
Abstract

A unique set of objective swallowing data is presented on a patient with a posterior pharyngeal wall cancer, starting before development of malignancy and swallowing abnormality and then tracing the progression of swallowing changes through serial evaluations performed before and after treatment of the cancer. Despite objective evidence of aspiration into the bronchi and lungs, the patient continued his regular diet, gained weight, and had no aspiration complications.
CASE REPORT
A 58-year-old man with a history of heavy alcohol and tobacco abuse originally sought treatment for a retropharyngeal neck abscess. The cause of the abscess was a 4 × 4 cm left-sided posterior pharyngeal wall squamous cell carcinoma that had metastasized to a retropharyngeal lymph node. After triple endoscopy he was noted to have bilateral cervical level II nodal involvement, and his tumor was staged T2N2bM0.
Coincidentally, 1.5 years before his cancer developed, this patient had enrolled in a research study on swallowing. Control subjects were being sought as cohorts to the population of cancer patients treated at the Detroit Medical Center, and persons with a history of smoking and drinking were included. When his cancer was later diagnosed, he presented an unusual opportunity for us to obtain a set of swallowing data, including his premorbid condition, for comparison.
The patient underwent a full course of photon radiation therapy to the primary site (70 Gy at 2 Gy/fraction) and bilateral necks (50 Gy to all nodal areas and 70 Gy to the involved nodes). He also received WR 2721 during radiation as a radio-protector for the salivary glands to reduce xerostomia. He underwent a tracheostomy to provide a stable airway before drainage of the abscess; this was removed 2 weeks after completion of radiation therapy. At completion of radiation therapy, there was no evidence of residual disease, and 15 months after treatment, when data collection was terminated, he was still free of disease.
Scintigraphy was used to quantify swallowing efficiency and aspiration. The test was performed with 2.5 mCi Tc 99m sulfur colloid added to 10 ml of either water or thickened apple juice with a viscosity of 1100 centipoise. 1 Dynamic imaging was used to determine oropharyngeal residues and bolus transit timing variables, from which a swallowing efficiency score was calculated. 2 This was followed by a series of 2-minute static scans to determine whether aspiration had occurred. The percentage of aspiration was quantified by outlining regions of aspirate in the subglottal region (proximal trachea), distal trachea, and bronchi/lungs and then by determining radioactive counts in those regions, referenced to the total radioactivity emanating from the patient. 3 Twenty-five minutes later the static scans were repeated to determine the amount of aspirate that had been removed by spontaneous coughing and natural clearing mechanisms.
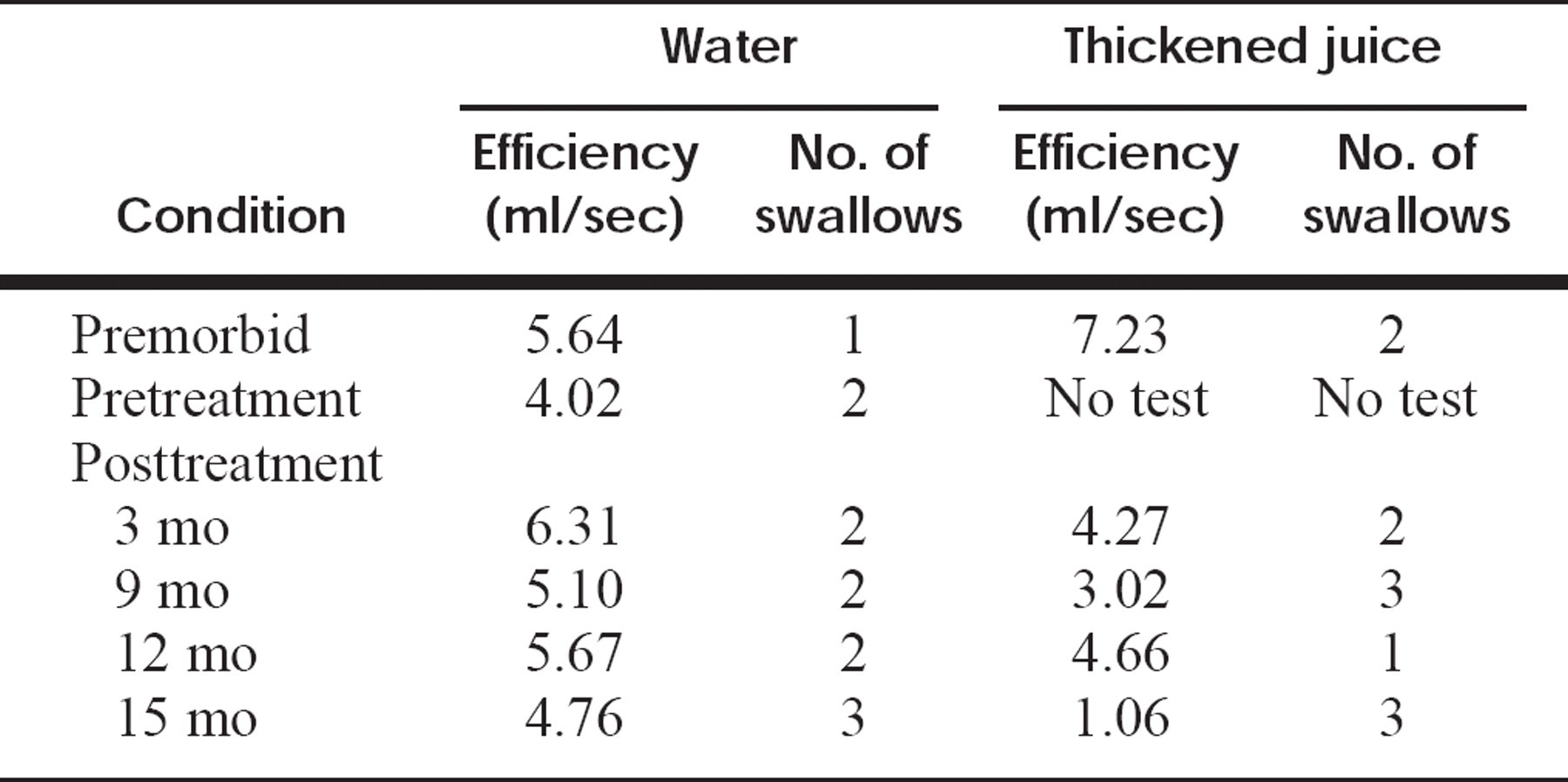
Changes in swallowing efficiency for the first swallow and number of swallows taken to ingest the test bolus, as determined by scintigraphy
Aspiration and rate of clearance
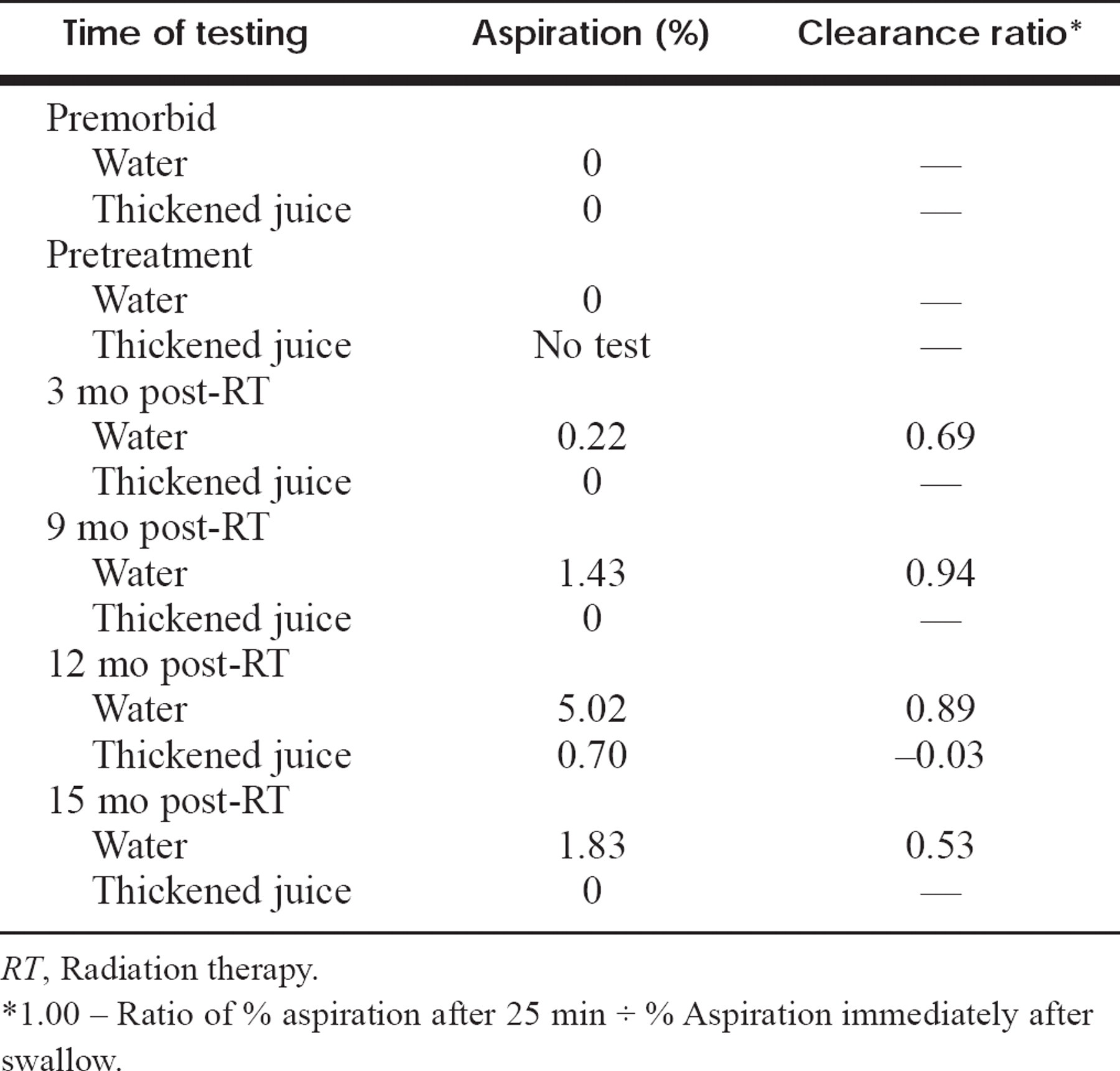
RT, Radiation therapy.
1.00 - Ratio of % aspiration after 25 min ÷ % Aspiration immediately after swallow.
Table 1 shows changes in swallowing efficiency over time. The patient demonstrated normal swallowing function before the development of cancer. 1 Swallowing efficiency of the water bolus improved to premorbid values 3 months after radiation therapy and then declined slightly thereafter. For the thickened apple juice swallowing efficiency did not revert to normal 3 months after radiation therapy and also declined thereafter. An increased number of swallows was required to ingest the test bolus after treatment, which is related to the decline in efficiency, which is based on timing and oropharyngeal residues after the first swallow. 2
No aspiration was detected for either water or thickened apple juice before disease onset or immediately before cancer treatment (Table 2). Three months after radiation therapy the patient was noted to aspirate into the subglottic region with a water challenge. Percent aspiration of water increased at the 9-month study but remained confined to the trachea. At the 12-month postradiation follow-up study, aspiration was seen reaching the bronchi and lungs for both consistencies. The rate of clearing was excellent for liquid aspirate but not for more viscous material. By 15 months after radiation, aspiration had lessened, but it still reached the lungs and was seen for water only.
The patient continued to eat a normal diet throughout the period of study and gained weight after his cancer treatment, and despite his aspiration, pneumonia did not develop. Pulmonary function testing 15 months after radiation therapy showed moderate obstruction with normal lung volumes and normal diffusing capacity for carbon monoxide. He had a normal cough and gag reflex at the time of his testing as a normal control, and he continued to demonstrate an adequate gag and cough reflex after therapy.
There were no swallowing complaints before treatment. After radiation therapy there was some diet alteration because of xerostomia, which led him to need to drink liquid when eating. He reported some difficulty swallowing solids and dry food, with a need for multiple swallows and oral rinse afterward; a feeling of food “sticking” in his throat; coughing when eating; and swallowing better with his chin tucked in and down. These symptoms are consistent with the lowered scintigraphic swallowing efficiency found for the more viscous test material and the increased number of swallows taken for both consistencies.
DISCUSSION
Alterations in swallowing and aspiration are common sequelae after treatment of head and neck cancers, but sub-threshold amounts do not necessarily lead to serious complications or require preventive medical intervention. Multiple factors come into play, including whether the patient is ambulatory, whether the patient has poor pulmonary function, whether the cough has diminished, and whether it is effective. The challenge is how to recognize patients able to eat a normal diet without such complications.
After cancer treatment, especially if surgery was involved, a swallowing therapist is often consulted, and preliminary studies are ordered, including a modified barium swallow or fiberoptic endoscopic evaluation. Aspiration of the test bolus is typically considered to portend a poor prognosis with the fear of development of aspiration pneumonia. When aspiration is suspected, the offending food substance is often restricted from the diet, or the patient's oral intake is restricted and he or she is kept feeding tube dependent. Quality of life is negatively affected by such restrictions.
There are no guidelines for predicting the risk of aspiration pneumonia in a particular patient, and no objective data have been published on the ability to withstand aspiration, especially in patients with adequate cough and gag reflexes. 4 Hamlet et al. 5 have recently reported scintigraphic data on 18 patients with aspiration after radiation therapy, with or without chemotherapy, for treatment of head and neck cancer. Oral nutrition was being maintained by 4 of 6 patients who aspirated into the bronchi or lungs, along with 9 of 12 patients who aspirated only into the trachea on a scintigraphic test using a 10 ml water bolus. The patient described here had his tracheostomy decannulated soon after completion of cancer treatment and demonstrated an adequate cough and gag reflex on clinical examination, which is consistent with his excellent airway clearance data for liquid aspirate.
In the patient described here, aspiration developed over time during the first year after radiation therapy, when late effects of radiation are anticipated to become evident. The aspiration subsequently decreased in amount. This pattern has been noted in several patients tested longitudinally after radiation therapy, 5 which suggests that there may be a period of special vulnerability in the latter half of the first year after treatment.
Scintigraphy can determine not only whether a patient is aspirating but also how deeply the material penetrates into the airways. The rate of clearance in 25 minutes holds promise for identifying those patients best able to tolerate the degree of aspiration they demonstrate. Scintigraphic testing, such as reported here, may aid in selection criteria for patients to be treated conservatively even though known to be aspirating. Such patients might continue to eat while maintaining vigilance for early detection of any adverse change in their status.