training), each task group provided CIMH with advice which was then used to assist in the formulation of a set of recommendations to be put to the GP MoU Group. When CIMH was unable to reach consensus on a particular issue, it then requested further advice from its task groups. This iterative process occurred at every stage, including the information flow to, and from, the office of the Federal Minister for Health and Ageing.
On July 1 2002, the first stage (i.e. incentive payments to GPs for completing cycles of care) of the Better Outcomes in Mental Health Care initiative that was detailed in the 2001 Federal Budget (see Table 3) came into place (www.health.gov.au). In November 2002, GPs will be able to claim new MBS items for the provision of focused-psychological strategies. A series of pilot programs will commence in late 2002, administered through local Divisions of General Practice, to purchase non-pharmacological treatments from a range of non-medical mental health specialists. Access to consultations with psychiatrists in emergency situations, in which the psychiatrists are remunerated for their time, is planned. The mechanism for payment for these services is to be resolved. Each of the new GP payments is tied to a requirement to engage in significant and ongoing skills training in mental health (www.racgp.com.au). These services are only to be provided within accredited general practice environments and, hence, do not encourage the proliferation of specialised psychological services outside the family medicine setting. However, not all aspects of the original model proposed by the stakeholder group were supported. Notably, proposals to offer incentives for psychiatrists to provide more initial consultations and ongoing (rather than just emergency) telephone-based consultation services to GPs were not supported.
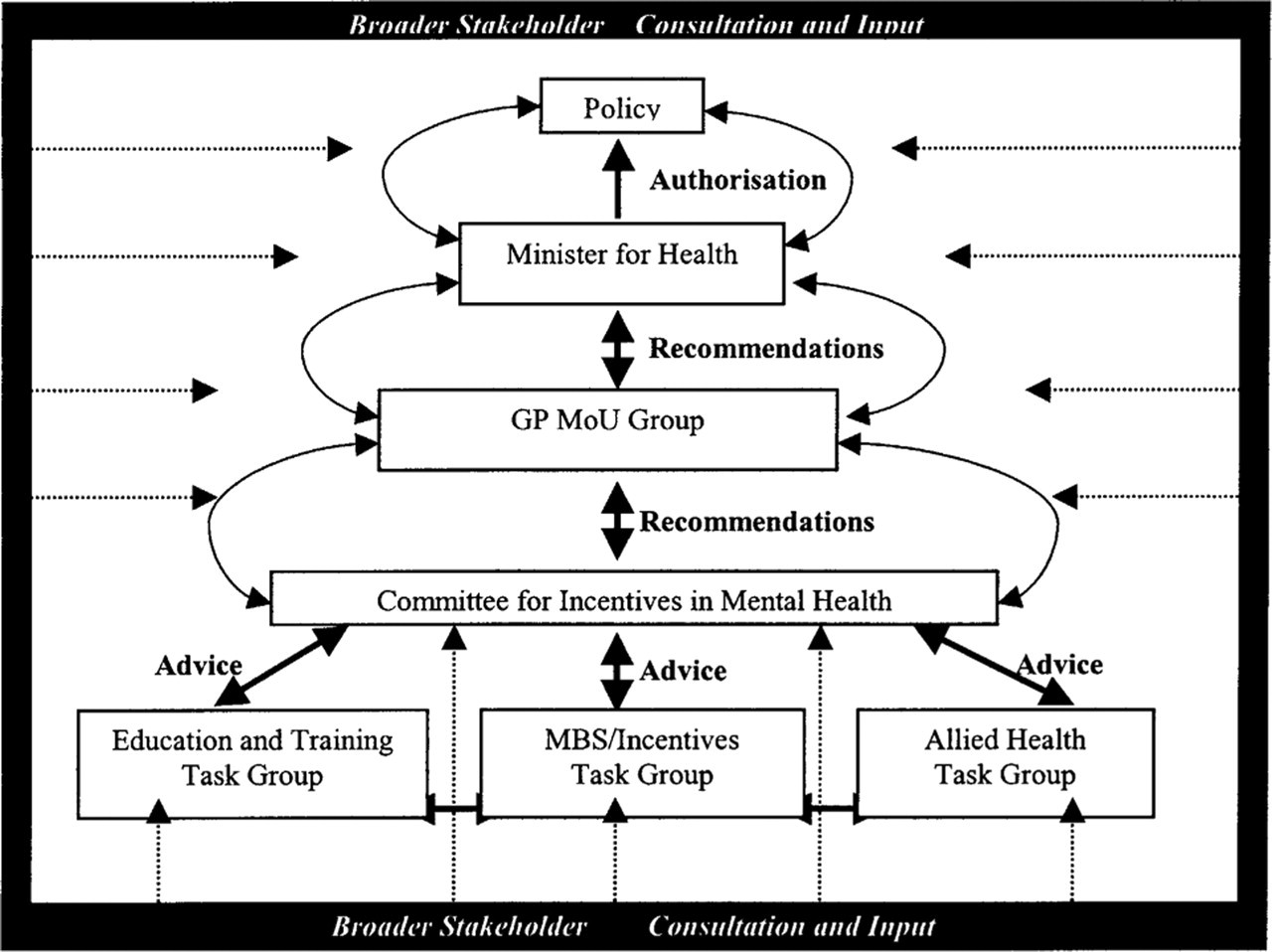
Committee for Incentives in Mental Health (CIMH) development of the Better Outcomes in Mental Health budget measure 21
Membership of the Committee for Incentives in Mental Health (CIMH) 19
Elements of the Better Outcomes in Mental Health Care initiative (2001-2005)
The specific focus on primary care-led mental health service reform has been in response to a range of factors. These include:
the population health focus of the Second National Mental Health Plan;
the body of evidence described in Figure 1;
consultation with consumers and carers whose lives are affected by common mental disorders such as depression and anxiety; 25 and,
current community views regrading the appropriate service environments and treatments for the management of common mental disorders. 4
The potential benefits of such a system are listed in Table 4.
Undoubtedly, there is a range of potential limitations with such a general practice-based system. If the system simply relies on a relatively ‘illiterate’ community 4 , 26 to present their psychological difficulties within a system that does not prioritise their active management or is not committed to the provision of an appropriate mix of evidence-based pharmacological and non-pharmacological treatments, then overall improvements in outcomes are unlikely. The deficiencies within the current general practice system have been extensively documented and we now have a number of relevant databases through which changes can be tracked. 30 , 32
As distinct from many of the deficiencies in the current specialist care systems, however, changes within critical areas of community understanding, professional attitudes, mix of services provided and distribution of services, are firmly on the primary care agenda of the relevant professional, community and advocacy groups. For example, the investment within the ADGP in infrastructure for mental health is now considerable. 33 While we are not yet close to achieving an ideal primary care-based mental health services system for persons with common mental disorders, it may assist to have a clear notion of the priorities of such a system (Table 5). At the heart of such notions are clearly models of proactive ‘stepped care’ that have been well developed in certain US health care systems. 34 , 35 Such systems prioritise early recognition of disorder, provision of the appropriate mix of primary care and specialist services at the appropriate point in the illness course, the appropriate mix of pharmacological and non-pharmacological interventions, active tracking, consumer support and outcome measurement. To date, these systems have only been tested within fixed care/fixed population environments. Similarly, primary care developments in the United Kingdom have begun to track more actively whether a variety of models may achieve sustainable improvements in population-based mental health services. The challenge for us is whether, within the Australian health care system, we can achieve both ready access and affordability of a relevant mix of services in combination with continuous improvements in the quality of services provided.
Potential benefits of a primary care-based system
Priorities for an ideal primary care-based system