
Abstract

Foreign-body aspiration accounts for approximately 3000 deaths per year in the United States. 1 Children between the ages of 6 months and 3 years are particularly susceptible because of their lack of molar teeth and their oral curiosity. 2 Additionally, patients older than 50 years are vulnerable because of denture use, suppressed reflexes, and ingestion of alcohol. 3 Most aspirated foreign bodies tend to get lodged in one of the mainstem bronchi; rarely are they reported to be located in the larynx. 2–4
Hand-held, self-propelled, metered-dose inhalers (MDIs), widely prescribed for the delivery of bronchial therapy, are often used in urgent situations. Because patients may keep them in their pockets, the possibility of inhaling an object inadvertently lodged within the mouthpiece exists. Few reports in the literature describe aspiration of foreign bodies after use of MDIs. 5–12 In each case in which the foreign object was retrieved, it was found in the tracheobronchial tree. We recently treated a patient who had aspirated a foreign body after use of an MDI; however, unlike previous reports, the foreign body was found in the larynx.
CASE REPORT
A 53-year-old man went to an outside hospital because of a mild choking sensation followed by an inability to vocalize. The patient had no stridor or respiratory distress. Lateral- and anteroposterior-directed neck x-ray films revealed a metallic foreign body (Figs. 1 and 2), but the treating physician was uncertain of its exact location. The patient's condition was described as stable, and a working diagnosis of an upper aerodigestive tract foreign body was made. He was transferred to the University of Illinois Eye and Ear Infirmary where, on arrival, he was breathing comfortably but was completely aphonic. Further investigation revealed that he had a history of asthma, for which he used an albuterol inhaler as needed. We learned that his symptoms began earlier that evening after using the inhaler. Physical examination revealed a respiratory rate of 20 breaths/minute, an oxygen saturation level of 99%, new-onset supraclavicular retraction, and mild inspiratory stridor. Auscultation over the trachea revealed turbulent airflow, and flexible nasopharyngoscopy confirmed a coin in the larynx. It was seen in the horizontal plane impacted bilateral into the laryngeal ventricles (Fig. 3); approximately 80% of the airway was obstructed.
The patient was taken emergently to the operating room. Because of progressing respiratory distress, an awake tracheotomy was performed to secure the airway, and the foreign-body penny was removed during laryngoscopy with cupped forceps. The patient was decannulated and discharged on postoperative day 3, with no sequelae. It was later learned that the patient kept his albuterol inhaler in a trouser pocket that contained loose change. He had used it without checking the discharge port and aspirated a penny that had lodged within it.

Anteroposterior-directed x-ray film of a metallic foreign body in the neck.

Lateral-directed x-ray film identifying a metallic foreign body in the horizontal plane.
DISCUSSION
Airway foreign bodies most commonly are found in the mainstem bronchi. Only rarely are they found in the larynx. 2–4 Laryngeal foreign bodies account for 1% to 12% of airway foreign bodies. 2–4,13 Most reports estimate that they account for 4% to 5% of airway foreign bodies retrieved at the time of endoscopy. Lima 13 found a 12% incidence of glottic and supraglottic foreign bodies in a review of all patients who came to the emergency department with a history of a choking sensation.
Patients with a laryngeal foreign body may cough it out, allow it to pass distally, or asphyxiate before medical treatment. A laryngeal foreign body requires emergent attention. The abdominal thrust described by Heimlich in 1975 has proved successful for a large number of choking victims, possibly explaining the decreasing number of fatalities from laryngeal obstruction. 13
Laryngeal foreign bodies are not always lethal. 2–4,13-15 Nonetheless, the largest recent review of laryngeal foreign bodies revealed the potential for grave consequences in patients with true glottic foreign bodies. 13 In this series 5 of 11 patients died, and 3 of 11 had hypoxic encephalopathy. Laryngeal foreign bodies were categorized into two distinct groups. Bulky, irregular, round, or cylindrical bodies that can completely obstruct the airway were associated with severe consequences, including five deaths and three respiratory arrests. Conversely, thin (laminar), triangular objects that can assume a sagittal position in the airway may go unsuspected. They tend to mimic inflammatory diseases such as croup or asthma. These patients are more likely to survive the acute event and seek treatment from an otolaryngologist. Three of 11 patients in this series had thin glottic foreign bodies, and all survived after planned laryngoscopy.
In addition to the type of object, the timing of aspiration during the respiratory cycle may be a strong determinant of the outcome. 13 The inspiratory act takes approximately 2 seconds, and it is during the initiation of this effort, when the pressure in the airways is increasingly negative, that a strong suction force is created. This force may result in impalement of the object into larynx. 13 With limited air volume in the expiratory reserve, there is little force to cough out the object or to be available for the powerful burst generated by the Heimlich maneuver. In contrast, objects that are aspirated at the end of an inspiratory cycle occur after a large volume of air has been inspired and are more likely to be expelled with lifesaving maneuvers. 13
Kent and Watson 14 emphasized the importance of early diagnosis of laryngeal foreign bodies. In their review of four cases, two were delayed in diagnosis. This resulted in a tracheostomy in both patients. One patient survived after a respiratory arrest, but the other could not be revived.
MDIs are ubiquitous in society. They provide immediate relief for bronchospasms and are often carried in accessible places. Loose objects may be stored in the same place, and the inhaler mouthpiece, if not capped, can easily entrap and conceal these objects, placing the patient at risk for aspiration. A few previous reports have described cases of airway foreign bodies (a lid to a makeup pencil, cap of an inhaler, tablets, and coins) after use of an MDI. 5–12
In all these reports the objects aspirated were found in the mainstem bronchi during endoscopy. 5–12 Additionally, laryngeal aspiration has also been suspected after inhaler use, resulting in a choking episode followed by expectoration of an MDI cap. Indirect laryngoscopy revealed left vocal cord edema. 6
Usually the patient realizes that an object has been aspirated, but Bray et al. 5 reported a patient with a delay in diagnosis for a month. A chest x-ray film was taken because of worsened cough and productive sputum, and a coin was identified in the left mainstem bronchus. The author advised physicians to be aware of silent foreign bodies in patients who use MDIs. Other recommended measures to decrease the chance of aspiration have included storing inhalers with the caps in place, checking the mouthpiece before use, and holding the inhaler 4 cm from the mouth during inhalation. 10
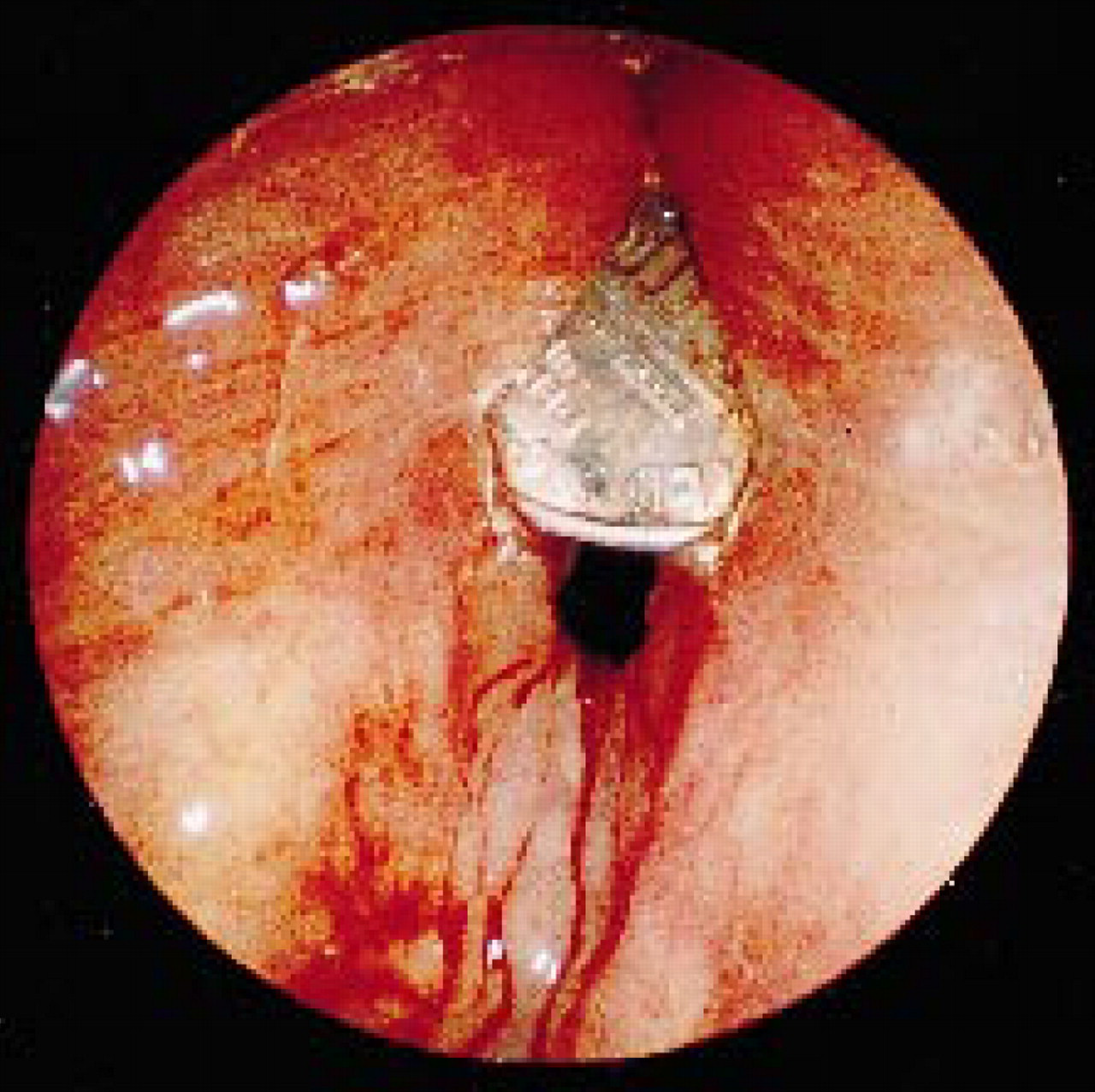
Endoscopic view of the larynx showing a coin lodged in the ventricles bilaterally. Most of the airway is obstructed.
The case that we have presented is unusual because the foreign body was impacted in the horizontal plane within the larynx, resulting in aphonia without initial respiratory distress. In addition, the patient was unaware that he had aspirated an object. This history puzzled the treating emergency department physician, but a prompt diagnosis was made after nasopharyngoscopy. The choice of anesthesia for removal of the foreign body was limited because of the onset of laryngeal edema and progressive stridor. The priority was to secure the airway with an awake tracheotomy before removal of the foreign body.
Anesthetic methods to remove laryngeal foreign bodies have been controversial. Because laryngeal foreign bodies have a great propensity for total airway obstruction, the anesthetic and airway management is critical to successful removal. Cohen et al., 2 in their reference to the management of airway foreign bodies, believed that general anesthesia is contraindicated in cases in which the airway cannot be controlled, specifically laryngeal or tracheal foreign bodies. Kent and Watson 14 believed that paralysis was contraindicated and that assisted ventilation might displace the object. He removed two laryngeal foreign bodies with the aid of a gaseous anesthetic, halothane, whereas the patient maintained spontaneous respirations. Hussain et al. 15 removed a nonobstructing safety pin from the larynx after inducing anesthesia with halothane and nitrous oxide. Anesthesia was maintained with propofol and atracurium while jet ventilation continued oxygenation. There are several anesthetic implications when dealing with the patient who has a laryngeal foreign body. Consideration is given to the presence or absence of a full stomach, which may play a role in the anesthetic technique used to induce anesthesia. It is prudent to lessen the risk of aspiration pneumonitis by the administration of metoclopramide to promote gastric emptying and histamine blockers to decrease gastric pH. In a patient with a laryngeal foreign body who is ventilating adequately, a mask induction with a volatile agent with the patient breathing spontaneously may be the most appropriate; however, because each case is unique, anesthetic management of the patient involves detailed communication between the endoscopist and the anesthesiologist in sharing the airway.
To our knowledge, this is the first reported case of an impacted laryngeal foreign body after use of an MDI. It is imperative that patients be appropriately educated on the proper storage and use of inhalers. In addition, diagnosis must not be delayed. Physicians should maintain an index of suspicion for foreign-body aspiration in patients who report a choking sensation after use of an MDI.